Article Text

Abstract
Objective Limited health literacy in patients with type 2 diabetes mellitus (T2DM) led to poorer diabetes knowledge, less medication adherence and increased healthcare cost. The purpose of this paper was to report the prevalence of limited health literacy in patients with T2DM and to identify factors that are associated with it.
Design A cross-sectional study was conducted from January to March 2018; data on patients’ sociodemographic characteristics, diabetes knowledge, perceived social support and health literacy level were collected. Health literacy level was measured using the European Health Literacy Survey Questionnaire (HLS-EU-Q47).
Setting Patients were recruited from four primary care clinics in Perak, Malaysia.
Participants Adult patients diagnosed with T2DM who attended the study clinics during the study period.
Primary outcome variable Patients with HLS-EU-Q47 General Index of ≤33 points were classified as having limited health literacy.
Results The prevalence of limited health literacy was 65.3% (n=279). In bivariate analysis, patients’ ethnicity (p=0.04), highest education level (p<0.001), monthly income (p=0.003), having health insurance (p=0.007), English language fluency (p<0.001), Malay language fluency (p=0.021), attending diabetes education sessions (p<0.001), perceived social support (p<0.001) and diabetes knowledge (p=0.019) were factors associated with limited health literacy. In logistic regression, not being fluent in English was associated with limited health literacy (OR=2.36, 95% CI 1.30 to 4.30) whereas having high perceived social support (OR=0.52, 95% CI 0.40 to 0.69) and having attended diabetes education sessions (OR=0.42, 95% CI 0.27 to 0.68) were associated with adequate health literacy.
Conclusion The prevalence of limited health literacy is high among patients with T2DM in Perak, Malaysia. Strategies to improve health literacy in these patients must consider the influences of English fluency, attendance at diabetes education sessions and social support, and may need to adopt a universal approach to addressing limited health literacy.
- epidemiology
- primary care
- general diabetes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to measure health literacy using the European Health Literacy Survey Questionnaire in patients with type 2 diabetes mellitus in Malaysia.
The study questionnaire was made available in three languages: Bahasa Malaysia, English and Mandarin to ensure inclusion of patients from various ethnicities.
The study was conducted in primary care clinics from urban and rural settings.
This study was conducted in only one state in Malaysia which limits it generalisability.
The cross-sectional design of the study means that we could not determine causality and temporal associations between patients’ health literacy levels and associated factors.
Background
Health literacy is defined as the degree to which individuals can access, understand, appraise and apply health information to make informed health decisions. It is closely related to literacy and entails the individual’s knowledge, motivation and competencies.1 It encompasses the abilities and skills required by patients to deal with the complexity and demands of the health condition or systems where patients are increasingly expected to be partners in care. Recent research showed that health literacy skills are important for patients with type 2 diabetes mellitus (T2DM). When patients are diagnosed with T2DM, they needed to understand new terminologies and learn self-care concepts quickly in order to make healthcare decisions related to treatment and to perform daily self-management activities for optimal diabetes control.2 Studies showed that patients with T2DM and limited health literacy struggled to understand print instructions, health advisories or warnings.3 They have poorer diabetes knowledge,4 5 are less adherent to medication6 and spend more money on their health.7 Furthermore, limited health literacy led to patients having poorer patient–doctor communication and participating less in shared decision-making.8 Studies evaluating health literacy-targeted patient education interventions in patients with T2DM showed improvement of glycaemic control.9 10
Previous studies measured health literacy levels in patients with T2DM and showed the prevalence of limited health literacy to be high; it ranges from 60% to 85%.11 Many of these studies were conducted in high-income countries in North America and Europe. However, nearly 79% of patients with T2DM live in low-income to middle-income countries, like Malaysia.12 Diabetes is a major health problem in Malaysia. In 2015, the prevalence of diabetes in the entire country of Malaysia was 17.5%, which was a 15% increase from the prevalence in 2011.13 The prevalence of diabetes risk factors is also a concern; the prevalence of abdominal obesity ranges from 55.6% to 57.4%14 15 with the prevalence of gestational diabetes reaching 8.66% in 2010.16 High prevalence of these risk factors means that diabetes will continue to be a major health problem in Malaysia for years to come. In order to face this problem, the Ministry of Health, Malaysia, had come up with new policies, strategic plans and clinical practice guidelines (CPGs) on management of patients with T2DM. These guidelines include strategies on screening, prevention and use of new efficacious drugs. Despite this effort, up to 30% of Malaysian patients with T2DM did not achieve the target glycaemic control of haemoglobin A1c (HbA1c) >6.5% as defined by the Malaysian CPG on management of T2DM;17 this led to a high proportion of patients having microvascular (75%) and macrovascular (29%) diabetes complications.18 19
Based on previous studies on health literacy and T2DM, health literacy may be a new target for intervention for patients with T2DM in Malaysia.20–22 Therefore, this study aimed to measure the prevalence of limited health literacy in patients with T2DM and to identify factors that are associated with limited health literacy. Findings in this study could help to identify new targets for interventions in order to improve management of patients with T2DM in Malaysia.
Methods
Study design and settings
This cross-sectional study was conducted at four primary care clinics in Perak, Malaysia. Perak is the second largest state in Peninsular Malaysia. The state of Perak was chosen because it has a diabetes prevalence similar to Malaysia’s prevalence (11.9%, 95% CI 9.9% to 14.3%) and a population with the highest prevalence of adequate health literacy in Malaysia (19.5%, 95% CI 13.2% to 27.9%).13 The latter is important to ensure the sample is from a population with a range of health literacy levels. Four primary care clinics were purposively identified from 17 clinics in Kinta District: Klinik Kesihatan Jelapang, Klinik Kesihatan Buntong, Klinik Kesihatan Manjoi and Klinik Kesihatan Menglembu. These clinics were selected to ensure ethnicity and socioeconomic representations.
Participant selection
Eligible participants were adult men or women with a known diagnosis of T2DM. The diagnosis was confirmed by participants’ medical records. The exclusion criteria were those who were unable to communicate in English, Bahasa Malaysia or Mandarin; had dementia as determined by an Elderly Cognitive Assessment Questionnaire Score of 5 points or less; and who were determined to be too ill based on vital sign assessments or interactions with the research assistants administering the questionnaire.
Data collection
All participants who fulfilled the inclusion and exclusion criteria and attended the study clinics for diabetes follow-up from January to March 2018 were recruited. This study used a self-designed questionnaire to capture participants’ sociodemographic data: age, gender, ethnicity, marital status, highest educational attainment, language fluency, employment status, monthly income and health insurance coverage. Language fluency in both English and Malaysian national language, Bahasa Malaysia, was assessed using a 4-point Likert Scale. Participants self-reported their ability to speak, read and write in the said language. Higher scores on the scale indicate better language fluency. In addition, health literacy level, diabetes knowledge and perceived social support were measured using validated tools. Data on disease outcomes (diabetes control and blood pressure control) were gathered from participants’ medical records. This questionnaire was made available in three languages: English, Bahasa Malaysia and Mandarin and participants chose the language they were most familiar with. The questionnaire was administered with the help of trained research assistants and supervised by the principal investigator.
A pretest of the questionnaire was conducted. Nine face-to-face interviews were conducted with five Malay, two Chinese and two Indian participants. During this process, the participants and the researcher answered the questionnaire together. The participants were asked to voice their thoughts on the questionnaire, particularly with regards to the clarity of the questions and the ease of answering them. The comments from these participants were used to improve the readability and clarity of the questionnaire. Minimal changes were made to the questions included in the questionnaire, including the removal of a question regarding self-rated health status, which the pretest participants had difficulty understanding. In the actual study only one1 participant did not complete all the measurements for the European Health Literacy Survey Questionnaire (HLS-EU-Q47). The participants took on average 15 mins to complete the questionnaire with assistance from the trained research assistants.
Sample size calculation
The sample size was calculated based on the formula by Peduzzi et al.23 Therefore, the required minimal sample size for logistic regression was 331. This number was inflated 20% to account for the non-responder rate giving a final sample size of 397.24
Conceptual model of the study
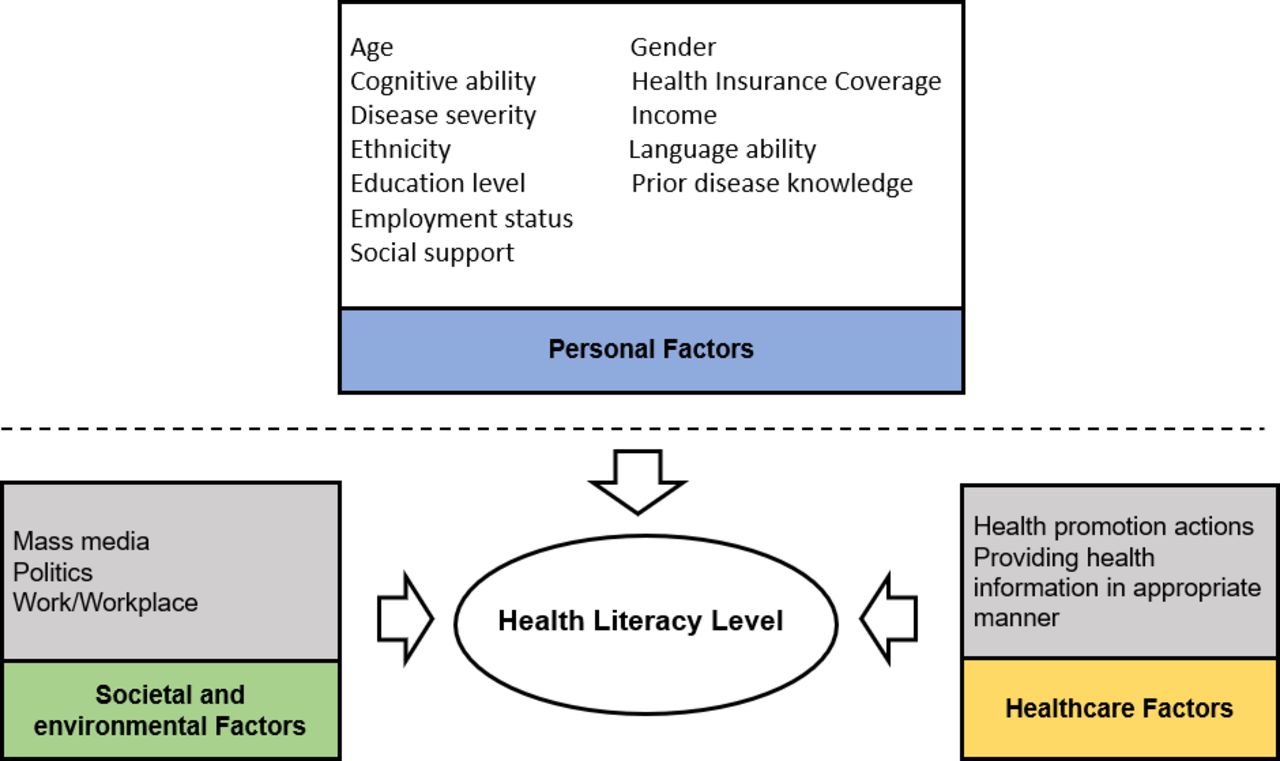
In order to identify possible associated factors of health literacy, we reviewed previous literature and conducted an expert review. A conceptual model of factors that had been found to be associated with health literacy level is presented in figure 1. This study focused on measuring the personal factors that may be associated with limited health literacy in patients with T2DM.
{kind=link}
The conceptual framework for the study measuring factors associated with limited health literacy.
Measures
Health literacy level
Health literacy level was determined using the General Health Literacy Index of HLS-EU-Q47. It contains 47 items that are phrased as direct questions, and the participants have to indicate on a 4-point Likert Scale how easy it is to find, understand, judge and apply health information. The original English questionnaire was validated in English with a good internal consistency of 0.97.25 The Malay and Mandarin translations were validated in a five Asian country survey with both having a Cronbach’s α of 0.96.26 The General Health Literacy Index was calculated using the formula:  . The General Health Literacy Index has a minimum score of 0 and a maximum of 50. Participants were classified as having limited health literacy if their General Health Literacy Index was ≤33 points.27
. The General Health Literacy Index has a minimum score of 0 and a maximum of 50. Participants were classified as having limited health literacy if their General Health Literacy Index was ≤33 points.27
Diabetes knowledge
The participants’ diabetes knowledge was measured using the Michigan Diabetes Knowledge Test (MDKT).28 The MDKT consists of 14 multiple-choice questions, each with one correct answer. The knowledge score is determined by giving 1 point for each correct answer and 0 for a wrong answer or no response. The total knowledge scores range from 0 to 14 with higher scores indicating higher levels of diabetes knowledge. The original version was in English (Cronbach’s α=0.70); the Bahasa Malaysian translation was also found to be valid and reliable (Cronbach’s α=0.702).29
Perceived social support
Perceived social support was measured using the Multidimensional Scale of Perceived Social Support (MSPSS), which measured perceptions of support from three sources: family, friends and significant others.30 The MSPSS is self-administered and contains 12 items, with 4 items for each subscale. Higher scores reflect higher perceived support. The original English MSPSS has excellent internal consistency, with a Cronbach’s α of 0.91 for the total scale. Cronbach’s α for the translated Malay and validated versions was 0.89.31
Disease outcomes
Diabetes-related measurements included the duration of diabetes diagnosis, attendance at diabetes education sessions as well as glycaemic and blood pressure controls. Glycaemic control was assessed using the mean of the three most recent HbA1c values over the last 1 year taken from the patients’ medical records. The blood pressure reading used to determine blood pressure control was also the mean of the three most recent blood pressure readings in the patients’ medical records over the last 1 year.
Data analysis
All statistical analyses were conducted using SPSS V.21.0 (IBM SPSS Statistics for Windows, Armonk, New York, USA). First, we reported the prevalence of limited health literacy and the descriptive statistics analysis of the sample and measured variables. Then we computed the bivariate relationships between measured variables and health literacy groups (limited or adequate health literacy) using the χ2 test for categorical data and the independent t-test or one-way analyses of variance for continuous parametrical data. Then, a binary logistic regression was performed to identify the factors associated with limited health literacy. Variables that had a p value <0.25 in the univariate analysis were included in the logistic regression. The resulting ORs were reported with 95% CIs and the p values. The results were checked for influential cases and multicollinearity. Regression diagnostics showed no influential cases. Furthermore, there was no multicollinearity among the variables. The statistical significance level for the variables inputted in the final model was set at p<0.05.
Patient and public involvement
There were no funds or time allocated for patient and public involvement so we were unable to involve patients. We have invited patients to help us develop our dissemination strategy.
Results
A total of 428 from 450 patients with T2DM approached, agreed to be involved in the study (response rate=95.1%). The mean General Health Literacy Index Score was 31.86 out of 50 (SD=7.04). The prevalence of limited health literacy in patients with T2DM was 65.3% (n=279). The majority of participants answered the questionnaire in Bahasa Malaysia (n=282, 65.8%) followed by Mandarin (n=82, 19.2%) and English (n=64, 15.5%). One patient has more than 30% of data missing, thus was not analysed. Final number of patients included in the analysis was 427. The mean age of the study population was 58.1 years (SD=10.6), and 60.3% (n=258) were female, 43.8% were Malay, 33.4% were Indian and 22.7% were Chinese. The mean duration of diabetes was 5.7 years (SD=3.48), 46.5% (n=199) had attended the diabetes education sessions, 68.9% (n=295) had not achieved target glucose control, conversely 30.4% (n=130) had not achieved target blood pressure control. The mean score for perceived social support was 5.23 (SD=0.92) and the mean diabetes knowledge was 7.70 (SD=2.31) (table 1).
Participants’ characteristics
All variables with a value of p<0.25 in the univariate analysis were included in the multivariate analysis. This analysis was performed using a binary logistic regression (table 2). The results of the likelihood ratio test indicated that perceived social support, attendance at diabetes education sessions in the clinic and English fluency were statistically significant factors associated with limited health literacy (χ2(15)=89.06, p<0.001). Those who were not fluent in English (OR=2.36, 95% CI 1.30 to 4.30) were twice as likely to present with limited health literacy. Patients with better perceived social support (OR=0.52, 95% CI 0.40 to 0.69) and those who attended diabetes education sessions at the clinic (OR=0.42, 95% CI 0.27 to 0.68) were more likely to have adequate health literacy than those who did not.
Factors associated with limited health literacy (n=427)
Consent to participate
All participants provided written informed consent prior to participating in the study.
Discussion
In this study, we found that more than two-thirds of the patients with T2DM attending primary care clinics in Perak, Malaysia have limited health literacy. Malaysia seems to be facing the same challenges as other countries with regards to limited health literacy in patients with T2DM. However, the prevalence in Malaysia is much higher than in several high-income countries such as the USA (30%), Canada (15.6%)32 and countries in Europe, such as Switzerland (8.7%)33 and the Netherlands (9.7%).34 There had not been a comprehensive study to explain the reason for these discrepancies. However, use of different health literacy measurement tools may have contributed to the differences in prevalence.11 Findings from our study suggested that sociodemographic characteristics and healthcare support may also play an important role in determining the prevalence level.
Patients with less perceived social support, not fluent in English and, those who did not attend diabetes education sessions were more likely to have limited health literacy. Patients with better perceived social support from friends, family and significant others were more likely to have adequate health literacy. Studies have shown that people with a larger social network are more likely to use interpersonal communication to seek health information than are people with a smaller social network.35 Qualitative studies suggest that people with a long-term health condition often draw on the health literacy skills of others in their social network36 and that people with high health literacy tend to pass on health information to others.37 This finding highlights the importance of social support in the management of patients with T2DM. Family members and significant others should play a more central role in empowering patients with T2DM.
Limited health literacy is also associated with not attending diabetes self-management education (DSME) sessions delivered at the clinics. DSME is an integral part of diabetes management, and many guidelines recommend that all patients with T2DM receive DSME at diagnosis and as needed thereafter.38 Diabetes education sessions that tailor education to patients with low health literacy levels have been shown to improve patient knowledge, activation, self-efficacy, diabetes distress and self-care behaviours.39 Currently, DSME is delivered by trained diabetes nurse educators. However, there is a significant lack of diabetes educators in Malaysia’s healthcare system. Since 2004, the training courses for diabetes nurse educators by the Ministry of Health have produced approximately 900 trained diabetes nurse educators to practise in a total of 1195 public hospitals and primary care clinics. Although DSME is expected as part of the standard care for all patients with T2DM, in reality, only approximately 4%–7% of patients have received it.40 41 In our study, only 50% of patients surveyed attended DSME sessions at their clinics. Interventions are needed to increase patients’ participation in DSME, and a review of the DSME programme to include training for health literacy may be a game changer in diabetes management.
This study identified three factors associated with limited health literacy that need to be considered when planning for interventions. In contrast to other studies, this study found the association between health literacy level and education level only at the univariate analysis level. In the final regression model, education level was not significantly associated with health literacy; instead, patients’ fluency in English displayed a significant association. Since the multicollinearity analysis was not significant, there were no confounders for this relationship. Limited health literacy is less likely in patients who are fluent in English. A previous study showed that patients who could understand health information better were more likely to have higher health literacy levels.3 It is thought that language influences the amount of information available to patients especially online. Also, in Malaysia, health information and patients’ interactions with healthcare providers are delivered mostly in English. Since most patients received their information from their healthcare providers, limitations in the English language may limit their understanding and appraisal. There may also be other explanations for this observation. Therefore, we plan to embark on a qualitative study to further explore the reasons for this observation.
The strengths of our study is that it had expanded the understanding of health literacy levels in patients with T2DM. Previously, we conducted a systematic review and meta-analysis of prevalence of limited health literacy in the same population of patients and found a lack of data from low-income to middle-income countries. Most prevalence data came from studies conducted in the USA and Europe.42 This study is only the second study done in Malaysia and the first to measure multidimensional aspects of health literacy. The other study showed 85.8% of patients have limited health literacy but used the Newest Vital Signs (NVS) to measure health literacy level.24 The NVS only measures the numeracy component of health literacy36 and has been shown to have administration issues in certain populations in Malaysia.43 In contrast, the HLS-EU-Q47 was well validated in the Malaysian population and was available in three languages commonly used by the multiethnic population of Malaysia.26 The use of HLS-EU-Q47 to measure HL in patients with T2DM is limited. So far only one other study in Spain had used this tool and reported 81.5% of patients with T2DM had limited health literacy.44 This study also added to the data on health literacy in Malaysia. Health literacy is a new research topic in Malaysia that is gaining importance. The health literacy levels of the adult population in Malaysia was first measured in 2015 and the survey found only 6.6% of Malaysian adults had adequate health literacy.13 Our study highlighted the need for further studies on limited health literacy as the problem is also found in patient populations and not just in the general population.
However, this study is not without limitations. Data for this study were collected only in Perak, which may not be representative of all states in Malaysia. Nevertheless, it was not our aim to generalise the findings to the entire country; rather, this study will form a basis to call for a countrywide measure of the health literacy level in patients with T2DM. Since the health literacy level and the associated factors were measured cross-sectionally, causal relationships could not be determined. Patients with type 2 DM who attended DSME or who have better social support may already have adequate health literacy level despite these factors rather than as a result of these factors. A qualitative study is planned to follow-up on these findings to fully understand the influence and impact of these factors on patients’ health literacy level.
Conclusions
In summary, this study found limited health literacy to be prevalent in patients with T2DM. This means that most patients with T2DM attending primary care clinics are unable to fully use their abilities to find, understand, appraise and apply information to optimally manage their disease. Strategies to improve health literacy are required, and must consider issues related to limited English fluency, attendance to diabetes education sessions and social support.
Acknowledgments
The authors thank the study subjects for participating in this study. The authors also thank Dr James Gnanasigamani, Dr Azlin Yusma bt Md Yusup, Dr S Shailaja Siva Sankaran, Mastura bt Awang, Uma A/P Muthu, Sattieswary A/P Govindasamy and Massarah Kee bt Shaharuddin Kee for their support in data collection and participant recruitment. The authors specially thank Dr Alison A. Jackson for proofreading the manuscript.
References
Footnotes
Contributors CJN and SML contributed to the conceptualisation of the study, study design and the writing of the manuscript. SA and PV contributed to the data collection and data analysis. KC contributed to the study design and data analysis. AA contributed to the conceptualisation of the study, study design, data collection, data analysis and the writing of the manuscript. All authors read and approved the final version of the manuscript.
Funding This work was supported by the University Malaya Research Grant, Special Grant, grant no. BKS047-2017.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The deidentified participant data are available upon reasonable request to the corresponding author. She could be contacted at adina@ummc.edu.my.