Article Text

Abstract
Introduction Parkinson’s disease (PD) is the second most common neurodegenerative disorder in Brazil. Physical activity is a complementary intervention in managing inherent declines associated with the disease like strength, balance, gait, and functionality and benefit health-related outcomes. Here, we report the PARK-BAND Study protocol, which aims to investigate potential benefits of power training using elastic devices in participants with PD. Our intervention will be provided in patients with PD using elastic devices like elastic bands and tubes. Therefore, we used the term Park from Parkinson’s disease and band from elastic bands.
Methods and analysis This randomised single-blind single-centre two-arm parallel, superiority trial will include 50 participants with PD attending the clinical setting. Those who meet the eligibility criteria and provide consent to participate will be randomised in a 1:1 ratio to either the exercise group, which will receive power training programme or the health education group, which will receive the education programme. Randomisation will be performed by permuted block randomisation with a block size of eight. Both groups will receive a 12-week intervention. The exercise group will have two sessions per week and the health education group will have one session per week. Changes from baseline in bradykinesia, as assessed by the Unified Parkinson's Disease Rating Scale motor examination subscore and physical functional performance, will be the primary outcomes. Secondary outcomes include other neurological, neurophysiological and physical variables, as well as the quality of life, depression, cognition, sleep quality and disturbances, assessed before and after interventions. We hypothesise that the exercise group will have greater improvement in primary and secondary outcomes than the health education group.
Ethics and dissemination The study is approved by the Research Ethics Committee of Hospital Universitário Walter Cantidio and all participants will provide their written informed consent (register number 91075318.1.0000.5045).
Trial results will be disseminated via peer reviewed journal articles and conference presentations, reports for organisations involved with PD and for participants.
Trial registration number Registro Brasileiro de Ensaios Clínicos Registry (RBR-5w2sqt); Pre-results.
- geriatric medicine
- Parkinson's disease
- rehabilitation medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The main characteristic of Parkinson’s disease (PD) is bradykinesia which is one of the main purposes of our intervention.
Power training with elastic devices is a simple, low-cost and easy-to-perform intervention which has potential benefits to participants with PD.
The sample size (50 participants) was calculated to be suitable for the two primary outcomes since the estimated size for bradykinesia was 24 per group and for Short Physical Performance Battery was 12 per group.
Recruiting for the PARK-BAND will be challenging, due to the extensive list of eligibility criteria and the relative fragility of some participants.
Background and rationale
Parkinson’s disease (PD) is the second most common neurodegenerative condition in Brazil, occurring in approximately 1% of individuals older than 65 years.1 Considering the projected increase in PD prevalence,2 interventions to minimise morbidity and improve quality of life are crucial. Currently, there is no proven pharmacological therapy to modify or slow the disease progression. Physical activity is, however, reported to complement pharmacological therapy in managing the inherent declines associated with the disease like strength, balance, gait and functionality.3 Studies indicate that upregulation of neurotrophic factors, including the brain-derived neurotrophic growth factor, is the potential mediator of the benefits associated with physical activity.3 Accumulated evidence suggests that individuals with PD may benefit from physical activity in several ways, from improvements in overall health to reductions in neuromuscular symptoms and other disease-modifying effects.3 However, randomised controlled trials on intervention with physical activity in PD is limited, mainly consisting of resistance training and movement-specific training.4
Muscle power is a more important predictor than strength in the functional performance of gait and in risk for falls in individuals with PD.5 According to the UK’s Parkinson’s Disease Bank Criteria, bradykinesia is required for a diagnosis of PD.6 Indeed, bradykinesia is the main cause for impairment in daily activities.7 Muscle power is the product of force and contraction velocity, factors that lead to a reduction in either of these parameters, or both, will contribute to reduced muscle power output. Power training (PT) is based on high-speed movement with low loads of resistance.8 PT is a specific method of resistance training (RT) that has been emphasised as an effective exercise intervention for improving strength, power and physical performance in different populations.4 9–11 The main characteristic of PD is bradykinesia which is one of the main causes of functional impairment of these individuals. In addition, studies have shown high prevalence of sarcopenia and dynapenia in these subjects compared with subjects without PD.12
In PD, changes in the frequency, variability and intensity of activation of motor units13 14 can contribute to deficits in the recruitment of the larger motor units required in the generation of rapid strength.15 In addition, the existence of a selective loss of type II muscle fibres in these individuals has been suggested.16 Thus, such changes in the neuromuscular system would limit the recruitment of larger high-frequency motor units necessary for the rapid production of torque during ballistic and isometric movements.15 As a consequence, movements are observed with decreased torque production during the acceleration phase and peak torque resulting in different manifestations of bradykinesia and muscle weakness in PD, respectively.15
Besides, neuromuscular changes such as an increase in the rate of strength development (increased firing frequency and/or recruitment of larger motor units) have been observed after resistance training17 18 and are decisive for high levels of muscle strength to be produced in the early stages of muscle contraction, guaranteeing the rapid execution of the movement. An increase in descending stimuli with increased firing frequency and the recruitment of larger motor units has been associated with muscle power training in the elderly.18 According to Aagard et al, the rate of strength development plays an important role in the ability to perform fast and efficient movements in the elderly18 who need to control unexpected disturbances in balance. The mechanism of action proposed above justifies the use of power training to minimise bradykinesia in PD. High-speed strength training has improved functional outcomes in PD in some studies.10 19 However, the literature is scarce about the advantages of PT for PD comparing with other interventions.20 Recent meta-analysis that investigated the efficacy of different exercises on PD included different types of training programmes like yoga, tango, dance, tai chi, RT, multimodal exercise training, aerobic exercise, qi gong, but no PT training.21
Given that PT focuses on rapid movement speed by low-resistance training, it would be beneficial to examine its role on functional outcomes in subjects with PD. Indeed, further studies are needed to support the beneficial effects of different types of RT in subjects with PD and to investigate the superiority of PT in participants with PD comparing with other treatment strategies.
Training with elastic bands represents a simple and affordable form of exercise suitable for the elderly, including those with mobility limitations.22 The ability to perform movements with speed has relevant clinical implications for the functional performance of elderly people with low mobility and risk of falls. Exercises with elastic bands are effective to promote strength increase similar to those of conventional RT, using different exercise regimes.22 Elastic bands and tubing are a simple-to-use tool for multipurpose physical training, highly practical allowing all the major muscle groups to be worked on.23 24
A health education programme can promote better understanding of the disease, drug treatment and non-pharmacological interventions to improve the quality of life of participants with PD. Education can motivate subjects to change their behaviours in improving diet, sleep, physical activity and quality of life. They will also learn strategies to prevent falls, infections and declines in their capacity to perform daily activities.25
This study aims to investigate the potential benefits of PT using elastic devices in participants with PD. PT with elastic devices is a simple form of physical activity that is low cost and easy to perform, requiring minimum space and equipment. Therefore, it can be easily implemented as a PD treatment strategy if proven effective.
Hypothesis
We hypothesise that PT will be more efficient than the health educational programme in promoting improvements in motor and non-motor parkinsonian symptoms, physical functional performance and quality of life of participants with PD.
Specific objectives
Primary objective
To determine if power training is more efficient than a health educational programme in improving bradykinesia and physical functional performance.
Secondary objectives
To ascertain if power training is superior to a health education programme in improving non-motor parkinsonian symptoms and quality of life.
Methods/trial design
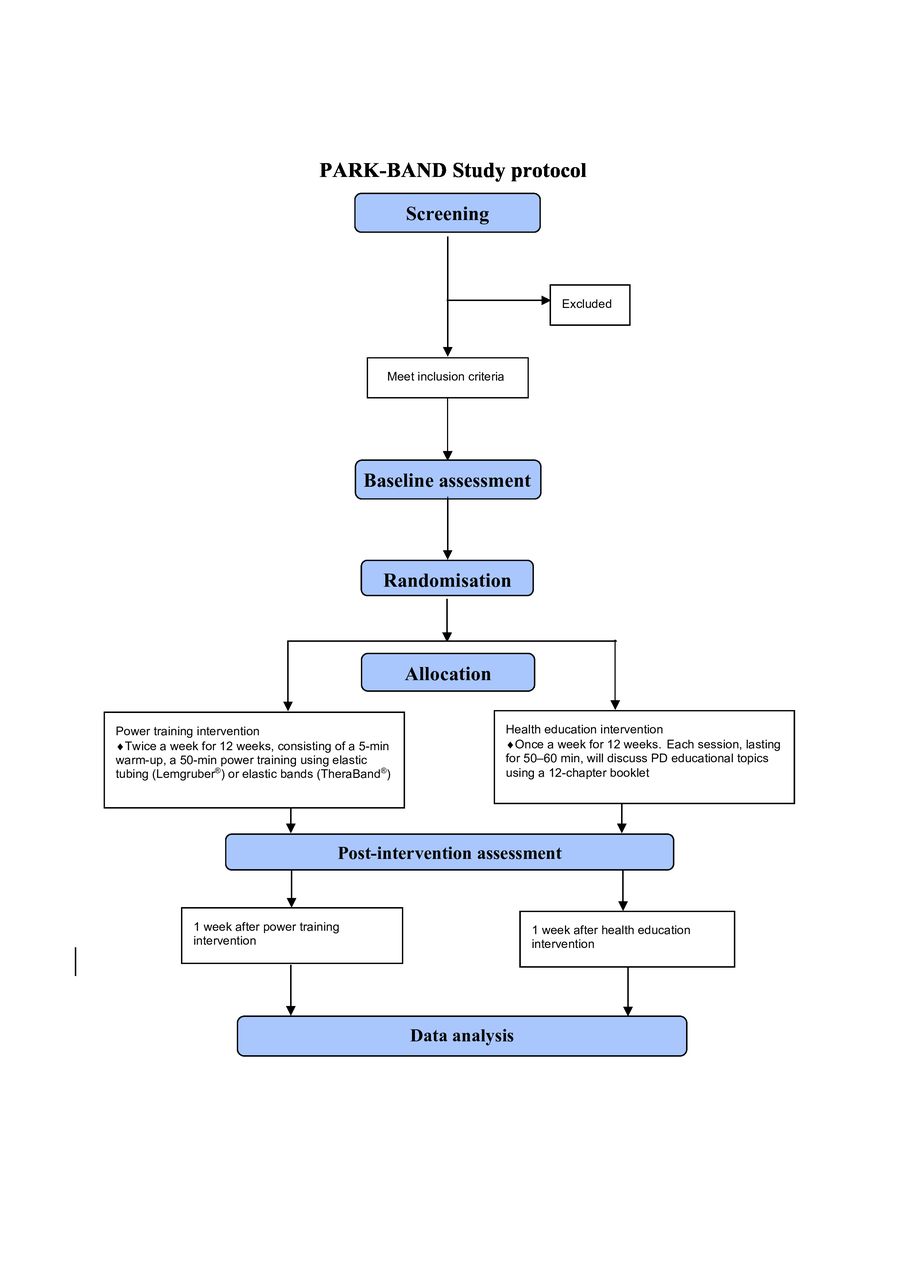
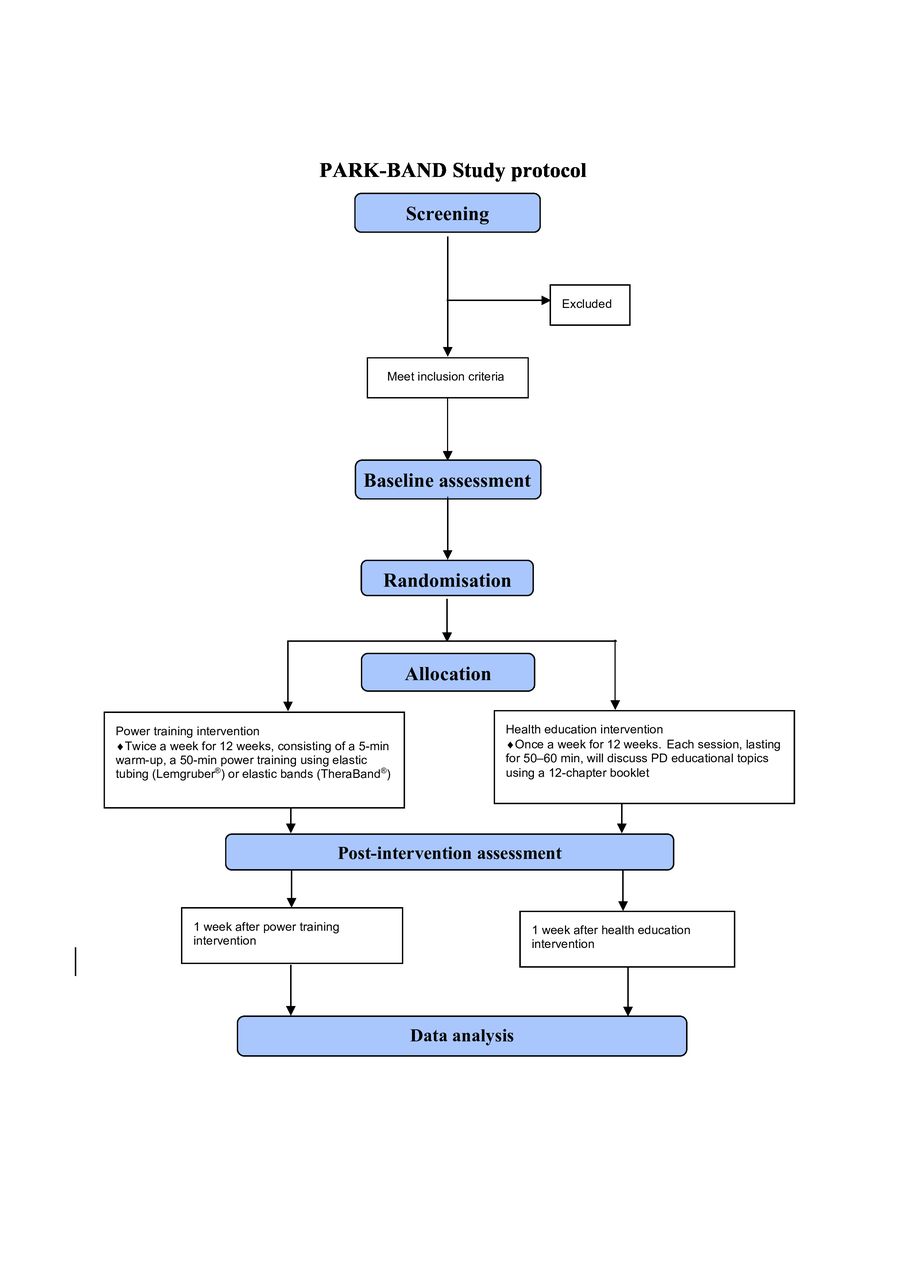
The PARK-BAND programme is a randomised controlled single-blind superiority trial. The primary endpoint of the study is improvement in motor parkinsonian symptoms of bradykinesia, as determined by Movement Disorders Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part III and Short Physical Performance Battery (SPPB). Details about trial information are available in online supplemental file 1. Eligible participants will be allocated in a 1:1 ratio to either the experiment or the control group, through a permuted block randomisation with a block size of eight. The flow diagram of the protocol is detailed in figure 1. All participants of both groups will perform the sessions during ‘on’ phases of medication.
Supplemental material
{kind=link}
Flow diagram of the study according to the Consolidated Standards of Reporting Trials. PD, Parkinson’s disease.
The PARK-BAND intervention protocol was developed in accordance with the Template for Intervention Description and Replication (TIDieR) checklist. An additional file shows this in more detail (see online supplemental file 2).26 The study protocol was described according to the Standard Protocol Items: Recommendations for Interventions Trials statement—item 11.27 The time schedule of the protocol is in online supplemental file 3.
Supplemental material
Supplemental material
Composition and roles of committees for the PARK-BAND protocol are detailed in online supplemental file 4.
Supplemental material
Study setting
The Hospital Universitário Walter Cantídio (HUWC) of Universidade Federal do Ceará (UFC) is a reference centre for training human resources and developing health research. Being integrated with the Public Health System, it also acts as an important centre for healthcare in Ceará. As a reference centre for teaching, it serves as an internship field for undergraduate and graduate students of UFC’s Medicine, Nursing, Physiotherapy and Pharmacology courses.
The Movement Disorders Outpatient Clinic of the HUWC manages approximately 350 subjects with PD. The neurologists and geriatricians work together once a week to assist them. Participants for this clinical trial will be recruited from this clinical setting.
The research project was submitted to the Research Ethical Review Board of the Clinical Research Unit of HUWC, Fortaleza, Ceará, Brazil, according to the terms of Resolution 466/2012, and was approved under report #91075318.1.0000.5045.
The description of the research team of our single centre and the contribution of each researcher are available in the online supplemental file 5.
Supplemental material
Eligibility criteria
Participants meeting the inclusion criteria and willing to provide written informed consent before trial initiation will be eligible. Participants will be informed that they can withdraw from the study at any time and that their withdrawal will not impact their care or inclusion in future studies.
Inclusion criteria
Eligible subjects meeting all of the following criteria at the time of randomisation will be included in the study:
Diagnosis of PD according to the United Kingdom Parkinson’s Disease Society Brain Bank criteria.
PD stages of I–III according to the modified Hoehn and Yahr Scale.
Stable medication regimen for at least 4 weeks before the trial.
Literate.
Perform basic daily living activities independently with a Schwab and England score of ≥80%.
Age, ≥40 years.
Exclusion criteria
Exclusion criteria were unstable cardiovascular disease or other uncontrolled chronic conditions that would affect their safety, testing or interpretation of results.
Participants meeting any of the following criteria will be excluded:
Body mass index >40 and <20 kg/m2.
Diagnosis of Crohn disease or ulcerative colitis.
Diagnosis of multiple sclerosis, acute disseminated encephalomyelitis, parkinsonism plus, cerebrovascular disease with motor sequelae or Guillain-Barre syndrome.
Dementia syndrome of any aetiology according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Schizophrenia with hospitalisation or a psychotic episode or suicidal ideation in the past 6 months.
Bipolar affective disorder with hospitalisation or an episode of mania, hypomania or depression in the past 6 months.
Depression with hospitalisation or suicidal ideation or a psychotic episode in the past 6 months.
Myocardial infarction with or without ST elevation in the past 12 months.
Myocardial revascularisation surgery or percutaneous angioplasty in the past 12 months.
Uncontrolled arrhythmia.
Severe or oxygen-dependent chronic obstructive pulmonary disease.
Cardiac insufficiency with reduced functional class III or IV symptoms.
Resting blood pressure of ≥160×100 mm Hg.
Implantable cardioversion defibrillator.
Severe chronic kidney disease (creatinine clearance of <30 mg/dL).
Proliferative retinopathy (type 2 diabetes mellitus).
Peripheral neuropathy with motor impairment.
Moderate-to-severe hearing impairment: inability to maintain a dialogue or need for lip reading.
Moderate-to-severe visual impairment: minimum visual acuity 20/70 on the Snellen Scale.
Active cancer or receiving treatment for cancer.
History of conventional surgery or deep brain stimulation for PD.
Alcohol consumption >14 drinks per week.
Living with individuals participating in the same study.
Thromboembolism without anticoagulation regimen.
Significant weight loss (10% of usual weight) in the past 6 months.
Lack of family support to participate in the study.
Bariatric surgery.
Exercise at moderate or high intensity for at least three times a week.
Glycated haemoglobin (HbA1c) level of ≥12.
Interventions for each group
Control group: health education
The Health Educational Intervention Committee (HEIC) elaborated the 12 sessions very carefully. The health education group will have four participants which will receive sessions to discuss PD educational topics once a week for 12 weeks, each session lasting for 50–60 min. This group will receive a 12-chapter booklet that will tell the story of a patient who received the diagnosis of PD and learnt about its clinical features, treatment and complications. Each chapter will teach the reader the strategies for living well with the disease.
It was planned each session with group dynamics and tutorial questions for group discussion. The sessions will be supervised by a psychologist and they will be performed by the HEIC. The educational booklet was written in accordance with the recommendations of A Guide to Creating and Evaluating Participant Materials which explains about design and effectiveness of educational materials.28 We have had active participation in its elaboration from health professionals of nursery, physicians, physiotherapists, nutritionists, psychologists, professionals of physical education and pharmaceutics. We agreed by common consensus to develop a material with the following characteristics: content structured in chapters and specific to PD clinical features, accessible language, no regionalisms in the vocabulary, so that participants understand from all the national territory, creative layout, illustrations to begin each chapter in order to facilitate learning and provide more motivation for subjects to feel interested in reading.28
Design and diagramming of the images were performed by professionals and students of social communication and marketing at the Universidade de Fortaleza. All the images were originally created in Adobe Illustrator program. We had meetings to discuss the expressions and features of the disease and the adequacy of the figures.
The booklet is entitled ‘Living with Parkinson’ and has 90 double-sided pages with front and back pages. It contains cover, back cover, summary, pages for notes and 12 chapters. At the end of each chapter, there are specific review questions to answer and consolidate the learning. The final version of the booklet had dimensions of 210×297 mm.
Each chapter begins with an illustration telling a new event with the character who has PD and the chapter titles are a sentence from the patient.
During the sessions, participants will be allowed to discuss their experiences and difficulties. In the final section of each session, they will have to answer few questions related to the major topics presented in the day’s programme. The chapters’ titles are shown in table 1. There is a specific chapter that teaches home safe exercises and many other chapters also encourage the participants to be physically active.
Health education programme
Exercise group: exercising with elastic band and tubing
The exercise group will have four participants as in the control group. Muscle power is a measure of the ability to produce muscle strength quickly. PT is based in high-speed movement with low loads of resistance. The participants will be instructed to move as fast as possible during the concentric phase of each repetition and to move slower during the eccentric phase. To ensure the required movement speed of the exercises, the physical education professionals will say phrases to encourage like ‘faster, faster’, ‘go faster’ and touch the patient to make a neurosensorial feedback eccentric dynamic progressive resistance training.29 30 Each exercise session will last a maximum of 60 min, consisting of a 5-minute warm-up (dynamic stretching and mobility exercises), a 50-minute power training using elastic tubes (Lemgruber)31 or elastic bands (TheraBand),32 and a 5-minute cool down (stretching and relaxation exercises). Multiple-joint exercises will be performed prior to single-joint exercises.
Before the start of the PT regimen, we will perform the familiarisation period of 2 weeks to teach the participants to exert force as fast as possible during the concentric phase and move slower in eccentric phase. During the familiarisation period, researchers will also spend more time repeating instructions for the proper performance of participants and teaching the participants to use the Rating of Perceived Exertion (RPE) method using the Borg category ratio scale. This scale is known as a valid, simple rating instrument that assesses perceived exertion, identifying the intensity used at the time of training.33 We will use the RPE Scale from 0 to 10. The numbers relate to how easy or difficult participants classify an activity. During the intervention period, the training load will be based on the RPE method using the Borg category ratio scale.33
For each participant, a trained physical education professional or student will provide individualised training with supervision of the PT intervention coordinator. The prescription of the exercise intervention was elaborated by a specialised physiotherapist with expertise in PT. Each session consists of 9 exercises designed to stimulate different muscle groups, with 10 submaximal repetitions performed up to a predefined maximum time.
Other details are explained in the TIDieR checklist in online supplemental file 2.26 Resistance exercise regimes using elastic devices are detailed in table 2. Descriptors of the progression of the elastic devices protocol are detailed in table 3. The 12 items detailed in the checklist are an extension of the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement—item 5.34 The illustrations of the exercise protocol are available in online supplemental file 6. TheraBand is divided in colours, where each colour represents a different level of resistance. Six resistance levels (yellow, red, green, blue, black and silver) of TheraBand (Hygenic Co., Akron, Ohio, USA) will be used.32 The elastic tubing has different types of diameters and resistance. Five different elastic tubing sizes (Lemgruber; Brazil) will be used. The inside diameter (ID) and outside diameter (OD) of each pipe are described according to the manufacturer’s specifications: #200 (ID: 3.0 mm, OD: 5.5 mm); #201 (ID: 4.0 mm, OD: 5.5 mm), #202 (ID: 4.0 mm, OD: 8.0 mm), #203 (ID: 6.0 mm, OD: 9, 0 mm) and #204 (ID: 6.0 mm, OD: 11.5 mm). In this way, varied resistances are allowed, which provide great mobility and increased exercise intensity without excessive weight load.35
Supplemental material
Resistance exercise regime using elastic devices
Exercise progression
Upper body and low body (LB) exercises will be executed in two phases. Six weeks in level 1 and the last 6 in level 2. Level 2 exercises will have greater complexity of execution and greater muscle demand.
We will use the progression scale by the colours of TheraBand️ and diameters of elastic tubing Lemgrumber️ as shown in table 3. The progression will be individualised according to RPE Scale. When the RPE Scale is lower than 4, the researcher will increase the resistance of the elastic devices according to table 3 in the next session. Thus, to increase the intensity of the exercise in order to adjust the RPE values, the colour that was being used will be replaced by the next colour and the next diameter on the resistance scale, for example, changing from red to green elastic band TheraBand️ and from #200 to #201 elastic tubing Lemgruber️. For individuals who achieve the highest resistance (silver colour in TheraBand️ and #204 in tubing Lemgrumber️), another elastic band and tubing will be added, always following the order of progression (eg, gray+yellow; #204+#200).
Criteria for discontinuation
Participants will be requested to complete a minimum of 20 of the 24 scheduled training sessions (ie, >85% attendance) during the 12-week intervention period. If the patient misses a session, he or she will be provided an opportunity to complete an additional session to make up for the missed training. Compliance will be recorded using attendance sheets, which will be filled by the attending researcher, after each training session.
If an adverse event is thought to have a causal relationship with the intervention and raises concern about the participant’s safety, the intervention will be discontinued for the participant.
Strategies to improve adherence
Patient adherence will be encouraged in the prerandomisation recruitment consultation. Each patient will be reminded of the session by a telephone call on the day of the meeting. Patient frequencies will be recorded using REDCap. In case of absence, the Intervention Monitoring Committee (IMC) will contact the patient to clarify the reason for the absence and to reschedule the session. Leaving the session before completion and the reason will also be recorded. Adherence will be reported as a percentage of fully accomplished intervention sessions without protocol deviations given the total number of scheduled sessions (24 in exercise group and 12 in health educational group).
Relevant concomitant care and interventions
To ensure the only difference between the groups is the clinical trial intervention, participants will be instructed not to make any dietary changes or engage in any formal exercise programme during the study.
Outcomes
The outcomes will be measured 1 week prior to intervention and 1 week after intervention. All participants will be evaluated during ‘on’ phases of medication.
Primary outcome measures
Changes from baseline in motor MDS-UPDRS examination subscores for bradykinesia will be derived using an upper limbs bradykinesia subscore, derived by summing the MDS-UPDRS motor examination items 23, 24 and 25, and a lower limbs bradykinesia subscore, computed as the sum of MDS-UPDRS motor examination items 26, 27, 29 and 31. The Part III Motor Examination (MDS-UPDRS-III) is an 18-item instrument assessing the severity of PD motor symptoms. Each item is scored ‘0’–‘4’ on a categorical scale, with ‘0’ indicating no impairment and ‘4’ indicating severe impairment. Higher scores indicate severe motor disabilities.4
Changes from baseline in physical functional performance will be compared between the exercise and health education groups by using SPPB, which combines the gait speed, chair stand and balance test results. SPPB is a well-recognised tool to measure physical performance in population studies on elderly individuals. It consists of three tasks: a hierarchical balance task, a short walk at the usual speed and a five-repetition chair stand test. Low SPPB scores predict various health outcomes such as mobility loss, disability, hospitalisation, length of hospital stay, nursing home admission and death. The cut-off score for low performance is ≤8.36
Secondary outcomes
Neurological and neurophysiological outcomes
Changes in the total MDS-UPDRS scores will be compared between the exercise and health education groups. The MDS-UPDRS consists of four parts. Part I has 13 questions on non-motor experiences of daily living; part II has 13 questions on motor experiences of daily living; part III has 33 scores on 18 motor examination items (right, left and other body distribution scores) and part IV has 6 questions on motor fluctuations and dyskinesias. Six questions in part I dealing with complex behaviours and all questions in part IV dealing with fluctuations and dyskinesias involve the rater interviewing the patient or caregiver. The remaining 20 questions in parts I and II are to be answered by the patient/caregiver via a questionnaire without direct input from the rater. Part III involves objective examination by the rater for all items. This scale evaluates the signs, symptoms and certain activities of the participants through self-report and clinical observation. Each item is scored from ‘0’ to ‘4’ on a categorical scale, with ‘0’ indicating no impairment and ‘4’ indicating severe impairment. Higher scores indicate more intensive motor disabilities.37
Changes from baseline in Beck Depression Inventory—Second Edition (BDI-II) will be used to assess depression among the study participants. BDI-II is a 21-item self-report questionnaire to measure depressive symptoms. Each item is scored on a scale of 0–3, and the items are summed to yield a total score. A higher score is indicative of greater depressive symptoms. Total scores may range from 0 to 63. A score of ≥14 is suggestive of clinically significant symptoms.38
Changes from baseline in Parkinson’s disease quality of life scale (PDQ-39) will be compared between the exercise and health education groups. The PDQ-39 Questionnaire evaluates various aspects of quality of life in participants with PD. It is a self-administered questionnaire consisting of 39 items distributed across eight domains: mobility, activities of daily living, emotional well-being, stigma, social support, cognition, communication and body discomfort. Scores on this scale can vary between 0 and 100, with lower quality of life indicated by a higher score.39
Changes from baseline in the Stroop Test will be compared between the exercise and health education groups. The final version of this test consists of three cards, each containing six columns of four items in blue, green, pink and brown. The following tasks are proposed: card 1, naming stitch colours; card 2, naming neutral word colours and card 3 (interference card), naming the colour of words printed in different colours. The last task aims at inhibiting auto-read response and produce word colour naming. The test evaluates inhibitory control, selective attention and processing speed. The patient is evaluated according to how quickly he or she performs the task and the number of errors made. The effect of interference is determined by calculating the additional time required to name the colours (from the printout) compared with the time required to name the colours in the first colour-control task.40
Changes from baseline in the Mattis Dementia Scale (MATTIS) (Mattis, 1998) will be compared between the exercise and health education groups. The MATTIS consists of five subscales: attention, initiative/perseveration, construction, conceptualisation and memory. The reference values for classifying elderly individuals with or without impairment were adopted from the study by Foss et al. Impairment was defined as scores less than −2.0 SDs from age and education standards. This cut-off point determines a marked impairment of one or more cognitive functions to differentiate neuropsychological profiles with greater specificity. The use of MATTIS to screen dementia in PD is well documented.41
Changes in Pittsburgh Sleep Quality Index (PSQI) will be compared between the exercise and health education groups. PSQI provides an estimate of sleep quality in the past month. It is a self-administered instrument consisting of five questions to be answered by the subject’s roommates and is to be used for only clinical purposes and 19 self-administered questions grouped into 7 components (with weight distribution from 0 to 3). The seven components are subjective sleep quality, sleep onset latency, sleep duration, sleep efficiency, sleep disorders, hypnotic drug use and daytime repercussion. The scores on each component are summed to yield an overall value ranging from 0 to 21. An overall PSQI value of >5 indicates that the individual is experiencing major sleep difficulty if represented by at least two components or moderate sleep difficulty if represented by at least three components.42
Changes in Epworth Sleepiness Scale (ESE) will be compared between the exercise and health education groups. The ESE Questionnaire has eight questions that address the nature and occurrence of daytime sleep and sleepiness. ESE scores range from 0 to 24, with a score of >10 considered as excessive sleepiness.43
Change in Parkinson’s Disease Sleep Rating Scale (PDSS) will be compared between the exercise and health education groups. The PDSS is a visual analogue scale addressing 15 commonly reported symptoms associated with sleep disturbance, with each symptom having a score of 0–10.44
Change in rapid eye movement (REM) sleep behaviour disorder screening questionnaire, which consists of 13 items, with ‘Yes’ or ‘No’ as answers, about clinical characteristics of sleep and dreams. Questions can be answered directly by the patient or by his or her bed partner. It is a self-applicable questionnaire.45
Change in the rate of respiratory disorders (apnea and hypopnea) and sleep atony during the REM phase are assessed using electroneuromyography, with a sensor attached to the chin muscles. Change in sleep quality is measured by the deepest sleep phases (N3 and REM) and the most superficial phase (N1). These sleep parameters will be assessed through video polysomnography (PSG), a diagnostic method for monitoring sleep. A definitive diagnosis of REM sleep behaviour disorder (RBD) is necessary to exclude other sleep disorders mimicking RBD. In addition, PSG is essential in evaluating sleep parameters and diagnosing obstructive sleep apnea (OSA).
The characteristic polysomnographic finding of RBD is the absence of atony in REM sleep, an elevation of motor tone during REM sleep as measured by electromyography (EMG) with the leads placed in the chin and/or limbs, and/or the presence of abnormal changes in this REM sleep. Diagnosis can be confirmed on the basis of sleep history or dream enactment behaviours as observed on video PSG via time-synchronised audio equipment.
Polysomnographic examination to evaluate RBD must include complete assembly on the electroencephalogram (international system 10–20), nasal pressure transducer, oral thermostat/thermopower, chest and abdominal respiratory belts, pulse oximetry and EMG bilateral chin and tibial musculature, synchronised audiovisual system and EMG recording in the upper limbs.
Before the examination, the patient is informed about the procedure, such as placing electrodes and the possibility of summoning the technician in case of any difficulty. Before and after the examination, a questionnaire is administered to identify the factors influencing the performance and interpretation of the examination, such as a bad night’s sleep with many awakenings. During the examination in the laboratory, the technician must note any abnormalities or suspicious movements that occur during sleep.46
According to the American Academy of Sleep Medicine sleep scoring manual, the polysomnographic criterion for diagnosing RBD is the presence of increased tonic and/or phasic activity during at least one 30-second epoch of REM sleep. It includes one or both of the following situations:
Sustained muscle activity (tonic activity), defined as a chin EMG amplitude of ≥50% the minimum amplitude during non-REM sleep.
Excessive transient muscle activity (phasic activity), defined as chin or limb EMG amplitude at least four times higher than background EMG activity during 0.1–5.0 s bursts in at least five of the ten 3-second mini-epochs.
For the diagnosis of OSA, we compute the Respiratory Disturbance Index, which is the number of respiratory events during sleep divided by the total sleep time. If this index is >5 events/hour in a symptomatic patient, the diagnosis of OSA is confirmed. In addition, PSG can verify the proportion of different sleep phases and the number of awakenings.
Changes in actigraphy sleep patterns from baseline will be compared between the exercise and health education groups. Actigraphy uses a small portable device (actigraph) that senses physical motion and stores the resulting information. Actigraphy test has been predominantly used in research studies to evaluate rest–activity cycles in participants with sleep disorders, determine circadian rhythm activity cycles and ascertain the treatment effectiveness. The actigraph is typically worn on the wrist, but it can also be worn on the ankle or the trunk of the body. Actigraphy test is based on the assumption that movement is reduced during sleep compared with wakefulness and that activity level can be used as a diagnostic indicator for sleep disorders. Data are expressed graphically as actograms or reported numerically as total activity counts per epoch. The test estimates sleep latency, total sleep time, number and frequency of awakenings and ‘sleep efficiency’. Actigraphy results has been proposed as a diagnostic parameter for several sleep disorders, including insomnia, restless leg syndrome/periodic limb movement disorder, circadian rhythm disorders and sleep apnea.46 In this study, for actigraphy, we will use the ActTrust by Condor Instruments.47
Physical functional performance outcomes
Changes from baseline in the five times sit-to-stand test (FTSTS) will be compared between the two groups. For the FTSTS, participants will have to sit in an armless chair with a seat height of 43 cm. The participants will be instructed to cross their arms over their chest and sit with their back against the upright backrest of the chair, with feet flat on the floor and knees at 90°. Subsequently, they will be instructed to quickly and repeatedly rise to a full standing position and then sit down five times. A single repetition will be defined as attaining a vertical standing position with an upright trunk, with hips and knees extended. The test will begin once the participant moves off the chair for the first stand and will finish once the participant sits following the fifth sit-to-stand (STS) repetition. The total time to complete the test is recorded in seconds. The cut-off point for low strength on FTSTS will be 15 s.48
We will also calculate the STS velocity and STS muscle power and measure the changes from baseline between the two groups. Alcazar et al49 proposed an equation to measure the STS velocity and muscle power by using the body mass and height of the subject, height of the chair and the time needed to complete five STS repetitions. The equations are:


Changes from baseline in handgrip strength will be compared between the exercise and health education groups. The participants will be tested after one research team member demonstrates proper device use and body positioning; the standard testing position approved by the American Society of Hand Therapists50–52 is as follows:
Set the handle at the second position (3.8 cm).53
Sit in a straight-backed chair with the feet flat on the floor.
Adduct and neutrally rotate the shoulder.
Flex the elbow to 90°.
Keep the forearm in a neutral position.
Hold the wrist between 0° and 30° extension and between 0° and 15° ulnar deviation.
In all cases, the arm should not be supported by the examiner or by an armrest.
The dynamometer should be presented vertically and in line with the forearm to maintain the standard forearm and wrist positions.54
Precede the test with three submaximal warm-ups at 50%–75% of perceived maximum effort.
Perform three trials with a 60-second recovery period between the trials.55
Each trial should last for 3 s.
PD asymmetry should be considered such that bradykinesia, rigidity and tremor may be present unilaterally or bilaterally. This is the reason to consider the greater handgrip strength, as was considered by Vetrano et al . The cut-off point for low grip strength is 27 kg for men and 16 kg for women.56
Changes in the 4-Metre Gait Speed Test will be compared between the exercise and health education groups. Gait speed (GS) will be measured using the time required for the participant to walk 4 m on a track at a self-determined pace. GS will be calculated in metres per second for each patient. The average value of the results from the two tests will be used. The cut-off point of low performance is ≤0.8 m/s.57
Changes in Fall Efficiency Scale—International (FES-I) will be compared between the exercise and health education groups. FES-I, the most reliable tool for assessing fear of falling in participants with PD, will be used.58 The participants will have to answer their concern levels of falling on performing 16 activities mentioned in the scale. Answer options are scored from 1 to 4, with 1 indicating not worried; 2 indicating a little worried; 3 indicating moderately worried and 4 indicating very worried. The FES-I score ranges from 16 to 64, with higher scores indicating greater fear of falling.59
Changes from baseline in muscular performance of the knee extensor and knee flexion will be compared between the exercise and health education groups. Isokinetic dynamometry (Biodex System 4 Pro, Biodex Medical Systems, New York, USA) will be used to determine knee extension and flexion strength. The isokinetic variables peak torque (Nm), work (joule), average power (watt), rate of torque development (Nm/s), all of them normalised by the subject’s body mass, will be used.60 The chair will be tilted at 85°. The thigh, pelvis and trunk will be adjusted using the straps provided in the equipment. The rotational axis of the device will be aligned with the lateral epicondyle of the femur, and the lever cushion will be positioned 3 cm above the lateral malleolus. Measurements of both legs will be obtained. The dominant side and the side most affected by PD will be analysed. The tests will consist of five maximal repetitions at 60°/s and 15 repetitions at 180°/s, with a rest period of 1.5 min between each evaluated speed. A 2-minute rest will be provided between the tests. During the test, the researchers will motivate the participant by using phrases such as ‘strength, strength, strength’, ‘try to hit the top’, ‘try to hit the bottom’, ‘move fast’, in addition to clapping. Calibration of the equipment will be performed according to the manufacturer’s specifications before every evaluation.
Changes in the rate of torque development from baseline will be compared between the exercise and health education groups. The Biodex System 4 Pro dynamometer will be used for the test, which consists of five maximal repetitions at 60°/s and 15 repetitions at 180°/s. A rest period of 1.5 min between each evaluated speed isotonic contractions of the leg-extensor muscles will be provided. Participants will be instructed to kick as fast as possible against different (relative) loads. The rate of torque development (Nm/s) is defined as the linear slope of the power-time curve and is measured from the onset of movement until peak power.60
Changes in fall history between the month preceding baseline and the month following the training period will be compared between the exercise and health education groups. Information on the number of falls and fall-related injuries will be obtained through interviews.61
Changes in physical activity, physical activity intensity and sedentary behaviour, as measured by actigraphy, will be compared between the exercise and health education groups. The time spent in moderate-to-vigorous physical activity (min/day) will be measured by accelerometry (actigraph) for 12 weeks. The accelerometer measures sedentary time and physical activity by assessing the magnitude of the body’s acceleration in terms of ‘counts’ per unit time. It will also measure the average daily number of steps in 24 hour/day for 12 weeks.62
Change in the New Freezing of Gait Questionnaire (N-FOGQ) score between the exercise and health education groups. N-FOGQ is a reliable tool for detecting and evaluating the impact and severity of gait freezing. It was developed based on the FOGQ by Giladi et al63 for participants with PD. The N-FOGQ64 consists of three parts: part I, which determines the presence of gait freezing using a dichotomous item in which individuals are characterised as ‘freezer’ (FR) or ‘not freezer’ according to the episodes of freezing that have occurred in the previous month. Parts II and III are designed only for FRs, providing a total score between 0 and 28. Part II (items 2–6, scores range from 0 to 19) rates the severity of freezing of gait (FOG) on the basis of its duration and of its frequency during the gait and the beginning of the gait. Item 2 was added to assess the overall frequency of the FOG, regardless of the circumstances. No items were added to the duration of all forms of FOG, recognising the difficulties in estimating the duration of FOG globally. Part III assessed the impact of FOG on daily life (items 7–9, scores ranging from 0 to 9).
Changes from the baseline in the score of the SARC-F sarcopenia questionnaire will be compared between the exercise and health education groups. The SARC-F Questionnaire will be completed by the participants during their stay at the clinic. This questionnaire includes five questions that are to be rated from 0 to 2, allowing for a maximum score of 10. According to the literature, the presence of sarcopenia is indicated by a score of ≥4. This screening tool includes questions about falls, assistance to walk, general strength, rising from a chair and walking on stairs as markers of the responder’s risk of developing sarcopenia.65
Change in the dynamic body balance, as measured using the Mini-Balance Evaluation Systems Test (Minibestest), will be compared between the exercise and health education groups. The Minibestest is a reduced version of Balance Evaluation Systems Test that can be applied to participants irrespective of age and disease severity. It consists of four domains: anticipatory, reactive postural control, sensory guidance and gait, with a variation of an ordinal scale of 3 points (‘0’, indicates severe; ‘1’ indicates moderate and ‘2’ indicates normal) and a maximum score of 28. The higher the score, the better the performance.66 In each of the 14 items evaluated, the participant will be instructed to perform certain activities under several specific functional conditions, according to the order requested, as described below67 :
Seated to standing: on command, move from sitting to standing, with arms crossed, standing without using hands, unless necessary; legs should not touch the chair when standing.
Standing on tiptoe: position the feet shoulder-width apart, stand on tiptoe, with the hands on the hips and look straight ahead, for 3 s.
Standing on one leg: standing with one leg support, without touching one leg on the other, with hands on the hips, looking ahead, as long as possible.
Correct with compensatory step forward: stand with feet shoulder-width apart and arms at the sides. Lean forward against the appraiser’s hands, beyond the previous limits. The evaluator will then release the patient, who must try to maintain the balance, taking measures to prevent a fall.
Correction with compensatory step back: stand with feet shoulder-width apart and arms at the sides. Lean back against the appraiser’s hands, beyond the posterior limits. The evaluator will then release the patient, who must try to maintain balance, including taking measures to prevent a fall.
Correction with compensatory step on the side: stand with feet shoulder-width apart and arms at the sides. Lean to the side (right and left) against the evaluator’s hands, beyond the lateral limits. The evaluator will release the patient, who try to maintain balance, including taking measures to prevent a fall.
Eyes open, firm surface (feet together): place the hands on the hips and look straight ahead. Each time remain as stable as possible until the evaluator asks to finish (normally 30 s).
Eyes closed, foam surface (feet together): place the hands on the hips and look straight ahead. Each time remain as stable as possible until the evaluator asks to finish (normally 30 s).
Inclination—eyes closed (time in seconds): stand on an inclined ramp with the toes pointed toward the top of the ramp. The feet should be shoulder-width apart and hands should be on the hips. Stand in this position with eyes closed. The appraiser will measure the standing time.
Change in GS: begin walking at a normal speed. When the evaluator says ‘fast’, begin walking as fast as possible. When the evaluator says ‘slow’, begin walking very slowly.
Walking with head turned horizontally: begin walking at normal speed. When the evaluator says ‘right’, turn your head and look to the right; when the evaluator says ‘left’, turn your head and look to the left. Try to keep walking in a straight line.
Walk and turn on the axis: begin walking at normal speed. When the evaluator says ‘turn and stop’, turn as fast as possible to look in the opposite direction and stop. After turning, the feet should be placed close together.
Pass over obstacles: begin walking at normal speed. On reaching the box placed on the route, go over it, not around it, and continue walking.
Get up and go timed with double task (TUG; TUG double task): TUG: when the evaluator says ‘go’, get up from the chair, walk at normal speed through the tape on the floor, turn and return back to sit on the chair. Dual task TUG: count down from 3 to 3, starting from 90 to 100. When the evaluator says ‘go’, get up from the chair, walk at normal speed through the tape on the floor, turn and go back to sit on the chair. Continue counting down all the time.
Materials:
A firm chair without armrests or casters.
Tempur/T-foam: 10 cm high foam, medium density T41 (firmness rating).
10° inclination ramp.
Stopwatch.
22.9 cm high box (eg, two shoe boxes stacked and fastened together).
Tape to measure and mark the floor: 3 m away from the chair.
Control variables
Blood parameters
Blood samples will be collected to assess complete blood count; fasting serum levels of urea, creatinine, sodium, potassium, calcium, glucose, cobalamin, thyrotropin, 25-hydroxy-vitamin D and HbA1c.
Anthropometric assessment
A calibrated scale and an analogue stadiometer will be used to assess weight and height, respectively. For this assessment, the study participant should wear light clothes and no shoes. In addition, the waist circumference will be assessed in the horizontal plane midway between the lowest ribs and the iliac crest, as is suggested by the WHO68 and the International Diabetes Federation.69 We will also measure the mid-up-arm circumference and calf circumference according to the International Standards for Anthropometric Assessment by ISAK.70
Sample size
The sample size registered in the Brazilian clinical trials registry was 50 participants so that is suitable for the two primary outcomes below.
Bradykinesia subscore MDS-UPDRS motor examination
G*Power71 analysis was used to determine the a priori sample size. One-way analysis of covariance (ANCOVA) will be conducted to examine the between-group differences (Elastic exercise vs Health education) in bradykinesia improvement over the course of the study, as is indicated by the MDS-UPDRS change scores (post-test minus baseline) after controlling for pre-test values. To obtain an estimate of the expected effect size, we consulted a study similar to our proposed investigation in which 14 participants with PD and 10 healthy control subjects completed 12 weeks of supervised resistance training aimed at improving neuromuscular function, as indicated by changes in UPDRS scores of upper limbs and lower limbs bradykinesia. The authors used the one-way ANCOVA design similar to that proposed by us and reported an average effect size (Hedge’s g) of −1.06 for upper and LB bradykinesia change scores.4 72 73
Although we established an expected effect size for the sample size analysis on the basis of literature review, the G*Power software requires estimated effect sizes to be imputed as an f statistic. Therefore, we recomputed the study’s reported effect size to Cohen’s d, and transformed the value from Cohen’s d to an f statistic. Hedge’s g is a correction made to Cohen’s d estimates when the total number of subjects is <20. By inverting the formula for converting Cohen’s d to Hedge’s g, we get:

where J(df)=1−34df−1, and (df)=total number of subjects–number of groups.
On applying this formula, we obtain an estimated effect size (Cohen’s d) of −1.0978. Finally, this estimated effect size was converted from Cohen’s d to f by using the formula:

where k=number of groups.
This resulted in an estimated f effect size of −0.549. Last, we applied the absolute value of our effect size to the G*Power software as this program accepts only positive effect size values for a priori calculations of the sample size. Considering an estimated effect size (f) of 0.549, a study design involving two groups, one covariate and a significance threshold of p<0.05, we must recruit 29 subjects to ensure a post-hoc statistical power of at least 0.80. To control for an anticipated dropout rate of 20%, a total of 35 subjects should be recruited. Assuming 20% loss, two participants are additionally added per group, amounting to 24 participants per group.
Short Physical Performance Battery
The sample size was estimated considering a two-tailed significance level of 0.05, acceptable type II error of 0.2 and randomisation ratio of 1:1. The mean differences and the SDs from the study by Nocera et al74 were applied to calculate the sample in the G*Power software. We chose this study because the authors studied the effect of PT SPPB scores in participants with PD, the same outcome as proposed in our study. The provided parameters had significance level of 0.05, SD of 1.33, power of 0.8, difference in means of 1.72.
In total, 10 participants will be recruited to this two-treatment parallel-design study. The probability of the study detecting a treatment difference at a two-sided 0.05 significance level is 81%, if the true difference between the treatments is 1.72 units. This value is based on the assumption that the SD of the response variable is 3.5. Assuming 20% loss, 2 participants will be added per group, amounting to 24 participants.
Recruitment
Data on participants with PD meeting the study inclusion criteria will be obtained from an existing research database of the hospital’s movement disorder outpatient clinic. Participants meeting the eligibility criteria will be telephonically contacted for participation, and those consenting will be screened telephonically. The screened participants will be provided an appointment to confirm the eligibility and allow for completion of the informed consent. Because the possibility of the Brazilian public health system offering non-pharmacological treatment is considerably low, participants are genuinely interested in such opportunities. To defray costs for the participants, subsidies will be offered for transportation.
The recruitment period will begin in July 2020 and will continue until the calculated sample size is reached.
Allocation
The number sequence will be password protected on a computer operated by the research assistant. The hard copy of the allocation list will be kept in a sealed opaque envelope inside a locked safe. The assessors and data analysts will be unaware of the allocation until the end of the study.
Randomisation
Randomisation will be conducted by an external research assistant, who will not participate in any other clinical trial function, to keep the data management personnel and the statistician blind to the study conditions. The randomisation list will remain with the research assistant for the duration of the study. Therefore, randomisation will be conducted without any influence of the principal investigators, raters or therapists. Stratified randomisation by sex and MDS-UPDRS III will be performed in blocks of eight (four participants per block). According to the intention-to-treat (ITT) principle,75 all randomised participants, including the dropouts, will be included for final evaluation.
Blinding
Considering the nature of interventions (exercise and health education), a double-blind design will not be possible for therapists and participants. However, outcome assessors and the statistician will be unaware of the participant group. All participants will be advised not to inform the intervention they received to the assessors during the post-test.
In the case of unintentional breaking of the blindness for any reason, it is mandatory that the researchers involved notify the centre coordinator. In such cases, the participant’s identification, date and unblinding circumstance will be documented for internal control.
Data collection methods
A manual of operating procedures has been written to increase the implementation consistency of the assessments and intervention. In addition, standard-operating-procedure (SOP) documents are available for each assessment. Data Collection of Outcome Committee (DCOC) will be trained, and they will use the short version of the SOP during each data collection. They will meet before the trial onset to consolidate data collection procedures. Periodic meetings and written communication are established to promote internal transparency and consistency.
All variables will be assessed at baseline (1 week prior to randomisation) and 1 week after the intervention.
All randomised participants who are prematurely discontinued from study for any reason will follow the same schedule of events as those who continue study treatment except adherence assessment.
Data management
The study data will be collected and managed using the REDCap electronic data collection76 and management tool hosted at the Clinical Research Unit of the UFC. The original study forms will be entered in REDCap. The study has obtained licence agreement from the International Parkinson and Movement Disorder Society Rating Scale. The participants’ files will be stored in numerical order at a secure and accessible place. These files will be maintained in the storage for a period of 5 years after study completion.
Description of hardware at DCOC
The computer that will be used for randomisation and statistical analysis will be in the clinical research unit of the HUWC with restricted access. Only people with institutional badges can enter the facility. Users can enter the desktop with a valid password.
Statistical analysis
Baseline differences in demographic and clinical characteristics between the exercise and healthy education groups will be described in a table format.
We will perform all analysis by ITT and per-protocol (PP) approaches. For repeated measures effect sizes, generalised linear models or analysis of variance will be carried on as made for our sample size calculation. We do not plan any adjusted analysis by confounding factors assuming that randomisation will be sufficient to distribute them equally between groups. No inferential analysis will be carried on for baseline characteristics (ie, table 1) and 95% CIs will be provided whenever possible.
Two analyses will be carried out1: an ITT analysis; including all randomised individuals, and2 one PP, including all subjects who completed the study (concluding) with adherence to at least 85% of intervention sessions (≥20 sessions for participants allocated in the exercise programme and ≥10 sessions for participants allocated to the educational programme). We will qualitatively document reasons and details of withdrawals for each case. No interim analyses are planned.
Continuous variables will be reported at each endpoint of the study, by arithmetic or geometric means, SDs, 95% CIs and IQRs, as appropriate. Post-intervention changes will be summarised descriptively along with its 95% CI. Considering the missing values for imputation models in the ITT analysis, the last carried observation forward model will be employed to impute them. Categorical variables at baseline and after intervention (if applicable) of each group will be summarised in absolute numbers and proportional of participants (%) with 95% CI.
For categorical data such as adverse events, we did not plan any inferential analysis.
Statistical procedures are intended to be carried on in Stata and R.
Subgroup analysis
We propose to perform analysis of the two subgroups: participants aged 40–60 years and participants aged ≥60 years. This sub-analysis is justified because age is a factor that influences outcomes.77
Statistical methods: analysis population and missing data
Our main purpose is to test the superiority of exercise by using two analytical sets: the ITT set,75 considering all participants as randomised regardless of whether they received the randomised treatment, and the PP set. Criteria for determining the ‘PP’ group assignment will be established by the Steering Committee (SC) and approved by the Data and Safety Monitoring Committee (DSMC) before the trial begins. These analyses should agree closely if few participants are lost to follow-up.
Data monitoring: formal committee
Considering the possibility of loss of participants due to side effects, clinical complications or other unforeseen reasons, we will assess whether additional group is needed according to missing data standards.
Therefore, we will qualitatively document the reasons and details of each participant. In the case of identifiable patterns that indicate that the missing data are non-ignorable, the interpretation of the related findings should take into account the missing data. No interim analyses other than monitoring of demographic data will be performed.
The statistician will report to the independent DSMC. The DSMC will have unblinded access to all data and will discuss the results of missing data with the SC in a joint meeting. The SC will decide on the additional groups and will report to the Broad Ethics Committee of HUWC. The trial will not be stopped in case of futility, unless the DSMC, during the course of safety monitoring, advises otherwise.
Harms
All participants will be instructed to report adverse events throughout the study period. The interventions will be monitored by a geriatrician and a DSMC that will record any symptoms or injuries. All adverse events will be assessed by the research team for severity, expectation and causality in accordance with the National Council for Medical Research in Health guidelines (https://www.nhmrc.gov.au/guidelines-publications/e112). In this study, an adverse event will be defined as any unfavourable or unintended medical occurrence related to health (signal, symptom, syndrome, disease) that develops or worsens during the study period. Adverse events will be monitored by the physician of IMC until resolution or stabilisation is achieved or until it is demonstrated that the study intervention is not the cause of the injury. Participants can contact the research team immediately on the provided cell phone numbers in case of a serious adverse event. Any adverse events that occur during the exercise programme will be recorded by the DSMC, which will monitor the interventions and report immediately to the SC. The DSMC and SC will meet to discuss the seriousness and causality of the adverse event along with any medical team handling the event. A serious adverse event that is considered related or suspected to be related to the exercise intervention will be reported to the Broad Ethics Committee of HUWC.
Auditing
If necessary, an audit of the HUWC clinical research unit will be called for. The team will be independent of the team of researchers in this study.
Ethics and dissemination
The study is approved by the Broad Ethics Committee of HUWC and all participants will provide their written informed consent (register number 91075318.1.0000.5045).
We are committed to disseminating the methods and conclusions of the PARK-BAND Study to the interested research groups. Therefore, our disclosure plan after completion of the study covers the following1: scientific meeting with residents, students, assistant doctors and researchers of HUWC in which the present study design, results and interpretation will be presented2 ; provide written communications to journalists and address the general public3; provide a plain summary report of results to the participants and4 prepare manuscripts. For the manuscripts, criteria authored by the PARK-BAND Study will follow the recommendations of the International Medical Journal Editors’ Committee and those defined by the destination journals. Because we have established a relatively large group of multiple authors, some of the publications will be authored by a group called the PARK-BAND Study Group. When sending a manuscript authored by the PARK-BAND Study Group, line authors will be defined primarily by full-time equivalents of workload in evaluation activities. To that end, we will conduct weekly monitoring of the researchers’ entire workload base. To ensure the integrity of the reports, the manuscripts written by the PARK-BAND Study Group must adhere to the CONSORT statement or, if applicable, more appropriate reporting guidelines.
Patient and public involvement
The participants and the public were not involved in the design, or conduct, or reporting, or dissemination plans of the research.
Protocol amendments
If there is a change in the protocol that could affect the study results, the potential patient benefits or patient safety, or changes in the study objectives, study design, study population, sample size, study procedures or significant administrative aspects, the change will be made only after a formal amendment to the protocol. This change has to be agreed by the DSMC and approved by the Broad Ethics Committee of HUWC before implementation.
Minor administrative changes to the protocol that do not affect how the study should be conducted will be agreed by the DSMC and a memorandum will be submitted to the Broad Ethics Committee of HUWC.
Consent or assent
The recruiting medical team will present the study details to the participants, who will receive a sheet with all information and a video with guidance on the study’s outcomes. The recruitment team will apply the consent form.
The recruitment team will encourage participants put forth their doubts and assure them that their privacy will be preserved, and they are free to withdraw from the study anytime.
Confidentiality
All information of the study participants will be stored in a locker in an area with limited access. All laboratory samples, reports, data collection, and process and administrative forms will be recognised by an identification number to maintain confidentiality. The database will be registered and stored in REDCap, with password protected access systems. Forms, lists, logbooks, diaries and other listings that link the participant’s identification number to other identification information will be stored in a separate locked file in an area with limited access.
Declaration of interests
ESTS is supported by PDCTR (CNPq/FUNCAP)—EDITAL 07/2018. SBA benefits from the scholarship of the UFC doctoral programme in medical science by FUNCAP.
Access to data
All principal investigators will have access to the clean data sets. The project data sets will be hosted on the REDCap, to which the project’s principal investigators will have direct access through a valid password.
Ancillary and post-trial care
The study participants will continue to be assisted at the movement disorders outpatient clinic of HUWC by a team of neurologists and geriatricians.
Dissemination policy: trial results
Our purpose is to dedicate our efforts to reduce the interval between the completion of data collection and the dissemination of study results to an absolute minimum. We expect to take about 3–4 months to prepare the document of final results for an appropriate journal. The results of the study will be released to participating physicians, referring doctors, participants and the medical community.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @helal_lucas
Correction notice This article has been corrected since it was published. Author name has been changed from Vlademir Gomes Carneiro to Vlademir Carneiro Gomes.
Contributors PB-N conceptualised the project and received funding. DPL, SBdA and JdCB were involved in designing the project. DPL and JdCB will be involved in the project implementation. ESTS will supervise the collection of outcomes. SBdA, along with VGC, will be involved in exercise intervention. LAOL supervised SBdA in developing an exercise protocol using elastic devices. PGD will apply neurological scales and interpret polysomnography. MASN will be involved in analysis and interpretation of data. ABVJ will perform statistical analysis of the data and randomisation. MSdA and JRGdL will coordinate the recruitment of participants meeting the eligibility criteria. JS helped with designing the project, statistics and exercise intervention. LH helped with designing and reviewing the project. ALdCG will be responsible for monitoring the intervention on recording of frequency, side effects and vital signs. PGBR and IdSP will record the results of the outcomes in the Redcap. ECBC and LMdO will collect data on physical performance, body composition and responses to other questionnaires. TAdMC and RRM will organise health education meetings. All authors helped draft the manuscript, read and approved the final version of the manuscript.
Funding Material support and scholarship grant for ESTS, SBdA, PGBR and IdSP: CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico), CAPES (Fundação Cearense de Apoio Coordenação de Aperfeiçoamento de Pessoal de Nível Superior), FUNCAP–PDCTR (Fundação Cearense de Apoio–Programa de Desenvolvimento Científico e Tecnológico Regional (CNPq/Funcap)—EDITAL 07/2018 files’ numbers DC8-0145-00070.01.00/18 and 9917237/2018.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.