Article Text

Abstract
Introduction Lifetime prevalence of shoulder pain is 70%, and approximately 50% of people with shoulder pain will experience pain for more than a year. Rotator cuff-related shoulder pain (RCRSP) is the most common shoulder condition and the main non-surgical intervention is exercise therapy. For approximately 30% of people with RCRSP, this approach does not lead to a significant reduction in symptoms. This may be due to an inappropriate dosage or choice of exercises. The aim of this investigation is to compare the short, mid and long-term effects, in terms of symptoms, functional limitations, kinesiophobia and pain catastrophising, of three different shoulder rehabilitation approaches (education, strengthening, motor control) in adults with RCRSP.
Methods and analysis In this single-blind (assessor), parallel-group, randomised clinical trial, 123 adults presenting with RCRSP will take part in a 12-week rehabilitation programme. They will be randomly assigned to one of three groups (education only, strengthening approach or motor control-focused approach). Abbreviated version of the Disabilities of the Arm, Shoulder and Hand Questionnaire, the primary outcome, Western Ontario Rotator Cuff Index and Brief Pain Inventory will evaluate symptoms and functional limitations, while Tampa Scale of Kinesiophobia and Pain Catastrophizing Scale will evaluate pain-related fear and catastrophising at baseline and at 3, 6, 12 and 24 weeks. Ultrasonographic acromiohumeral distances and tendon thickness will be assessed at baseline and 12 weeks. Intervention groups will be compared on outcomes with intention-to-treat analyses using two-way repeated measures analysis of variance if the data are normally distributed or non-parametric analysis of longitudinal data if they are not.
Ethics and dissemination Ethics approval was obtained from the Sectorial Rehabilitation and Social Integration Research Ethics Committee of the Centre Intégré Universitaire de Santé et de Services Sociaux de la Capitale Nationale (CIUSSS-CN). Results will be disseminated through international publications in peer-reviewed journals, in addition to international conference presentations.
Trial registration number NCT03892603; pre-results.
- elbow & shoulder
- musculoskeletal disorders
- shoulder
- rehabilitation medicine
- sports medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This randomised controlled trial directly compares three of the most widely used interventions for rotator cuff-related shoulder pain (education, strengthening and motor control exercises) to highlight the most efficient and guide shoulder rehabilitation.
Effects on symptoms, kinesiophobia, catastrophisation, acromiohumeral distance and tendon thickness of different exercise programmes as well as education will be analysed.
Methods to reduce the risk of bias will be implemented throughout the study, which includes a statistically justified sample size, blinding, randomisation and adequate concealment of group allocation for the assessors.
Patients will be blinded to the treatment provided to the other groups as it is not feasible to completely blind the participants and the treating therapist due to the nature of the allocated treatments.
A true control group (wait-and-see approach) will not be included as it would be difficult to maintain a high retention and avoid cointerventions during the mid-term and long-term follow-up.
Introduction
Shoulder pain is one of the most frequent musculoskeletal (MSK) complaints in the general population with a lifetime prevalence of up to 70%.1 The overall prognosis is highly variable, with up to 50% of patients still reporting persistent pain 6–12 months after seeking an initial primary care consultation.1 Rotator cuff-related shoulder pain (RCRSP), a broad term that includes rotator cuff tendinopathy, tendinitis, tendinosis, partial and atraumatic full-thickness rotator cuff tears, impingement and subacromial pain, accounts for 50%–85% of diagnoses for shoulder pain.2
Several interventions are available for RCRSP such as education, exercise, manual therapy, electrotherapy, injection, medication and surgery. Clinical trials suggest that the long-term outcomes of patients pharmacologically or surgically treated are comparable to those receiving rehabilitation.3–6 Regardless of modality, treatment is unsuccessful for more than one-third of patients who continue to have pain and disability following care.7 Several reasons may explain this lack of effectiveness and include psychosocial factors (including kinesiophobia7 and pain catastrophising8), occupational factors, lifestyle factors,9 lack of adherence to the exercise programme,3 low expectations regarding recovery and low levels of self-efficacy.4 5 Other reasons behind this lack of success might be inadequate choice of exercise.
Education and exercises are two of the most frequently used interventions for RCRSP with evidence supporting their effectiveness.6 10 11 Patient education often constitutes the first management strategy in health-related conditions as it does not necessitate extensive resources and is available to all. It helps reduce false beliefs and fears related to the pathology as well as increase patient’s knowledge of their condition in order to improve their self-efficacy.6 However, education alone might not be sufficient for all patients, as some may present deficits such as muscular weakness or inhibition, altered shoulder muscle recruitment patterns and kinematics.12 13 These deficits might explain the persistence of symptoms in some patients. Recent systematic reviews strongly recommend with low to moderate quality evidence that exercises be prioritised as a first-line intention treatment since it presents better outcome on pain and function than placebo or wait-and-see.14 15However, we still do not know which types of exercise are better and thus lead to better outcomes.13 There is even some evidence in the literature suggesting that some types of exercise may not be more effective than a placebo.16 17 These findings highlight the need for higher quality studies evaluating the effect of different exercises for RCRSP.
Motor control exercises have been shown to reduce pain and disability in individuals with RCRSP.10 One rationale behind these effects is that improving muscle recruitment patterns and kinematics could prevent the compression of the subacromial soft tissues underneath the coracoacromial arch as the arm elevates.12 Apart from this potential explanation that is still debated,2 efficiency of motor control exercises might reside in the reduction of fear-avoidance behaviour or pain catastrophising as the patients are encouraged to move in previously feared positions.18 It could also have a direct neurophysiological central effect on pain-related brain areas, similar to the one observed with manual therapy,19 20 and bring change in pain sensitivity and sensorimotor processing. On the other hand, by progressively loading contractile tissue, strengthening exercises have been shown to decrease pain and muscle weakness.11 This could be the result of an increased capacity by the tendon to sustain load or to a decrease in rotator cuff tendon inhibition.21
Although their clinical usefulness has already been assessed separately,22 23 no study has directly compared those three interventions for the management of RCRSP in order to better highlight recovery over time as well as the choice of intervention provided. Identifying the most effective and efficient intervention(s) for RCRSP is of paramount importance to prevent symptoms persistence, limit healthcare costs associated with these disorders and all resulting consequences.
Objective and hypotheses
The primary objective of this randomised controlled trial (RCT) is to compare the short, mid and long-term effects of three different approaches (education, strengthening, motor control) of delivering shoulder management on the symptoms and functional limitations of individuals with RCRSP. A secondary objective is to explore the effects of the programmes on shoulder control (acromiohumeral distance (AHD)), subacromial structures (supraspinatus (SS) and infraspinatus (IS) tendon thickness), kinesiophobia and catastrophisation related to shoulder pain. The hypothesis is that both exercise groups will demonstrate a better outcome in pain and function compared with the education group. The motor control programme should lead to a quicker improvement in symptoms and functional limitations than the strengthening programme because, by improving muscle recruitment patterns, it will decrease control deficits and thus lower the odds of individuals experiencing pain. Its effect on kinesiophobia should also contribute to a quicker reintegration of movements into patients’ life, hence improve function. Finally, all groups should lead to a decrease in kinesiophobia and pain catastrophisation, but the motor control and strengthening groups should lead to a greater reduction since participants will be guided to move in amplitudes that were previously limited by pain or pain-related fears or perform near-maximal intensity muscle contractions.
Methods and analysis
Study design
This single-blind, parallel-group RCT will include five evaluation sessions over 24 weeks (baseline, 3, 6, 12 and 24 weeks), six intervention sessions over 12 weeks for both exercise groups and two education sessions over 12 weeks for the education group (figure 1). All participants will take part in the baseline evaluation. They will complete self-administered questionnaires on sociodemographic characteristics, symptomatology, comorbidities, functional limitations, kinesiophobia and pain catastrophising using self-reported questionnaires. Then, ultrasonographic (US) measurements of the AHD and of the SS and IS tendon thickness will be conducted. Thereafter, participants will be randomly assigned to one of three intervention groups, and take part in their assigned programme. All study outcomes will be reevaluated at 12 weeks, while the self-administered questionnaires will also be readministrated at 3, 6 and 24 weeks using web-based questionnaires. A global rating of change question will be completed at 3, 6, 12 and 24 weeks. The study will be conducted at the Centre interdisciplinaire de recherche en réadaptation et en intégration sociale. This RCT is registered on ClinicalTrials.gov and the Standard Protocol Items: Recommendations for Interventional Trials checklist was used when writing the protocol.24
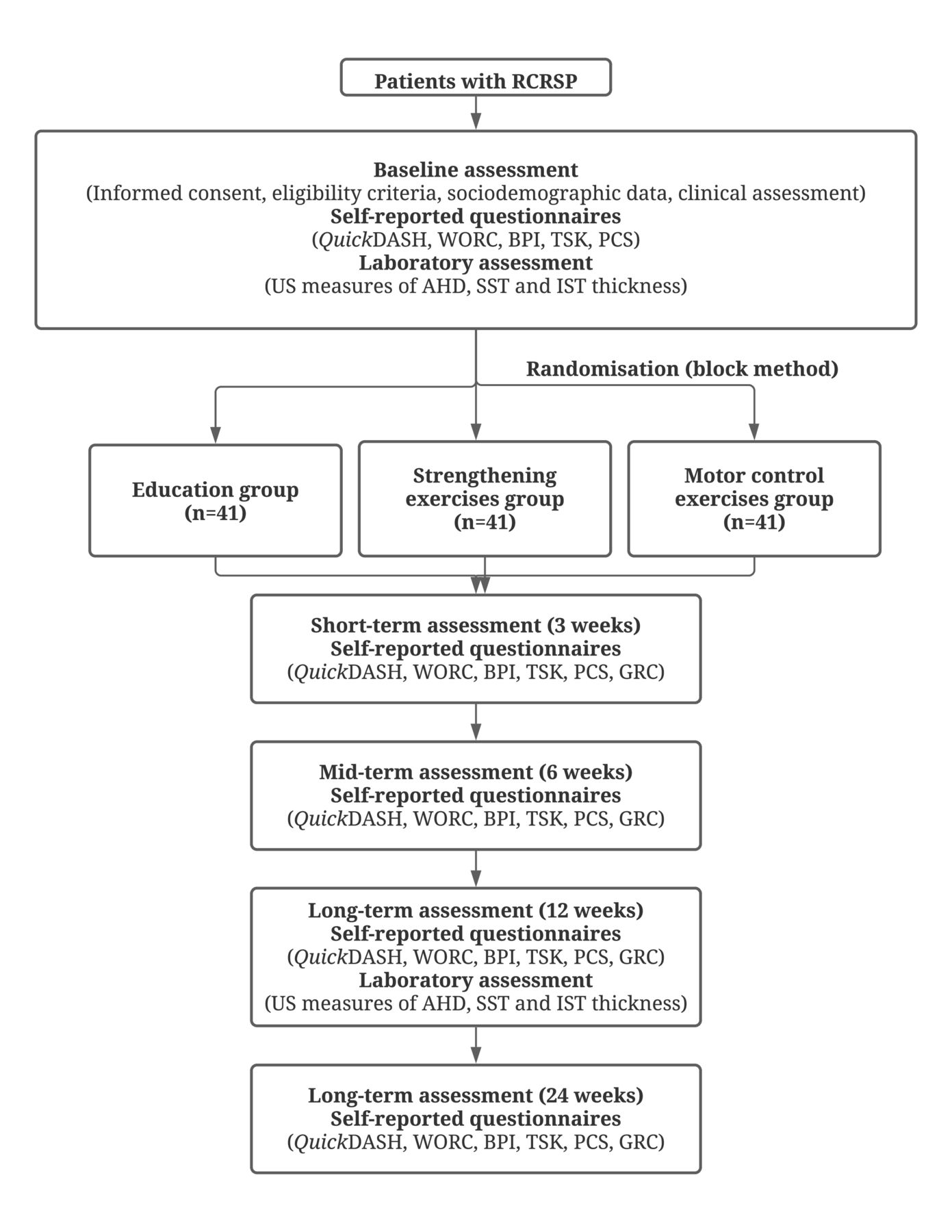
{kind=link}
Schematic diagram of the study design. AHD, acromiohumeral distance; BPI, Brief Pain Inventory; GRC, global rating of change; IST, infraspinatus tendon; PCS, Pain Catastrophizing Scale; QuickDASH, abbreviated version of the Disabilities of the Arm, Shoulder and Hand Questionnaire; RCRSP, rotator cuff-related shoulder pain; SST, supraspinatus tendon; TSK, Tampa Scale of Kinesiophobia; WORC, Western Ontario Rotator Cuff Index.
Participants and sample size
Adults presenting with RCRSP will be recruited using the following inclusion criteria: (1) 18–75 years of age, (2) symptoms lasting longer than 3 months, (3) presence of a painful arc in flexion or abduction, (4) presence of a positive Neer sign or Hawkins-Kennedy Test, (5) presence of pain when resisting humeral external rotation or abduction, or positive Jobe Test, and (6) ability to speak English or French. A positive cluster of criteria 3, 4 and 5 represents an adequate diagnostic tool for RCRSP (sensitivity: 0.75, specificity: 0.74).25 Participants will be excluded if they present any of the following criteria: (1) clinical signs of massive rotator cuff tears as defined by presence of gross weakness in the absence of limited pain, (2) other shoulder disorders, for example, adhesive capsulitis (restriction of passive glenohumeral movement of at least 30% for two or more directions), severe osteoarthritis, fracture, dislocation, severe acromioclavicular joint pathology, (3) previous shoulder surgery, (4) presence of significant comorbidity, for example, neurological disorders, rheumatoid arthritis, (5) current or past carcinoma, (6) unlikely to be able to perform required clinical assessment tasks or attend the required evaluation and intervention sessions, (7) symptomatic cervical spine pathology, defined as reproduction of symptoms with active physiological cervical spine movements, and (8) corticosteroid injection in the last 6 weeks. All recruited participants will be evaluated by a physiotherapist (PT) in order to confirm their eligibility.
Based on our sample size calculation, calculated for our primary outcome (abbreviated version of the Disabilities of the Arm, Shoulder and Hand Questionnaire (QuickDASH)), 41 participants are required per group (G*Power V.3.1.9; effect size: 0.80, α=0.05, power=0.95, SD=13 DASH points, clinically important difference (CID)=11 DASH points, expected lost at follow-up=15%). Therefore, 123 participants with RCRSP will be recruited. This sample size should be sufficient to detect a CID between groups.
Potential participants will be recruited in outpatient physiotherapy clinics of hospitals and in private physiotherapy clinics in the Quebec City region, and through electronic mailing lists of employees and students at Université Laval (>52 000 individuals). Since our research team has performed studies evaluating the same population in the same metropolitan area, we are confident to recruit the targeted population.26–28 With an average rate of seven new participants per month, we estimate that 18 months will be ample time to reach our goal of 123 participants.
Randomisation and blinding
A randomisation list has been generated prior to the initiation of the study by an independent research assistant not involved in data collection using a random number generator. Allocation is concealed in sealed and opaque envelopes that are sequentially numbered. Randomisation was stratified to ensure balance of the treatment groups with respect to sex (male/female) and age (18–55/55–75). A blocked randomisation was also used to make sure that three equal groups of 41 participants will be obtained (random blocks of 3, 6 or 9). Given that it is impossible to blind the treating PT and participants, a single-blind design will be used. To reduce potential contamination bias, the three programmes will be given at different time periods. Further, participants will be instructed not to discuss their group assignment, exercises performed or advice received with other potential participants and with the evaluator. To evaluate the effectiveness of blinding at the 3-month follow-up, the evaluator will answer the following question: What intervention do you think the participant received?; with one of the following answers: (1) education and advice, (2) strengthening, (3) motor control, or (4) no idea. If they answer 1, 2 and 3, they will have to explain why they think the participant received this intervention.
Interventions
Advice and education programme
During two education sessions of 30 min each, participants will be given written information by a PT about the shoulder (anatomy and function), basic pain science and will be directed to watch a series of six educational videos on shoulder pain and function, persistent pain, physical activity, stress, sleep and eating habits. For each video, they will have two questions to answer: (1) What was the most important message? and (2) Was there anything you didn’t understand in the video? The comprehensive written information includes advice on:
The shoulder and their condition.
The relevance of pain.
Pain management (night and day).
Activity modification (when to increase and decrease).
Reassurance.
Shoulder muscle strengthening programme
In addition to the same advice and education the control group receives, participants from this group will be given a shoulder progressive strengthening exercises programme (online supplemental file 1) based on one-repetition maximum (RM) that will involve concentric and eccentric contractions with free weights and resistance elastic tubes. Exercises will target humeral internal/external rotators and abductors and the scapular muscles (protractors, retractors, elevators and depressors). Number of repetitions will be one set of the maximum number of repetitions until muscular exertion or until pain reaches 3/10. If the pain level is 3/10 or more at rest, participants will be asked to start with a lower number of repetitions and increase or decrease depending on their pain behaviour in the following hours and the next day. Participants will be asked to complete the exercises every day for 12 weeks. At each session with the PT (six over a 12-week period), shoulder movements and strength will be reassessed, and the programme will be progressed accordingly. The necessary equipment (dumbbells, elastic bands) will be provided to the participants. Any questions or concerns will also be addressed by the treating PT, and participants will be requested to complete a daily diary of their exercise adherence.
Supplemental material
Motor control and functional rehabilitation exercise programme
Participants will receive the same advice and education as the other groups as well as a motor control exercises programme (online supplemental file 2). Each session with the PT (six over a 12-week period) will start with a pain neuromodulatory (motor control) technique in order to look at the influence of different corrections to alleviate symptoms during upper limb movements. A series of quick clinical tests will be conducted taking no more than 3 min. The tests will be performed in a sequential format through three key areas: thoracic ‘finger on sternum technique’, scapular facilitation and ‘humeral head’ procedures.29 30 If a technique reduces pain, that technique will then be performed as exercises and incorporated into the participant’s functional movement. In addition, motor control exercises during arm elevation, progressed through a standardised six-phase retraining sequence, will be executed.26 31–33 Retraining phases will be graded according to: (1) resistance applied to the shoulder; and (2) use or non-use of feedback. Once participants have reached pain-free execution, the programme will be progressed into re-education exercises according to the participants’ work, sports and activities of daily living and incorporate a series of functional activities involving the whole body. Number of repetitions will vary from one to three sets of 10–30 repetitions. Participants will be asked to complete the exercises every day. The necessary equipment (dumbbells, elastic bands) will be provided to the participants. Participants will be requested to complete a daily diary of their exercise adherence.
Supplemental material
Both exercise groups will be given information about pain related to the execution of their exercise programme (online supplemental file 3).
Supplemental material
Data collection
An evaluator blinded to group assignment will perform all evaluations according to standardised procedures.
Symptoms and functional limitations will be evaluated using the QuickDASH (generic questionnaire assessing any upper limb disorders), the primary outcome, as well as two other validated self-reported questionnaires: Western Ontario Rotator Cuff Index (WORC; specific to RCRSP) and the Short Form of Brief Pain Inventory (BPI-SF). The QuickDASH is a self-reported questionnaire that includes 11 items measuring physical disability and symptoms of the upper extremity. It presents excellent reliability, is responsive to change, has a minimal detectable change (MDC) and CID around 11%.34 The WORC is a disease-specific questionnaire developed to measure pain, function and health-related quality of life of individuals suffering from RCRSP. It contains 21 items divided into five sections: physical symptoms, sports/recreation, work, lifestyle and emotions. It has demonstrated excellent reliability, is responsive to change for patients with RCRSP, has an MDC around 12% and a CID varying from 12% to 13%.35 Finally, the BPI-SF is a validated questionnaire used to assess the intensity of pain and the interference of pain on the patient’s life. It has shown to be reliable, internally consistent over time and valid with several musculoskeletal populations including RCRSP.36
Pain-related fear and catastrophising: The Tampa Scale of Kinesiophobia (TSK) is a self-administered questionnaire that measures beliefs and behaviours related with pain, specially focusing on beliefs that pain is damaging and painful movements should be avoided.37 The psychometric properties of the TSK have been confirmed for different pain disorders.38 The Pain Catastrophizing Scale is a self-administered questionnaire measuring the range of catastrophic thoughts and feelings (magnified threat, ruminating thoughts and feelings of helplessness) associated with pain that individuals may experience. High internal reliability has been reported in patients with chronic pain with adequate validity and test–retest reliability.39
US measurement of AHD and SS and IS tendonswill be assessed with a 12 MHz linear array probe (Logic e9, GE Healthcare, Milwaukee, Wisconsin, USA). US images of AHD will be obtained with the participants seated in a standardised position with the arm at rest and at 60° of active abduction. US measures will be obtained by placing the transducer on the anterior aspect of the lateral surface of acromion along the longitudinal axis of the humerus in a frontal plane. The AHD will be measured using the built-in electronic calliper option by manually locating the superior aspect of the humeral head and the inferior aspect of acromion and then measuring the shortest linear distance between those two landmarks. For each upper limb position, three measurements will be taken (intraclass correlation coefficient (ICC): 0.98; MDC: 0.7 mm).40 Thickness of the SS tendon will be obtained with the medial aspect of the wrist against the ipsilateral anterior superior iliac spine. Measures will be obtained with the transducer perpendicularly, 1 cm behind to the anterolateral aspect of the surface of the acromion. The thickness of the SS tendon borders will be defined inferiorly as the first hyperechoic region above the anechoic articular cartilage of the humeral head, and the hyperechoic superior border of the tendon before the anechoic subdeltoid bursa. IS tendon thickness will be measured at the level of the posterior border of the acromion with the hand placed on the opposite shoulder. The thickness of the IS tendon borders will be defined inferiorly as the first hyperechoic region above the anechoic articular cartilage of the humeral head, and the hyperechoic superior border of the tendon. These US tendon measures have been shown reliable (ICC >0.92).40
Withdrawal of individual participants
All dropouts and their underlying reasons will be reported. Principles underlying ‘intention-to-treat’ analysis will be followed, meaning that every participant will be analysed according to the randomised treatment assignment. Therefore, non-compliance, protocol deviation and withdrawal will all be ignored in the primary analyses. Additionally, ‘per-protocol’ analysis (ie, the analysis will be restricted to participants who adhered to the intervention as stipulated in the protocol) will also be performed. To ensure appropriate insight of mechanisms underlying changes in symptoms and function, only participants who completed evaluation at week 12 will be considered for the US-based outcomes. Any harm or unintended effects during the interventions will be recorded. If a participant presents with an adverse event, the primary investigator will report it to the Ethics Committee.
Data integrity and analysis
All collected data will be accessible only to the research team. All data will be kept for 5 years after the end of the study to ensure the completion of planned publications. After this period, all data will be destroyed. A Data Monitoring Committee is not necessary as this trial is low risk. The research team has opted not to undertake interim analysis.
Statistical analyses
Descriptive statistics will be used for all outcome measures at each measurement time to summarise results. Baseline demographic data will be compared (independent t-tests and χ2 tests) to establish the comparability of groups. All data will be tested to check the distributional assumptions for inferential statistical analyses. If data are normally distributed, a two-way repeated measures analysis of variance (three interventions (control or strengthening or motor control) × 5 times (0, 3, 6, 12 and 24 weeks)) will be used to analyse and compare the effects of the three programmes on primary outcome (QuickDASH) as well as secondary outcomes (three interventions (control or strengthening or motor control)× 2 times (0 and 12 weeks) for the US-based outcomes). Analyses will be made using non-parametric analysis of longitudinal data package (R software) if parametric criteria are not met since it is not possible to assume that the covariance matrix is a compound-symmetry matrix. For the multiple comparisons, Bonferroni post hoc test will be used. Alpha level was set at 0.05.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient-relevant outcomes. Patients will not be invited to contribute to the writing or editing of this document for readability or accuracy.
Discussion
It is essential to develop and identify effective interventions for the management of shoulder pain since it may become chronic and lead to adverse consequences such as decreased participation and quality of life, absenteeism at work, early retirement, multiple medical consultations as well as high associated health costs. As stated earlier, up to 30% of individuals with RCRSP still present pain and disability after rehabilitation interventions such as rehabilitation exercises. A recent study conducted by our research team showed that a rehabilitation programme comprising mainly motor control exercises led to fewer than 15% of individuals showing unsatisfactory results.26 In order to further decrease this percentage, we have attempted to compare different optimized exercise programmes. We have added exercises targeting the whole body, not only the shoulder, to our motor control programme because we believe it is essential to involve the whole body since deficits in trunk or lower limb capacity may overload the upper limb during activities of daily living. On the other hand, multiple studies have shown promising results from strengthening programmes primarily targeting shoulder abductors and external rotators.2 We believe that adding strengthening exercises for other shoulder muscles such as scapular muscles could lead to even better results.
A true control group (wait-and-see approach) will not be included as it would be difficult to maintain a high retention and avoid cointerventions during the mid-term and long-term follow-up. We also chose not to include a placebo group, as it is hard to have a real placebo for this type of study and it is not really ethically fair for the participants given that they will be followed for the 6 months and that the exercises used in the programmes have been shown to be superior to placebo.14
Defining more efficient rehabilitation regimens for common conditions such as RCRSP is important as it may lead to a reduction in associated costs. Therefore, the present study will establish the effectiveness of these two programmes and determine if one is more effective than the other or more effective than education.
Ethics
Ethics approval was obtained from the Sectorial Rehabilitation and Social Integration Research Ethics Committee of the Centre Intégré Universitaire de Santé et de Services Sociaux de la Capitale Nationale (CIUSSS-CN) (No 2019-1762).
Consent
Detailed information about the research and experimental procedures will be provided to all participants before signature of the written informed consent. Participants will be requested to sign a detailed informed consent before starting any experimental procedure (online supplemental file 4).
Supplemental material
Confidentiality
All research team members will respect the data confidentiality of the patients, in agreement with the law. Patients’ names will be coded to keep their identity confidential; however, a list of names and respective codes will be stored in a locked and filing cabinet. All information collected during the study, including test results, will be treated as confidential. The trial data set will be accessible only to the research team and the Ethics Committee of the CIUSSS-CN for the purposes of management or audit of research development. Publications related to these data will respect all principles of confidentiality.
Dissemination
Results of this protocol will be disseminated through international publication in peer-reviewed journals, in addition to international conference presentations. Participants, clinicians and relevant research staff in the field will be informed about the results of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @marco_dube
Contributors MOD contributed to conception, design and preparation of the procedures, and data collection, and will conduct the recruitment, interventions, interpretation, data analyses and writing. FD and JSR contributed to study design, statistical analysis and interpretation of the data. JL contributed to conception, design and preparation of the procedures. All authors commented on the study protocol and approved its final version.
Funding This work was supported by the Quebec Rehabilitation Research Network (REPAR). MOD received a Master’s Training Scholarship from the Fonds de Recherche Québec-Santé (FRQS). JSR and FD are supported by salary awards from the Canadian Institutes of Health Research (CIHR).
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.