Article Text

Abstract
Objectives We hypothesised that patients having experienced one coronary event in their life were susceptible to present differences in their pathways of care and within 1 year of their life courses. We aimed to compare pathways between first-time ST-elevation myocardial infarction (STEMI) and STEMI with prior myocardial infarction (MI).
Design A retrospective observational study based on the Observatoire des Syndromes Coronariens Aigus du réseau RESCUe (OSCAR) registry collecting all suspected STEMI from 10 percutaneous coronary intervention centres in France.
Setting All patients with STEMI from 2013 to 2017 were included (N=6306 with 5423 first-time STEMI and 883 STEMI with prior MI). We provided a matching analysis by propensity score based on cardiovascular risk factors.
Participants We defined first-time STEMI as STEMI occurring at the inclusion date, and STEMI with prior MI as STEMI with a history of MI prior to the inclusion date.
Results Patients with first-time STEMI and patients with STEMI with prior MI were equally treated during hospitalisation and at discharge. At 12 months, patients with first-time STEMI had a lower adherence to BASIC treatment (ie, beta-blocker, antiplatelet therapy, statin and converting enzyme inhibitor) (48.11% vs 58.58%, p=0.0167), more frequently completed the cardiac rehabilitation programme (44.33% vs 31.72%, p=0.0029), more frequently changed their lifestyle behaviours; more frequently practiced daily physical activity (48.11% vs 35.82%, p=0.0043) and more frequently stopped smoking at admission (69.39% vs 55.00%, p=0.0524). The estimated mortality was higher for patients with STEMI with prior MI at 1 month (p=0.0100), 6 months (p=0.0500) and 1 year (p=0.0600).
Conclusions We provided an exhaustive overview of the real-life clinical practice conditions of STEMI management. The patients with STEMI with prior MI presented an optimised use of prehospital resources, which was probably due to their previous experience, and showed a better adherence to drug therapy compared with patients with first-time STEMI.
Trial registration number Commission Nationale de l’Informatique et des Libertés (number 2 013 090 v0).
- secondary prevention
- ST-elevation myocardial infarction
- recurrence
- risk reduction behavior
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Observatoire des Syndromes Coronariens Aigus du réseau RESCUe (OSCAR) registry provided an exhaustive overview of real-life clinical practices conditions.
We enrolled 5423 first-time ST-elevation myocardial infarction (STEMI) and 883 STEMI with prior MI.
We provided a matching analysis by fitting a propensity score on cardiovascular risk factors.
A strength of this study was that 88.52% of vital status was known at 1 year post-discharge.
A limitation of this study was that the key lifestyle interventions at 1 year were collected by the general practitioner for only 33.54% of enrolled patients.
Background
The recently declining mortality of patients with myocardial infarction (MI) is attributable to the wide diffusion of early reperfusion techniques,1 modern antithrombotic therapies and secondary prevention.2 Despite these major advances, mortality remains substantial with approximately 10% of mortality rate at 12 months in angiography registries3 4, and in-hospital mortality rates at 4%–12% observed in the national registries of the European Society of Cardiology (ESC) countries.5 Additionally, reinfarction carried a strong, significant and independent risk of subsequent cardiac death.6 Regardless of the curative and preventive treatments, the literature has identified individual predictors of reinfarction, such as advanced age, arterial hypertension, hyperglycaemic, dyslipidaemia, renal failure, alteration of left ventricular ejection fraction (LVEF), history of ischaemic stroke,7 8 active smoking and certain genotypes.9 Whereas the management of the acute phase is essential in short-term outcomes,10 the key lifestyle interventions following MI, as depicted by the European guidelines,11 give the patient a central role in their own management. The literature has shown that a low adherence to drug therapy and behavioural interventions were associated with worse outcomes.12 It is estimated that only 14%–35% of heart attack survivors participate in secondary prevention programmes, and 70% of suitable patients did not receive dedicated interventions for risk factor reduction.13 We hypothesised that despite the absence of differences in management in the acute phase between the first-time ST-elevation MI (STEMI) and STEMI with prior MI, the life courses within 12 months post-STEMI may differ. This study aimed to compare the pathways of care in the acute phase and the life courses within 12 months between first-time STEMI and STEMI with prior MI.
Methods
Data source
Since 2010, the Réseau Cardiologie Urgences (RESCUe) network has gathered emergency physicians and cardiologists from 10 percutaneous coronary intervention (PCI) centres around common guidelines. Covering a population of 3 million inhabitants in the Rhône-Alpes region of France, the prospective observational Observatoire des Syndromes Coronaires Aigus du réseau RESCUe (OSCAR) registry reports all patients with persistent chest pain and ST-segment elevation ≥2 mm in two contiguous leads, with no limitations with respect to age or delay in treatment. The monitoring of clinical research technicians guaranteed the quality and completeness of data, which is regularly tested by cross-checking the regional medico-administrative data. Since 2009, data have been at least 85% complete.14 All the participants gave oral informed consent. We used the Strengthening the Reporting of Observational Studies in Epidemiology cohort reporting guidelines.15
Patient and Public Involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of the research.
Collected data
Patients were enrolled by prehospital emergency medical services (EMS) or the emergency department (ED). They received an individual information notice in accordance with the French legislation and gave their oral consent to participate in the data collection. At 12 months after discharge, the patient or his relatives were contacted by phone to collect possible new cardiac events, their vital status and adherence to the BASIC treatment (ie, beta-blocker, antiplatelet therapy, statin and converting enzyme inhibitor). For this study, the patients have not been re-contacted; all the information used in this study was derived from data collection in the observational register.
Collected data comprised cardiovascular history at admission, regular medications, prehospital delays and hospital management. We referred to BASIC treatment as the optimal drug therapy recommended by the ESC 2017 guidelines,11 which is a combination of a beta-blocker, antiplatelet therapy, statin and converting enzyme inhibitor. After hospital discharge, a phone operator contacted patients or their relatives at 12 months to collect adherence to BASIC treatment. At 12 months, a survey was sent by mail to general practitioners (GPs) to collect additional information about healthy lifestyle behaviours (including cessation of smoking, advice about diet and weight control, encouraged physical activity at least 30 min/day, participation in a cardiac rehabilitation programme and monitoring of lipid and glucose at 3 months and/or 6 months) and vital status (cause and date of death). The data from the GPs were retained if any discrepancies were reported between the follow-up by phone and the survey.
Population selection
All patients with STEMI as a final diagnosis were included. We restricted the study period from 1 January 2013 to 31 December 2017, considering a delay of 2 years after the French marketing authorisation for ticagrelor and 1 year after European recommendations favouring P2Y12 inhibitors at discharge, such as clopidogrel.16 17 A first-time STEMI was defined as a STEMI occurring at the inclusion date, without history of coronaropathy disease in the past, and STEMI with prior MI was defined as a STEMI with a history of MI up to 1 year before the inclusion date (figure 1).
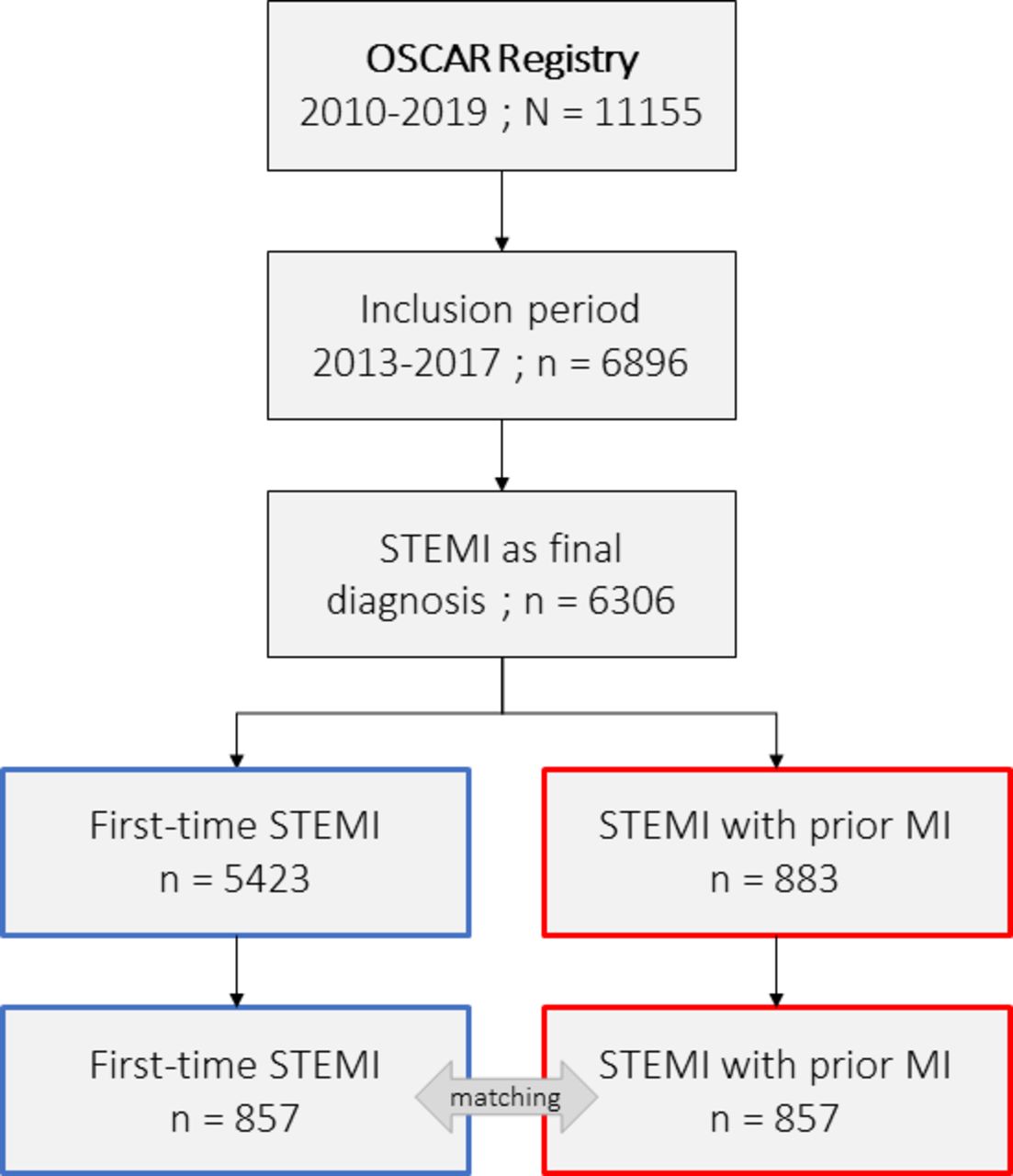
Flowchart of the study population from the OSCAR, registry of acute coronary syndromes. MI, myocardial infarction; OSCAR, Observatoire des Syndromes Coronariens Aigus du réseau RESCUe; STEMI, ST-elevation myocardial infarction.
Outcomes: measured indicators
The comparison of the pathways of care between first-time STEMI and STEMI with prior MI was based on recommended quality indicators18 as follows: (1) proportion of patients reperfused within 12 hours from the onset of symptoms to diagnosis, (2) proportion of patients with timely reperfusion, (3) proportion of patients with adequate P2Y12 inhibition at discharge and/or with dual antiplatelet therapy, (4) proportion of patients discharged on statins, (5) proportion of patients with heart failure discharged on an Angiotensin Converting Enzyme Inhibitor (ACEI) or Angiotensin Receptor Blocker (ARB) if intolerant of an ACEI and (6) proportion of patients with heart failure discharged on beta-blockers. The comparison of life courses between first-time STEMI and STEMI with prior MI was based on the key lifestyle interventions mentioned in the 2017 ESC guidelines, including: (1) the 12-month adherence to BASIC treatment, (2) the follow-up of the cardiac rehabilitation programme, (3) daily physical activity, (4) smoking cessation for active smokers, (5) balanced diet for overweight, diabetes and dyslipidaemic patients and (6) lipid and glucose monitoring at 3 months and/or 6 months.
Statistical analysis
Categorical data are presented as frequencies and percentages, and continuous data are presented as medians and IQRs (first and third quartiles). The Results section mentions in brackets the observed data for first-time STEMI and then for STEMI with prior MI. Bivariate statistical comparisons were performed with Pearson’s χ2 test for categorical data and the non-parametric Wilcoxon rank test for continuous data, which is labelled as ‘unadjusted p value’. A probability value, p, of less than 0.05 was considered significant. We also provided a matching analysis by fitting a propensity score. The propensity score was computed by logistic regression using 6306 patients (0: first-time STEMI vs 1: STEMI with prior MI, as response variables). The explanatory variables were age, sex, active smoking, hypertension, diabetes, dyslipidaemia, renal failure and being overweight. The matching was achieved using the nearest neighbour method with a specified calliper distance of 10% of the propensity score’s SD. We excluded 223 (3.54%) patients, with 197 (3.63%) first-time STEMI and 26 (2.94%) STEMI with prior MI, because of missing values. The final matched population comprised 1714 patients (857 first-time STEMI vs 857 STEMI with prior MI). The balance between matched samples was assessed using standardised mean differences before and after matching (figure 2). We performed the McNemar’s Khi² test for categorical variables and the non-parametric Wilcoxon sign test for continuous variables to compare adjusted pairs, which was labelled as ‘adjusted p value’. We provided a Kaplan-Meier survival curve for comparison of mortality rates at 1 month, 6 months and 1 year post-qualifying ECG. For testing the equality of survival curves in propensity score matched samples, we performed stratified log-rank tests.19 We mentioned the adjusted results alongside the results section, except for the section’s baseline characteristics.

Standardised mean differences before and after propensity score matching. MI, myocardial infarction; STEMI, ST-elevation myocardial infarction.
Results
Baseline characteristics
We enrolled 6306 patients with 5423 first-time STEMI and 883 STEMI with prior MI. Patients with first-time STEMI were younger than patients with STEMI with prior MI (62 years old (53-74) vs 67 years old (56-78), p<0.0001) and presented fewer cardiovascular risk factors at admission, including hypertension (40.90% vs 54.81%, p<0.0001), diabetes (15.80% vs 28.88%, p<0.0001), dyslipidaemia (27.84% vs 46.77%, p<0.0001) and renal failure (20.47% vs 28.99%, p<0.0001) (table 1). Overweight patients were represented equally in both groups (38.80% vs 40.77%, p=0.2817). Women were older than men (72 years old (59-82) vs 60 years old (51-70), p<0.0001) in the first-time STEMI group. Reinfarction occurred later in life for women compared with men (78 years old (64.5-87) vs 65 years old (55-76), p<0.0001). There was also no difference regarding heart failure (Killip score≥2) (9.98% vs 15.29%, p<0.0001), cardiogenic shock at admission (Killip score=4) (1.07% vs 1.25%, p=0.7700) and cardiac arrest (6.88% vs 5.89%, p=0.3102).
Baseline characteristics at admission of first-time STEMI and STEMI with prior MI
Delays and reperfusion strategy
The following results were presented after matching analysis. Patients with STEMI with prior MI more frequently called the medical dispatch centre (p<0.0001) and were more frequently managed by EMS (p<0.0001) compared with patients with first-time STEMI (table 2). Once in the pathways of care, the delays from symptom to ECG were comparable whether patients were managed by EMS (p=0.2420) or arrived directly to the ED (p=0.0609). When patients arrived directly to the ED, the delay from symptom to admission was longer for patients with first-time STEMI (p=0.0347). The patients with first-time STEMI received more PCI (p=0.0049). Among patients with PCI, the delay from ECG to reperfusion was similar between both groups (p=0.7339), as well as the LVEF (p=0.0954).
Management delays of first time STEMI and STEMI with prior MI groups in the acute phase (delays in minutes) and reperfusion strategy
Pathways of care in the acute phase
Even though both groups were equally treated with primary PCI (p=0.2293), we observed a lower proportion of stenting among STEMI with prior MI (p<0.0001). The initial observation of thrombolysis in MI grade flow 0 were similar between the two groups (p=0.9169), with complete reperfusion (p=0.8391). During hospitalisation, patients with first-time STEMI and patients with STEMI with prior MI were equally treated with adequate P2Y12 inhibition (96.74% vs 95.14%, p=0.5322). The prescriptions of P2Y12 inhibitors at discharge were different between the groups for ticagrelor (55.71% vs 43.26%, p<0.0001) and clopidogrel (15.10% vs 23.33%, p<0.0001), but the difference was not significant for prasugrel (12.26% vs 9.06%, p=0.0713).
At discharge, patients were equally treated with statins (95.29% vs 91.88%, p=0.0872), ACEI (92.31% vs 88.46%, p=1) and beta-blockers among patients with heart failure (93.99% vs 92.27%, p=0.4795) and dual antiplatelet therapy (95.99% vs 94.64%, p=0.6583). We observed a higher in-hospital mortality among patients with STEMI with prior MI (p=0.0360).
Life courses within 12 months of follow-up
Concerning the life courses within 1 year after discharge, we observed only 33.54% of follow-up by the GP, with no significant difference in the follow-up proportions between the groups (33.98% vs 30.80%, p=0.0691). At 12 months, the first-time STEMI group presented a lower adherence to BASIC treatment compared with the STEMI with prior MI group (48.11% vs 58.58%, p=0.0167) (figure 3). The first-time STEMI group also more frequently completed the cardiac rehabilitation programme (44.33% vs 31.72%, p=0.0029), presented better adherence to the recommended lifestyle behaviours with the practice of a daily physical activity (48.11% vs 35.82%, p=0.0043) and stopped smoking (for active smokers reported at admission) (69.39% vs 55.00%, p=0.0524) compared with the STEMI with prior MI group. We did not observe differences between first-time STEMI and STEMI with prior MI with regard to a balanced diet for overweight, diabetes and dyslipidaemic patients (72.82% vs 67.55%, p=0.3023) and lipid and glucose monitoring at 3 months and/or 6 months (92.78% vs 88.43%, p=0.1045).

Radar plots for the pathways of care in the acute phase (reperfusion among eligible patients, timely reperfusion among eligible patients, adequate P2Y12 inhibition during hospitalisation, statins at discharge, Angiotensin Converting Enzyme Inhibitors (ACEIs) at discharge among patients with heart failure, beta-blockers at discharge among patients with heart failure and dual antiplatelet therapy) and the life courses within 12 months of follow-up (12-month adherence to BASIC treatment, cardiac rehabilitation programme, daily physical activity, smoking cessation for active smokers, balanced diet for overweight, diabetes and dyslipidaemic patients, and lipid and glucose monitoring at 3 months and/or 6 months) based on matching analysis. BASIC, beta-blocker, anti-platelet therapy, statin and converting enzyme inhibitor; MI, myocardial infarction; STEMI, ST-elevated myocardial infarction.
The vital status at 1 year was known for 88.70% of the first-time STEMI and 87.43% of the STEMI with prior MI (p=0.2991). The mortality estimated by the Kaplan-Meier estimator was higher for patients with STEMI with prior MI compared with patients with first-time STEMI (figure 4) at 1 month (6.7% (5.0%-8.4%) vs 10.3% (8.2%-12.4%), p=0.0100), 6 months (8.3% (6.4%-10.1%) vs 11.4% (9.1%-13.5%), p=0.0500) and 1 year (9.7% (7.6%-11.7%) vs 13.0% (10.6%-15.3%), p=0.0600).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves of mortality at 1 month, 6 months and 1 year post-qualifying ECG. MI, myocardial infarction; STEMI, ST-elevated myocardial infarction.
New cardiac event within 12 months follow-up for the first-time STEMI
Among the first-time STEMI, we observed 3.45% patients with a new cardiac event during the 1-year follow-up (187/5423). We did not observe any differences in the secondary prevention programme between first-time STEMI that experienced a cardiac event during follow-up and those who did not: p=0.1247 for daily physical activity, p=0.2459 for smoking cessation for active smokers reported at admission, p=0.3912 for balanced diet for overweighted, diabetic or dyslipidaemic patients, and p=0.2198 for lipid and glucose monitoring at 3 months and/or 6 months.
Discussion
Concerning the pathways of care in the acute phase, the ESC 2017 guidelines recommended immediate angiography in cases of STEMI with prior MI. In this study, we noticed only 26/5423 patients with first-time STEMI and 4/883 patients with STEMI with prior MI who did not undergo coronarography probably because of their advanced age, comorbidities and risk of major bleeding. Also, we observed a lower PCI rate for the STEMI with prior MI compared with first-time STEMI. This difference may be partly explained by a higher rate of coronary revascularisation surgery (45/315 (14.3%) vs 14/85 (16.5%), p=0.7484) or a higher rate of in-hospital mortality after coronarography (31/315 (9.8%) vs 14/85 (16.5%), p=0.1277) in the STEMI with prior MI group. Based on the recommended quality indicators, we observed a small margin of improvement in the acute phase, except for the timely reperfusion for first-time STEMI and STEMI with prior MI.
Concerning the life courses within 1 year after STEMI, the patients with first time STEMI were less compliant to treatments at 1-year follow-up, but they seem more compliant to lifestyle changes. The literature stated that survivors of STEMI remained at high long-term risk of recurrent ischaemic cardiovascular events20 21 and mortality, and demonstrated the effectiveness of patient education in decreasing the risk with changing the key lifestyle habits in particular smoking cessation22 and control of the high density lipoproteinlevel.21 The literature has also highlighted that secondary prevention strategies after a STEMI episode are still far from being optimal23 and also denoted substantial problem of guidance documents for clinicians.24 These results potentially counterbalance the prognostic benefits of the reperfusion therapy. Literature also suggested the need to integrate post‐discharge health support with cardiac rehabilitation to facilitate recovery after primary PCI,25 with post‐discharge home visits at 4 weeks and at 6 months for instance. In this study, we observed that one-third of patients were discharged home within 48 hours after STEMI, which tends to trivialise the MI and suggests that patients were probably not receptive to the prevention messages. And as mentioned in the literature, the existence of the ‘healthy adherer’12 should also probably be considered.
Further investigations are required to identify the reasons for non-adherence to secondary prevention and to propose appropriate responses to clinicians and patients. Our findings should also make us focus on the possibility to propose post-discharge health support to increase the adherence to key lifestyle interventions, and thus facilitate recovery and reduce reinfarction and mortality. Another investigation field concerns the impact of living in rural and urban geographical area on the recovery.26 The 2019 AHA recommendations concluded that education programmes must consider patients’ health literacy, education levels and motivations to improve their lifestyle habits.27 One of the key goals also included the consideration of the cost and value for enhancing the overall value of the delivery of cardiovascular care.
With 88.52% of patients with STEMI being followed-up at 1 year, we brought a substantial added value with respect to the main challenges in secondary prevention.13 However, several limitations should be mentioned. First, data about clinical history (eg, cancer or chronic obstructive pulmonary disease) and coronary atherosclerotic involvement (eg, left main or multivessel disease, syntax score, chronic total occlusion and incomplete revascularisation) were not collected in the Registry and could have a prognostic value in the 1-year follow-up. Also, we cannot determine the role of secondary prevention in the 1-year mortality or reinfarction rates, because the key lifestyle interventions were collected for patients who were alive at 1 year after PCI discharge. Second, the date of reinfarction was not collected during the 1-year follow-up, preventing a survival analysis and a multivariate analysis to determine the role of secondary prevention in reinfarction and/or mortality.
Conclusion
The OSCAR registry provided an exhaustive overview of real-life clinical practices conditions for the management of STEMI in the acute phase and during the 1-year life courses. There was no significant difference in terms of delays and reperfusion strategies between first-time STEMI and STEMI with prior MI. STEMI with prior MI presented an optimised use of prehospital resources, probably due to their previous experience. But nearly one half of survivors did not observe the secondary prevention programme with low adherence to BASIC treatment and to the recommended lifestyle behaviours.
References
Footnotes
Collaborators On behalf of the RESCUe Research Group: Dr Christophe Robin (Clinique Convert, Bourg en Bresse), Dr Xavier Tchenio (Hôpital Fleyriat, Bourg en Bresse), Dr Pierre Lantelme (Hôpital Nord-ouest site Villefranche), Dr Pierre Lantelme (HCL Groupement Hospitalier Nord, Lyon 4), Pr Eric Bonnefoy-Cudraz (HCL, Groupement Hospitalier Est Hôpital L Pradel-Bron), Dr Jean-Philippe Claudel (Infirmerie Protestante, Caluire-Cuire), Dr Alain Hepp (Clinique la Sauvegarde, Lyon 9), Dr Thibault Perret (Centre Hospitalier Saint Joseph-Saint luc, Lyon 7), Dr Didier Champagnac (Médipôle Privé, Villeurbanne) and Dr Philippe Chapon (Centre Hospitalier de Valence).
Contributors LF drafted the manuscript and develop methodology., OK interpreted the results. CC provided statistical analysis. NE and AP collected the data. KT, EB-C and CD provided critical readings. CEK supervised the work.
Funding The RESCUe Network is funded by the Regional Agency for Health from Auvergne-Rhône-Alpes region (Agence Régionale de Santé Auvergne-Rhône-Alpes). Grant/Award: not applicable.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.