Article Text

Abstract
Background Reducing dietary sodium (salt) intake has been proposed as a population-wide strategy to reduce blood pressure and cardiovascular disease (CVD). The cost-effectiveness of such strategies has hitherto not been investigated in Cameroon.
Methods A multicohort multistate life table Markov model was used to evaluate the cost-effectiveness of three population salt reduction strategies: mass media campaign, school-based salt education programme and low-sodium salt substitute. A healthcare system perspective was considered and adults alive in 2016 were simulated over the life course. Outcomes were changes in disease incidence, mortality, health-adjusted life years (HALYs), healthcare costs and incremental cost-effectiveness ratios (ICERs) over the lifetime. Probabilistic sensitivity analysis was used to quantify uncertainty.
Results Over the life span of the cohort of adults alive in Cameroon in 2016, substantial numbers of new CVD events could be prevented, with over 10 000, 79 000 and 84 000 CVD deaths that could be averted from mass media, school education programme and salt substitute interventions, respectively. Population health gains over the lifetime were 46 700 HALYs, 348 800 HALYs and 368 400 HALYs for the mass media, school education programme and salt substitute interventions, respectively. ICERs showed that all interventions were dominant, with probabilities of being cost-saving of 84% for the school education programme, 89% for the mass media campaign and 99% for the low sodium salt substitute. Results were largely robust in sensitivity analysis.
Conclusion All the salt reduction strategies evaluated were highly cost-effective with very high probabilities of being cost-saving. Salt reduction in Cameroon has the potential to save many lives and offers good value for money.
- health economics
- preventive medicine
- epidemiology
- cardiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study uses the well-established proportional multistate life table Markov model to estimate—for the first time in Cameroon—changes in cardiovascular disease (CVD) incidence, mortality and cost-effectiveness of population salt reduction strategies.
A life-course time horizon is used, which captures the maximum future benefits of preventive strategies while accounting for heterogeneities in CVD risk, such as sex, age and hypertension status.
Intervention and healthcare costs used local unit costs and resource use, making our results highly context-specific and policy-relevant to the ministry of health.
This modelling does not include demographic changes such as migration and fertility likely to influence future population structure.
Introduction
Heart disease and stroke continue to claim the lives of many around the world, together responsible for almost 18 million global deaths in 2017.1 Low-income and middle-income countries (LMICs) are most disadvantaged, with over four-fifths of premature cardiovascular disease (CVD) deaths occurring in these countries. Hypertension is the leading and single largest risk factor for CVD, with over a billion adults worldwide currently affected.2 Pooled estimates from sub-Saharan Africa (SSA) report that about one-third of adults currently have hypertension, with increasingly similar rates in urban and rural settings.3 In Cameroon, recent evidence has shown that about a third of adults have hypertension.4
High dietary salt intake is linked with elevated blood pressure and increased risk of non-fatal and fatal CVD events. This linear relationship has been demonstrated in methodologically robust cohort and interventional studies for both normotensive and hypertensive populations (with steeper gradient in the latter).5 High sodium intake was identified as a leading dietary risk factor for disease burden worldwide in 2017, causing over 3 million non-communicable disease (NCD) deaths and over 70 million disability adjusted life years.6 There is limited empirical evidence in Cameroon on the relationship between sodium and blood pressure. In a recent cross-sectional study in Cameroon, a significant positive linear relationship was observed between urinary sodium excretion (surrogate of intake) and age-adjusted systolic and diastolic blood pressures in rural and urban dwellers.7 Moreover, after adjusting for age, sex, body mass index, alcohol and tobacco use, another study showed that urinary sodium excretion independently predicted elevated blood pressures among adult Cameroonians.8
Evidence from a systematic review and metaregression of salt intakes in SSA showed that most countries have intake levels above the WHO recommendation (<2000 mg of sodium, or <5 g of salt).9 In Cameroon, recent mean salt intake was estimated at around 7.1 g from spot urine,8 which is above global recommendations. Reducing dietary salt intake has been recommended at global and at continental levels as a cost-effective population strategy to reduce blood pressure and CVD burden. Mozaffarian and colleagues estimated that over 1.6 million CVD deaths in 2010 were attributable to sodium consumption above 2000 mg.10 Furthermore, we have shown that achieving the WHO 30% population-wide dietary salt reduction in Cameroon could lead to substantial improvements in population health, with over 700 000 health-adjusted life years (HALYs) gained over the life course of adults alive in 2016, as well as reduce the probability of premature mortality from CVD by almost 17%.11
The majority of sodium in the Cameroonian diet is from discretionary addition during cooking and at table, either as salt itself or in the form of stock cube and sauces.12 13 Data from national household expenditure surveys in Cameroon showed that consumption of salt and other condiments was substantially higher than consumption of sugar, honey and other sweet products; however, this varied by region, with the northern regions consuming less salt and more sugar compared with the southern part of the country.13 Strategies to reduce salt in the diet must therefore be carefully tailored towards its sources. To date, there is no study on the cost-effectiveness of specific salt reduction interventions and for CVD as a whole in Cameroon. Building on the aforementioned literature and previous work, this study aimed to assess the cost-effectiveness of specific salt reduction strategies, which have hitherto not been investigated in Cameroon.
Methods
Study design, perspective and population
A cost-utility analysis was conducted from a healthcare system perspective. A lifetime horizon was used, and the study targeted all Cameroonian adults aged 30 years and above alive in 2016. This age cut-off and group were selected due to the fact that they are the ones most at risk of developing hypertension and related complications that were the focus of the preventive interventions assessed. We used the generalised cost-effectiveness analysis approach as recommended by the WHO and described in detail elsewhere.14 Here, alternative interventions are compared against a ‘do nothing’ scenario. This was consistent with respect to the salt reduction interventions assessed, given that Cameroon currently has no official strategy on salt reduction and more broadly has absence of a functional CVD prevention programme.
Interventions and effectiveness
Three population-wide salt reduction strategies were evaluated, including a mass media campaign (MMC), a school-based education programme to primary school children and their families, and replacing common salt with a salt substitute at the producer/provider level. The inclusion of these interventions was guided by the sources of salt in the Cameroonian diet. Given that majority of the salt in the Cameroonian diet is added at table or during cooking,12 and the low awareness of populations regarding CVD and its risk factors,15 two of the interventions analysed targeted improving consumer awareness (see online supplemental file 1) on the ills of excess salt consumption and its effects on blood pressure and CVD. The salt substitute refers to a switch in the composition of salt consumed (here assumed to apply to just salt and stock cubes), from 100% sodium chloride (NaCl) to a mix of 65% NaCl and 35% potassium chloride (KCl). Reductions in sodium intake from each of the interventions assessed were linked to systolic blood pressure (SBP) reduction using pooled evidence from the literature, and changes in blood pressure were linked to occurrence of CVD. Table 1 provides detailed descriptions of the interventions and their effectiveness.
Supplemental material
Description of interventions, effectiveness estimates and uncertainty assumptions
Intervention and healthcare costs
The WHO NCD-costing tool16 guided our estimation of the intervention costs. Categories of resource use for the MMC and salt-substitute interventions included programme management, health promotion, media and advocacy, training and meetings, rent and office supplies. These were distributed over periods of intervention planning, development, partial implementation and full implementation. In addition to these, for the salt substitute, we estimated the excess cost of switching a proportion of NaCl with KCl based on Cameroon consumption and expenditure data. For the school-based education programme, resource use as detailed in the trial17 guided our intervention costing, and these were scaled up nationwide to involve all public, private (including faith-based) and community schools informed by data from the Ministry of Basic Education.18 Two times per day, to contextualise our analysis and make them most relevant to Cameroon health policy/decision makers, we obtained unit costs of resources such as per diems, staff salaries, transport costs, production of supplies from local sources. For cost offsets, we used data from our prior work that estimated the per-person average annual direct medical costs of ischaemic heart disease (IHD), ischaemic stroke, haemorrhagic stroke and hypertensive heart disease.19 Due to absence of national data on cost of illness in Cameroon, we used health expenditure per capita estimated by World Bank20 to estimate the cost due to unrelated diseases that accrue from life extension due to the interventions modelled. Costs were estimated in local currency (central African francs (XAF)) and converted to US dollars using the average exchange rate of 31 December 2016 (US$ 1=XAF 621.722).21 Where necessary, all costs were adjusted using the World Bank consumer price index for Cameroon.22
Overview of modelling framework
In this analysis, we use a multicohort multistate life table Markov model to estimate the lifetime health outcomes (HALYs) and costs of the adult Cameroonian population aged 30 years and above using 2016 as baseline year. The modelling framework follows three steps.
Modelling exposure (impact of changes in sodium (salt) on blood pressure)
First, we estimate the impact of a change in sodium intake on SBP using evidence from a Cochrane review and meta-analysis23 (see online supplemental file 2 for details). This meta-analysis was used given it included studies which had a minimum intervention duration of 4 weeks, considered relevant when assessing the population health impact of salt reduction interventions. In this meta-analysis, a salt reduction of 4.4 g resulted in 4.18 (3.18–5.18) mm Hg decline in SBP, and for black ethnic populations, the SBP decline was 7.83 and 4.02 mm Hg for hypertensive and normotensive individuals, respectively (see online supplemental file 2 for details).
Supplemental material
Modelling health outcomes (influence of changes in blood pressure on CVD and HALYs)
Second, relative risks of four CVDs (IHD, ischaemic stroke, haemorrhagic stroke and hypertensive heart disease), known to have a strong causal relationship with blood pressure, were obtained from the Global Burden of Disease (GBD) 2016 study.24 Via the potential impact fraction, we explicitly modelled the impact of changes in population SBP distribution on disease incidence (see online supplemental file 2 for details). Each of the diseases modelled has a separate Markov submodel with four states: healthy (alive without CVD), disease (having any of the CVDs), death from CVD and death due to other cause. Movement of proportions of the population between these states is governed by transition probabilities, including incidence hazard (healthy to diseased state), case fatality (diseased to death from CVD) and other mortality probability (movement to death from other cause). Finally, in the disease-specific models, changes in disease incidence lead to change in prevalence and mortality, which then feeds into a population life table. The models have two sections, one containing the population that does not receive the intervention and the second one containing an identical population, which receives the intervention, all of which are stratified by sex and 5-year age groups. The life table (following changes in disease-specific mortality) then explicitly recalculates new mortality probabilities and life years. The life years are adjusted for poor quality of life using weights from the GBD study to calculate HALYs. Differences between the two populations then give estimates of the health impact of the interventions modelled. See supplementary file for additional details. The model structure here was adapted and expanded from previous work conducted at the ACE Prevention programme in Australia.25 26
Cost-effectiveness modelling
Cost-effectiveness analysis was done from a healthcare system perspective. In the base case analysis, all costs and health outcomes were modelled over the remaining life course of the population, with 2016 as baseline year to determine the incremental cost-effectiveness ratio (ICER) while applying a discount rate of 3%. Given the absence of set discount rates for Cameroon, the choice of discount rates is in conformity with economic evaluation recommendations.27
Given the pluralistic nature of data sources, we attempt to quantify their uncertainty by setting plausible distributions to parameters like intervention effectiveness estimates (normal distribution), change in SBP due to salt reduction (normal distribution), relative risk of CVD from change in SBP (log-normal distribution), intervention and healthcare costs (gamma distributions). A probabilistic sensitivity analysis using Monte Carlo simulations (2000 iterations) implemented using Ersatz software28 was conducted to estimate the 95% uncertainty intervals around HALY and cost outcomes. Given the absence of willingness to pay threshold for Cameroon, we adopted the WHO approach of multiples of gross domestic product (GDP per capita for Cameroon 2016: US$1391.75) to determine the probability of cost-effectiveness for the modelled interventions based on their ICERs.14
Sensitivity and scenario analysis
In the sensitivity analysis, we evaluated costs and health outcomes over different time horizons: 10 years (2025), 15 years (2030) and 30 years (2045). We also evaluated other scenarios, including varying the discount rates to 0% and 5%, and assessed ICERs using only intervention costs and a scenario using net costs (ie, including cost offsets and costs due to unrelated diseases in added life years to the future). Other scenarios explored included varying the rate of decay in intervention effect, as well as alternative sodium–SBP relationships.
This study adhered to the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Consolidated Health Economic Evaluation Reporting Standards (CHEERS) guideline for good reporting practices.29
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient-relevant outcomes or to interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
Effects on SBP and hypertension prevalence
The modelled interventions reduced SBP by 0.17–1.37 mm Hg and 0.15–1.23 mm Hg in normotensive men and women, respectively. In hypertensive people, SBP reductions ranged from 0.34 to 2.66 mm Hg and from 0.28 to 2.39 mm Hg for men and women, respectively. These SBP changes translated to reductions in prevalence of hypertension by 0.3%–2.5% in men and 0.2%–2.1% in women. The greatest reductions were for the salt-substitute intervention and the least reductions were with the mass media campaign (table 2).
Estimated changes in systolic blood pressure and prevalence of hypertension by interventions modelled
Effects on CVD incidence and mortality
Over the remaining lifetime of adult Cameroonians, implementation of the MMC could prevent over 9000 new cases of IHD, over 6000 new cases of ischaemic and haemorrhagic strokes and over 2000 hypertensive heart disease (HHD) cases. In addition, about 5000 IHD deaths, over 4000 stroke deaths and over 1000 HHD deaths could be averted. The school education programme could lead to a reduction of over 69 000 incident IHDs, over 50 000 strokes and 17 000 HHD cases over the remaining lifetime of adults. With respect to mortality, over 38 000 IHD deaths, over 32 000 stroke deaths and about 9000 HHD deaths could be postponed or averted. If reduced sodium salt substitutes were used in place of common salt, the model projects that more than 73 000 new cases of IHD, 53 000 new cases of ischaemic and haemorrhagic stroke and over 18 000 new cases of HHD could be prevented over the life course of the adult population. Corresponding reductions in mortality are 40 000, 34 000 and 9000 for IHD, both forms of stroke and HHD, respectively (table 3).
Averted new cases and deaths from cardiovascular disease for modelled salt reduction interventions over the remaining life course of the adult population in Cameroon, 2016
Effect on HALYs, costs and cost-effectiveness
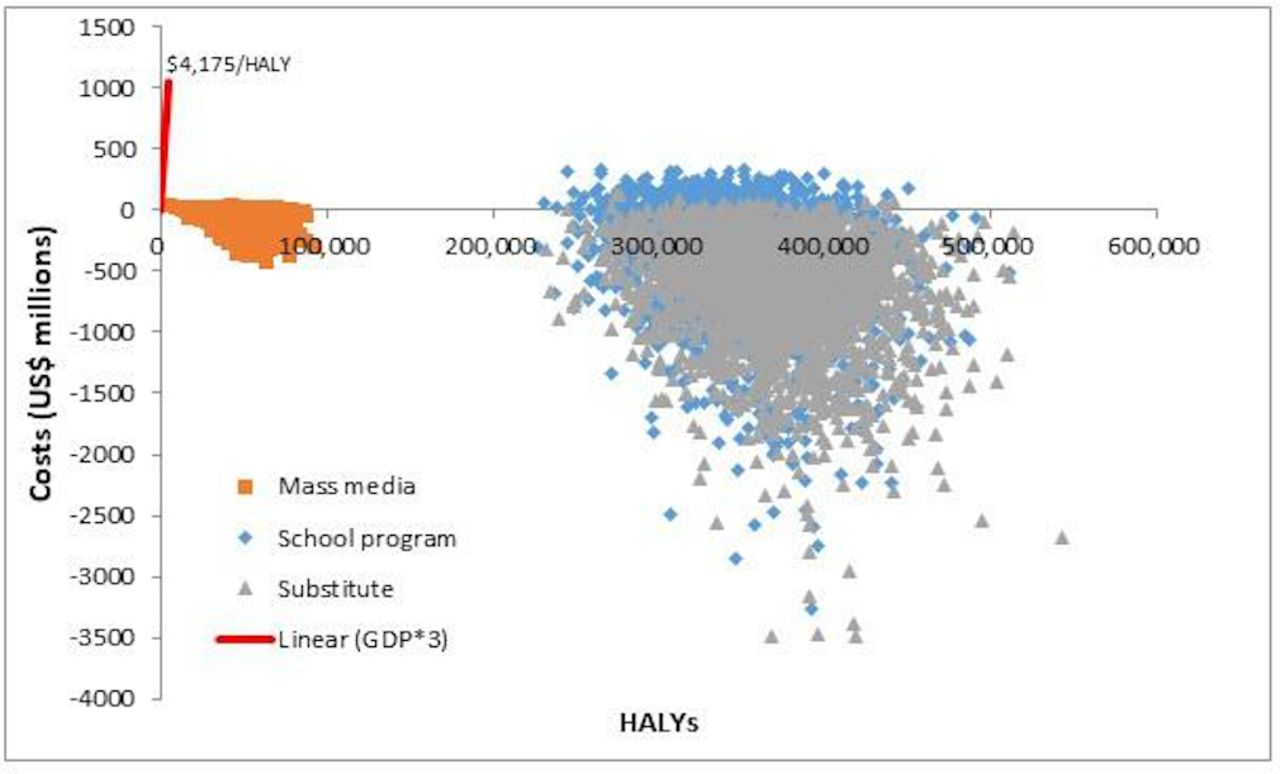
In the base case analysis, implementing the MMC could yield 46 700 HALYs over the life course at a cost of US$37.1 million. When only intervention costs are considered, the MMC was found to be very cost-effective at US$802 per HALY. However, when net healthcare costs (taking into account cost offsets and costs of future unrelated disease) were considered, the intervention was dominant, with an 89% probability of being cost-saving and 100% probability of being very cost-effective, that is, less than GDP per capita.
The school education programme was projected to gain 348 800 HALYs and would require US$370 million for implementation over the lifetime. This translates into an ICER of US$1076 per HALY gained, and when net healthcare cost were accounted for, the intervention became dominant with an 84% probability of being cost-saving and 100% of being very cost-effective.
Switching from common salt (100% NaCl) to a salt substitute with reduced sodium (65% NaCl) would cost about US$174.7 million over the life span and could gain 368 400 HALYs. This intervention was very cost-effective (US$481 per HALY gained) if only intervention costs were considered and was dominant when net healthcare costs were taken into account with 99% probability of being cost-saving (tables 4 and 5 and figure 1).

Cost-effectiveness plane showing cost-effectiveness of salt reduction interventions compared with ‘do-nothing’ scenario.

{kind=link}
{kind=link}
Cost-effectiveness acceptability curves depicting the probability of being cost-effective for the three salt reduction interventions in base case analysis and varied time horizons compared with doing nothing. The green vertical lines represent the 1×GDP per capita threshold while the red vertical lines represent the 3×GDP per capita threshold. GDP per capita (2016)=US$1391.75. GDP, gross domestic product.
Population health, intervention costs and their cost-effectiveness over different time horizons
Probability of salt reduction interventions being cost-effective or cost-saving
Sensitivity analysis
As expected, health gains reduced with high discount rates (5%) compared with undiscounted outcomes, and shorter (10 years) time horizons compared with longer—30 years. Nevertheless, results of cost-effectiveness were largely robust—staying dominant or very cost-effective. However, the probability of being cost-saving appeared to (progressively) reduce with shorter time horizons and higher discount rates compared with undiscounted results. Varying the intervention decay and sodium–blood pressure relationship increased the uncertainty in the ICERs, but mostly remained cost-saving and very cost-effective—less than one times the GDP (for salt substitute), and ranged from dominant to cost-effective (less than one to two times the GDP) for the media campaign and school programme (see figure 2 and online supplemental file 2).
Discussion
Principal findings
Our evaluation of three population-wide salt reduction interventions for CVD prevention shows that these interventions not only could result in substantial health gains, that is, reducing incident CVD and related deaths, but also are very cost-effective. When future net healthcare costs are taken into account, the interventions have very high probabilities of being cost-saving, ranging from 85% to 99% compared with doing nothing over the remaining life course of adult Cameroonians. Even after multiple scenario/sensitivity analyses, our findings were largely robust. Health impacts and probabilities of being cost-effective or cost-saving were greatest for the reduced sodium salt substitute’s intervention followed by a school-based education programme targeting children (with their families) and least for MMC.
Comparison with other studies
In a global cost-effectiveness analysis of government-led salt reduction policy that included industry agreements to reduce sodium content of processed foods and a public health campaign, authors found that such a policy over a 10-year time horizon was highly cost-effective, with ICERs in almost all countries reported at less than the GDP per capita.30 There is limited evidence from individual countries in Africa regarding economic evaluation of salt reduction strategies. In South Africa, the government recently legislated to reduce nationwide salt intakes, among others by reducing salt in processed foods and via media campaigns to reduce discretionary salt use.31 Watkins and colleagues, in an extended cost-effectiveness analysis evaluating this salt policy, found that in addition to resulting in large healthcare savings to the South African government, this salt policy could save households over US$4 million in out-of-pocket expenses, as well as prevent 2400 cases of catastrophic health expenditures annually.32
Several modelling studies, mostly out of Africa, have evaluated the health and economic impacts of various salt reduction interventions, in which majority were found to be cost-saving or very cost-effective.25 33 34 For example, Mason et al modelled the impact of health promotion campaign, labelling food packaging and mandatory reformulation across four Eastern Mediterranean countries. Compared with ‘no policy’, these interventions over a 10-year time horizon were found to be potentially cost-saving and resulted in substantial gains in life years, especially when combined.34 Among the three interventions they assessed, the health promotion campaign had comparatively lower health and economic gains, which is somewhat on par with our analysis. However, in their healthcare costs estimates, the authors did not take into account future costs due to other unrelated disease, which may have inflated their estimate of the benefits.35 Nevertheless, other studies that accounted for these costs still found the majority of population salt reduction interventions were highly cost-effective or dominant.25 33
Studies evaluating pharmacological strategies for CVD prevention reported mixed results. The polypill was shown to be highly cost-effective in LMICs.36 In Tanzania, pharmacological strategies were cost-effective for individuals at moderate or high CVD risk; however, for individuals at low CVD risk, with or without diabetes, medical management was not cost-effective.37 In a study from Ethiopia, most pharmacological interventions assessed for treatment of CVD events were not cost-effective. Similarly, for primary prevention, treatment for elevated cholesterol (at >6.2 and >5.7 mmol/L) and high blood pressure (>160 and >140 mm Hg) were not cost-effective. Treatment following the absolute risk approach was mostly cost-effective, with the lowest ICERs for those with greater than 35% 10-year CVD risk. These results were, however, sensitive to different willingness to pay thresholds (with higher thresholds improving the cost-effectiveness of these interventions).38 Taken together, these findings on the cost-effectiveness of salt reduction strategies and pharmacological interventions for CVD bring to context Geoffrey Rose’s perspective. He advocated that interventions that shift the risk factor distribution of whole populations were likely to result in larger population health gains compared with interventions targeting just the high-risk individuals.39
Strengths and limitations
This study had a number of weaknesses. Our model does not include changes in population demographics and fertility rates over time. In addition, trends in disease incidence or mortality were not accounted for in the model. Forecasts from the GBD suggest that between 2016 and 2040, age-standardised mortality rates for IHD and stroke in Cameroon could decline annually by 0.58% and 1.37%, respectively, while HHD rates increase by 0.15% annually. In their worst-case scenario, IHD and HHD mortality rates were projected to increase annually by 0.65% and 1.78%.40 Furthermore, high blood pressure and high body mass, which strongly influence incidence of CVD, were projected to worsen by 2040. Therefore, it is likely that these trends in IHD and stroke could reduce our modelled health gains, while the projected increasing trends in HHD, blood pressure and BMI could increase them, the balance of this future trends being unclear. Second, we rely on salt consumption data obtained in 2010 for our modelling. It is highly likely that these may have changed (increased) a decade later, given the current growth in urbanisation and accompanied nutrition transition, with worsening dietary patterns such as increasing sugar and energy-dense food consumption41 reportedly related with high salt intake.42 Third, in our base analyses, we assume full intervention effects (and costs) over the lifetime, which could seem unrealistic. However, in sensitivity analyses, we test alternate scenarios limiting the intervention effect to the first 20 years and then decay of 50% for the remaining lifetime and another with zero benefits after 20 years (but maintain full costs throughout the life course). In addition to applying higher discounting, which further penalises future benefits, we also modelled scenarios with a shorter time horizon of 10 years. As expected, there were proportionate reductions in health outcomes and costs, but ICERs were largely robust to these alternative assumptions. Fourth, other diseases that are linked to excess salt intake, such as gastric cancer, osteoporosis and kidney disease, were not modelled. This was mainly because the causal evidence linking them to salt is not as strong as that for CVD. While this omission suggests that our modelled population health gains are probably underestimated, implying the interventions are likely even more economically attractive than currently presented, some of these benefits could be balanced by the harmful effect of potassium-rich salt substitutes on people with chronic kidney disease. Fifth, the school education intervention modelled here is based on cluster randomised trial evidence from China. This study reported both absolute and relative salt reductions for children and for adults. Even though most of the salt in the Chinese and Cameroonian diets are discretionary or added at table or during cooking, the differences in culture and baseline salt consumption levels between the two countries made it seem more reasonable to apply the relative intervention effect. This effect was scaled to the general adult population, and we recognise that some adults in the population do not have children. However, we anticipate that the overall impact of this assumption might have been attenuated by the non-inclusion of adults who were less than 30 years old. Finally, our modelling focused on those 30 years old and above. Given that we model into the future (lifetime), younger populations are likely to age out 30 years and more into the future. Not including them similarly indicates our modelled health gains are conservative and would have reduced our ICERs, making the interventions more economically attractive.
This study also has number of strengths. First, contrary to previous salt modelling studies that have focused on just coronary heart disease and all stroke, we explicitly modelled both major forms of stroke separately, given their varied relationship with blood pressure, as well as modelled HHD that has seldom been modelled. Second, most of the input data, especially on risk factors, was obtained locally for direct applicability of findings. In addition, intervention and healthcare costs used an ingredients approach to estimate total costs using local unit costs and resource use, which made our results more context-specific and policy-relevant to the Ministry of Health. Third, our modelling approach accounts for certain heterogeneities such as sex, age and hypertensive status, for which CVD risk differs. In addition, we test multiple scenarios and sensitivity analyses to ascertain the robustness of our study results. Finally, this study is the first of its kind from Cameroon and contributes to the very scant evidence from Africa on the cost-effectiveness of salt reduction interventions for CVD prevention.
Implications for policy and future research
We have evaluated just three salt reduction strategies. While this may seem interesting, there is a need for the evaluation of other salt reduction strategies such as a salt tax for foods high in sodium content, evaluation of the impact of reducing salt in specific foods such as bread, which also constitute important sources of salt in the diet. Second, future studies should also consider broader health and distributional or equity (by socioeconomic status, rural vs urban) impacts, as well as financial risk protection afforded by health policies. Third, there is a need for evaluation of interventions for other risk factors for NCDs such as physical activity, smoking, alcohol and body mass, as suggested in the broader WHO best-buys. This would provide more evidence for policy makers to decide on the optimal mix of interventions for NCD prevention.
In this study, we use a healthcare system perspective; future studies should consider using a wider societal perspective. There is evidence that productivity costs due to CVD mortality is likely to lead to significant economic returns from investment in preventive health.43 This may provide additional information for policy makers as they grapple with resource allocation decisions. The interventions modelled may not be an exhaustive list, and given most of the salt in the diet is discretionary especially added during cooking, and acknowledging the challenge of changing behaviours, health policy makers may consider implementation of low-sodium salt substitutes. This requires no conscious behaviour change on the part of the consumer; hence, it is likely to be sustainable and has the largest health gains with almost 100% probability of being cost-saving. These economic returns could be reinvested in other much needed health interventions or invested in other non-health sectors. These may, however, need to be evaluated in the context of political feasibility and budget impact.
Conclusion
This study provides modelling evidence of the potential cost-effectiveness of population-wide salt reduction interventions in Cameroon, which has hitherto been unknown. While there is need for country-specific evidence, our findings could potentially be extrapolated to other SSA and LMICs where the consumer adds the majority of salt in the diet. While all interventions were highly cost-effective with about 85%–100% probability of being cost-saving, LSSSs had the largest health gains and highest probability of being cost-saving. This could be considered among the priority strategies for salt reduction in CVD prevention in LMICs as countries work towards meeting the WHO target of a 30% relative reduction in population salt intake.
Acknowledgments
We are grateful to Jan Barendregt for developing previous iterations and model frameworks adapted and expanded in this current analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @l_aminde, @lennertveerman
Contributors LNA conceived the study, did the modelling analysis and wrote the first version of the manuscript. LC and JLV contributed to analysis and interpretation of findings and reviewed successive versions of the manuscript. All authors critically reviewed the manuscript and approved the final version for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Detailed data and results over different time horizons of the results and sensitivity analyses are reported in the paper and supplementary files. Authors, via the corresponding author, welcome other reasonable requests for additional information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.