Article Text

Abstract
Objectives The study aimed to understand through qualitative research what patients considered material in their decision to consent to an acute surgical intervention.
Participants, setting and intervention The patients selected aged between 18 and 90, having been admitted to a major trauma centre to undergo an acute surgical intervention within 14 days of injury, where English was their first language. Data saturation point was reached after 21 patients had been recruited. Data collection and analysis were conducted simultaneously, through interviews undertaken immediately prior to surgery. The data were coded using NVIVO V.12 software.
Results The key theme that originated from the data analysis was patients were unable to identify any individual risk that would modify their decision-making process around giving consent. The patient’s previous experience and the experience of others around them were a further theme. Patients sensed that there were no non-operative options for their injuries.
Conclusion This is the first study investigating what patient considered a material risk in the consent process. Patients in this study did attribute significance to past experiences of friends and family as material, prompting us to suggest that the surgeon asks about these experiences as part of the consent process. Concern about functional recovery was important to patients but insufficient to stop them from consenting to surgery, thus could not be classified as material risk.
- medical law
- surgery
- orthopaedic & trauma surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study examining what patient considered to be a material risk in the consent process through qualitative analysis.
The interviews were shorter compared with other qualitative ones as they were preoperatively, which limits the time for in-depth interviews.
This study provides early data about the challenges of the application of the Montgomery ruling to surgical practice.
Introduction
The 2015 Supreme Court decision in favour of Nadine Montgomery v Lanarkshire Health Board1 was a paradigm shift in the legal framework relating to negligence, consent and risk disclosure throughout all specialties in the UK and, to some degree, internationally.2 Ms Montgomery’s child suffered a shoulder dystocia during labour, which resulted in a 12 min period of acute hypoxia resulting in him suffering from cerebral palsy. She sued for negligence arguing that she would have requested a caesarean section had her obstetrician informed her of her personally increased risk of shoulder dystocia, based on her known risk factors.3
Before the Montgomery ruling, the legal test for adequacy of risk disclosure concerning medical negligence was the Bolam test.4 The Supreme Court ruled in Ms Montgomery’s favour and declared that doctors should ensure patients are aware of any risks material to them. “The test of materiality is whether in the circumstances of the particular case the court is satisfied that a reasonable person in the patient’s position would be likely to attach significance to the risk.”5 Defining material risk in more objective terms is problematic; however, it has been suggested that 1:1000 risk would not have been material.5 The Montgomery ruling has been described as ‘the most important UK judgment on informed consent for 30 years’6 and resulting in new guidance by the Royal College of Surgeons7 and there has been anecdotal evidence of ‘cases coming through the clinical negligence system of solicitors referring to the Montgomery ruling’.8
Despite being an obstetric ruling, the Montgomery ruling applies to all medical and surgical specialties. There is much published opinion and theory on this topic,2 3 9–25 but currently, little research,26 27 especially in trauma surgery, looking at what patients attribute significance to when providing consent and therefore what common material risks may exist in the specialty. An understanding of any common material risks will help guide the consenting surgeon to apply the Montgomery ruling to their practice.
The objective and individual understanding of consent process is complex and dependent on the perspective of the parties involved, with marked differences between patients and clinicians.28 29 The respective roles have changed over the last 20 years from a doctor paternalistic model to a patient autonomous decision-making.30 Noteworthy, the mismatch between patient’s and clinician’s perspective has been observed in percutaneous coronary interventions.31
This is a qualitative study of patients of the acute trauma and orthopaedic admissions in a large trauma centre in the North of England. It attempts to identify the common material risks from the patient’s perspective, or types of material in relatively simple trauma operations by interviewing post consent, but preoperatively. The hypothesis was that patients would be unable to vocalise what they considered a material risk.
Patients and methods
Ethics
In advance of each interview, informed written consent was obtained from participants. This included the fact that patients could refuse consent, or withdraw consent at any time with no impact on the healthcare provided to them. Each patient was given an anonymous identifier number. Audio recordings were recorded on a secure device, transcribed on the day of the interview and then the raw audio files were deleted. The Consolidated criteria for Reporting Qualitative research was completed (see figure 1).

The Consolidated criteria for Reporting Qualitative research (COREQ).
Data collection
The study population of patients was selected from the acute trauma and orthopaedic taken from a northern major trauma centre. Patients who met the inclusion/exclusion criteria during the morning trauma meeting (where each patient on the opearative lists for that day are discussed)were selected. The consenting surgeons were unaware of the study and consented the patient before knowing they were going to be subject to a data collection interview. Multiple different surgeons consented the patients involved in this study.
The study adopted the following inclusion: aged 18–90; operation within 14 days of injury; ‘Simple’ trauma injuries—defined as definitive treatment of injury in a single surgical procedure (eg, wrist or ankle fractures); English as first language; able to provide consent for the operation with a consent form 1. Exclusion criteria included unable to consent for any reason; impaired cognitive function (defined as MMSE less than 8); polytrauma; first procedure of any of the operative trauma lists (in order to minimise disruption to the clinical team). These criteria aimed to exclude patients who could not consent, were unable to have an informative discussion within an interview context, exclude consent processes involving multiple procedures/operations and to be minimally disruptive to the clinical team.
Patients were then approached and consented to participate in the study by the lead researchers, where the purpose of the study was explained on the hospital ward. The exploratory qualitative approach used semistructured interviews in order to gather data. These bedside interviews were conducted after consent was taken, but preoperatively alone by either JW or AH, predoctorate and postdoctorate researchers. This was to capture patients’ views when consenting surgeons were legally required to elicit, discuss and disclose material risks. An interview topic guide was used to initiate and develop conversation into the factors that patients feel are important before signing a consent form (table 1, online supplementary material 1), previous and current positive and negative experiences of consent, and to assess any material risks. The single stage interviews were exploratory in order to elicit material risks. Questions that came up repeatedly to look for these included open questions, such as “what was important to you when you gave consent to this operation?”; closed questions such as “are there any of the risks on the consent form that are particularly important/significant to you?,” or “were there any of the risks on the consent form that would have changed your decision making?,” and directly explaining the Montgomery ruling to the patient and asking for their reflections as a patient consented to and awaiting an operation in relation to this. The interviewer was a medical doctor independent of the clinical team responsible for the patient’s care. Interviews lasted 35–50 min including purpose of the interview, clarification of topic under discussion and format of the interview.32 The interviews were usually conducted at the bedside.
Supplemental material
Examples of semistructured interview questions
Patient and public involvement
No patient involved.
Data analysis
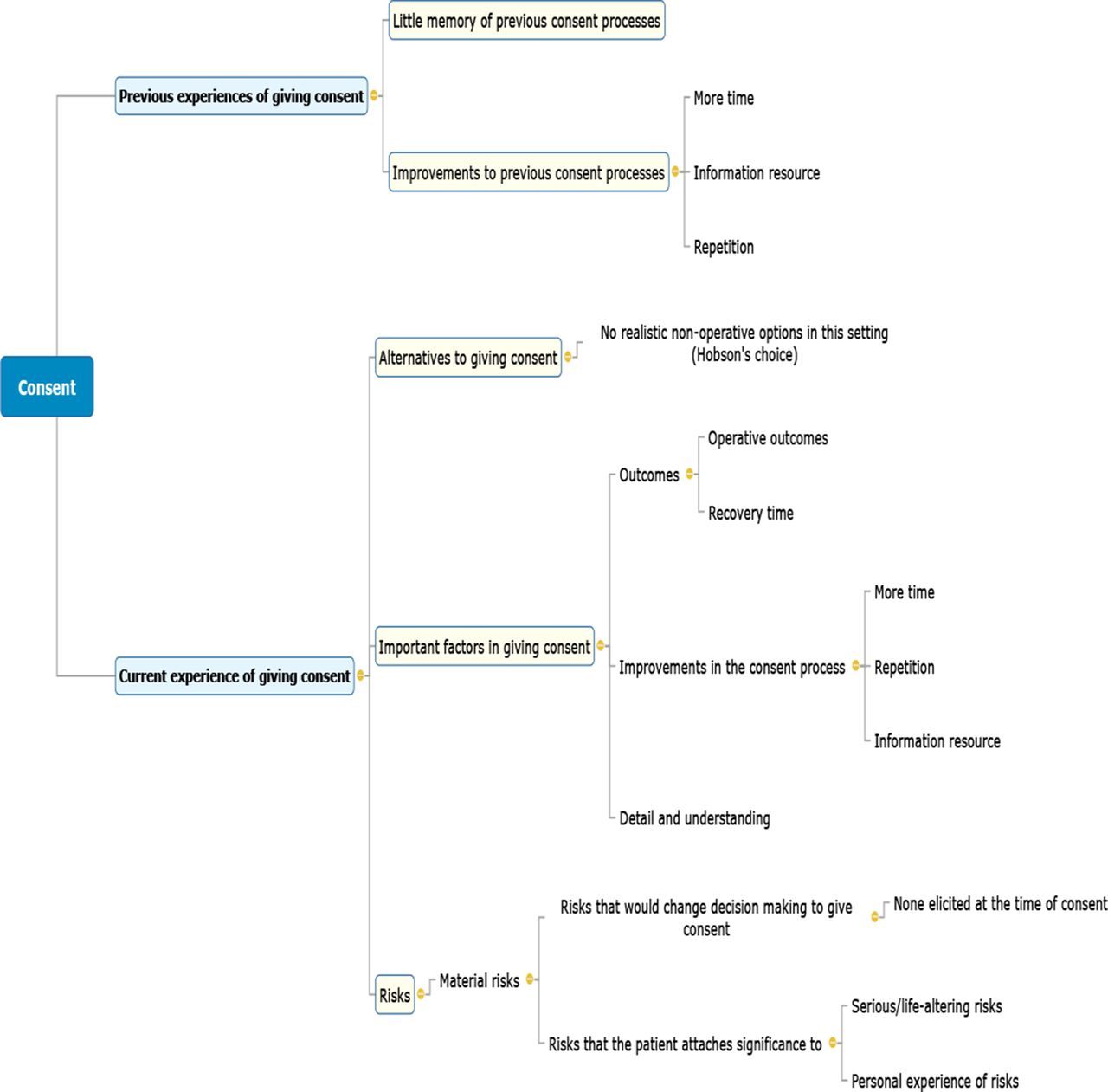
An exploratory thematic analysis was employed based on the six-phase approach outlined by Braun and Clarke.33 We chose thematic analysis because of the nature of the dialogue and its flexibility, comparative to other techniques, that is, discourse analysis. Data familiarisation was conducted by the first author and involved conducting, recording, fully transcribing, reading and re-reading the interviews. Data collection and analyses were conducted simultaneously. The patients did not review transcripts. A realist method was employed, “which reports experiences, meanings and the reality of participants”.33 The research question was to assess for material risks that the patient attaches significance to. We did not examine the ways in which such experiences may or may not be the result of discourses operating within the participant’s individual context or the effects of a range of discourses operating within society.33 The data were coded using NVIVO V.12 software into open codes using direct quotes from the participants. These codes were then collated into themes, until saturation of themes was reached. A summarised overview of this process is provided in figure 2. Saturation was reached when data from the new interviews generated similar codes already within the existing categories. Codes were then collated into themes in relation to the questions being looked into. These themes were then reviewed, defined and named. A quarter of the data was encoded separately by a separate member of the research team. Any disagreements or additions in the coding were discussed until a compromise was reached.
{kind=link}
{kind=link}
Summarised overview of coding structure and themes.
Results
Overall, 21 (12 male) consecutive patients with a mean age of 60.6 (range 19–88 years) gave their consent and participated in this study. On being approached, no patients refused to participate in the study. The nature and number of patients show a broad range of orthopaedic acute surgical interventions (table 2).
The characteristics and number of patients within the patient sample
Material risks
Courts have struggled to define material risk. The patients were asked to define what in their opinion were ‘material risk’. However, in addition to this question/answers, there is a difference between a patient concern about a surgical procedure and concern to a degree that prevents them consenting to the procedure (patient concern).
From the qualitative analysis undertaken as defined above, we found that patients were unable to cite examples of a material risk in the context of their surgery. Interestingly, when specifically asked if any individual risk would modify their decision-making process around giving consent, none were identified. In a trauma setting, most patients felt that they had no non-operative options that would provide a reasonable outcome. Statements such as “it has to be done. I didn’t really have a choice” were present in the majority of interviews.
He [the consenting surgeon] said the consequences of what would happen if I didn’t do it [have the operation], so I was like “yeah”. (Patient 9—open reduction internal fixation ankle)
You just want it done, you can’t dwell on it, it just needs doing. (Patient 10—open reduction internal fixation ankle)
One patient referred to the operation as ‘Hobson’s Choice’, an old English saying describing an apparently free choice when there is no real alternative.34
I look on this as Hobson’s choice. I mean I’m probably more relaxed than a lot of people in my position right now because I know I’ve got to have it done. (Patient 11—left hip hemiarthroplasty)
Personal experience or serious risks
Although no patients identified a risk that would change their decision-making, some did identify risks that were particularly significant to them, these are more of patient concerns rather a patient-specific material risk. Thus, there was variation in terms of the specific risks identified as significant rather than a material risk within the group. Some risks felt to be most significant came from personal experiences, others came from serious life-changing/threatening risks.
With the infection it is because my wife went into hospital with cancer and unfortunately, she had a really successful operation, but she was in saint james’ [anonymised hospital] a number of weeks with infection and a number of weeks at home with home nursing and things like that. So obviously I’m going to focus on that in my mind too. (Patient 6—open reduction internal fixation acetabulum)
When they start going on about “you might not pull through,” and heart attacks, strokes, and things like that, that makes your mind start ticking. If they probably wouldn’t have said owt like that you’d be like “yeah, yeah just get on with it” but then you start to think “no, I might have a heart attack or a stroke,” … It’s the more serious things that go through my mind the whole time”.(Patient 5—open reduction internal fixation ankle)
Operative outcomes, non-operative options and recovery time
When asked about material risks, some (usually younger) patients were most concerned about their operative outcomes and speed of recovery in relation to granting consent rather than the risks attached. When asked if any of the risks would change their decision-making about proceeding with the operation, these patients described the operation itself and the postoperative period as the keys to their decision-making process.
They said it can either take 10–12 weeks or I can have an operation and it would be a lot quicker and for me I want to get back to work. (Patient 21—open reduction internal fixation clavicle)
I think I was more concerned at the technical aspect of the operation and what it entailed, and the recovery period, rather than the risks. (Patient 15—open pectoralis major tendon repair)
For the two patients who had tendon repairs (patient 14, distal biceps tendon repair, and patient 15, open pectoralis major tendon repair), both spoke about functional outcomes as significant. When asked about significant risks, one echoed the concern of other participants about the serious or life-threatening risks, but also mentioned that a suboptimal (visual or functional) outcome was also a significant risk to them. The other patient spoke of operative versus non-operative outcomes related to his decision-making to provide consent for surgery.
I suppose the ones that are more serious to your health - infection, bleeding, deformation, or not being able to fully recover or gain your full strength. (Patient 14—distal biceps tendon repair).
If he [consenting surgeon] said the operation would have been no different to not having it, it wouldn’t have been worth doing but he said I’d have limited arm strength, and I kind of need my arm to do stuff. (Patient 15—open pectoralis major tendon repair).
Important factors to the patient when signing a consent form
Detail and understanding
The majority of patients identified thoroughness in explanation and details of both the operative procedure and the recovery as important to them before signing consent. This view was echoed by several patients with words/phrases like ‘thorough’, ‘detail’, ‘no stone unturned’ and ‘I understand everything they are saying’ being present in many answers.
I wanted to understand the detail of what was planned, why that approach was planned, how it would work, what would be happening, what would happen afterwards in terms of rehabilitation period, and then the risks. (Patient 1—open reduction internal fixation left ankle)
Improvement to the consent process: more time
When asked about either what was good about giving consent or improvements to the process, the theme of time recurred in many interviews. Several patients commented that it would have been useful to have more time between being given the information and signing the form. These patients said that they struggled to retain the risks and benefits of the procedure otherwise:
It was quite a long list of things which was hard to keep up with. (Patient 17—open reduction internal fixation radius)
One patient specifically mentioned that an online information resource would have improved his experience.
It was all very quick really. They haven’t got much time, but I felt there was a great deal of time explaining about everything, but also I was trying to take everything in at the time so the actual process of the operation would have been better if there was a link to an email or a video information specifically about that, that I could go to afterwards would have been useful. (Patient 15—open pectoralis major tendon repair)
Several patients mentioned that repetition of going through the consent form as helpful.
I think it was good that they went through it multiple times because I’ve been to a few wards and every time I went to a new place they went through it again. That was good. (Patient 17—open reduction internal fixation radius)
Little memory of previous consent
In the group of patients who had given consent prior, most admitted to having little or no memory of the consent process or the risks involved. One patient even denied that she had given consent all together. Only one patient could give a description of the process which was vague.
I think I was very happy about everything [with a previous consent process]. I was quite a wee while ago so it’s hard to remember. (Patient 2—left total hip replacement)
I don’t quite remember, I had a colonoscopy and I’m sure they did some consent before that, but I don’t quite remember. (Patient 1—open reduction internal fixation left ankle)
Discussion
This is the first study to look at eliciting material risks in patients undergoing single trauma operations. Previous studies have considered the position following the surgical intervention.35 The courts have struggled to define material risk, and in our study, patients were unable to explain what they thought was a material risk. This is separate to the concept of patient concern, inevitable with any medical procedure, which may or may not stop a patient consenting to the surgical intervention. The factors are particular to the patient; however, defining what patient concern amount to a material risk is problematic.
The key finding of the study is that patients are unable to identify what constitutes a material risk after giving consent. This highlights the difficulties of applying the Montgomery ruling in a trauma surgery setting. “The crux in the Montgomery case was that the doctor herself argued that by telling Mrs Montgomery about the risk of shoulder dystocia associated with a normal vaginal delivery in a diabetic mother she anticipated that the patient would elect for delivery by caesarean section.”10 In other words, that the risk that was not disclosed would have changed her decision-making to give consent. The current expectation of the consenting trauma surgeon is to be able to elicit these material risks at the time of taking consent. This study showed in a small qualitative sample that shortly after the moment consent was taken that patients themselves could not identify these material risks and felt that there were no risks that would change their decision-making. This re-enforces the need in the acute setting for time to be invested in the consent process to ensure that patients are aware of the intervention’s risk. From the results of the analysis, the experiences of the patient’s friends and family are particularly relevant, thus direct question is appropriate as time may preclude a conversation that elicits this information voluntarily from the patient.
The consent process for trauma operations included in this study bears little resemblance in character to other consent processes that now fall under the Montgomery ruling, such as palliative chemotherapy for example. In a trauma setting, consent is obtained shortly after injury. There is still much debate about optimum timing of fixations after trauma, but for broken neck of femurs, most national guidelines in developed countries recommend early surgery.36 The consenting surgeon is unlikely to have a detailed knowledge of the patient or a pre-existing clinical relationship with them. The aim of all the operations included in this study was curative, and the disability that would be incurred through non-operative management would be high. This demonstrates a unique challenge to the trauma surgeon’s consent process in relation to the Montgomery ruling, with possible similar (but not identical) scenarios including acute abdominal surgery.
The inability of the patients in this study to define any risks that were significant enough to change their decision-making may be in relation to these factors.
The ‘Hobson’s choice’ described by patients points the authors to hypothesise that in fact that potential disability of non-operative management could be thought of as a material risk in and of itself. This aligns with the finding that patients focus on the technical aspect and functional outcomes of the operation rather than the risks inherent to it. These findings are of patients who have accepted the risk of their operation and are thinking forward to the operation itself as they feel they have no other alternatives. The patient focus on the results of the intervention rather than risks associated with achieving those results is consistent with other studies looking at surgical management of neoplasms.37
These findings have generalisability. Consent for trauma operations, as discussed above, with their curative intent and high non-operative morbidity, is a specific decision-making process. However, these findings could be relevant to other curative surgical procedures such as acute abdominal surgery or tumour removals, it is unlikely to applying to consenting to life-prolonging chemotherapy, diagnostic colonoscopy or an elective total hip replacement for example. The short time period between injury, consent and operation may also have an impact on decision-making and an extensive analytical processing of the risks and benefits of the patient’s potential options.38
The legal test of materiality laid out in Montgomery relates to “a reasonable person in the patient’s position … attach[ing] significance to the risk”.1 Patients in this study attached significance to serious or life-threatening risks, however, not to the point where it would change their decision-making to consent for the operation. No patients in this study who had had previous operations had suffered a serious adverse outcome from these. The authors speculate that if patients within our cohort had previously experience such a complication, that would have had an impact on their decision-making.
Some of the risks that patients in this study regarded as significant were based on past experiences of friends and family. Thus, we suggest that the surgeon asks about any previous experienced ‘complications’, as this may elicit material concerns.
Patients in this study valued having more time to think before signing the consent for and felt that going through the consent form multiple times and to align with the Department of Health guidance on consent that ‘the seeking and giving of consent is usually a process, rather than a one-off event’. For major interventions, it is good practice to seek the person’s consent to the proposed procedure well in advance, when there is time to respond to the person’s questions and provide adequate information.39 As outlined above, the trauma surgery setting differs greatly from many other types of medical and even surgical consent and presents challenges to implementing this. The National Institute for Health and Care Excellence guidelines for management of a neck of femur fracture, for example, recommend “perform surgery on the day of, or the day after, admission,”40 which in most cases would be prohibitive to applying the Department of Health’s guidance.
One of the interesting findings of this study is that most patients struggled to remember any details of previous consent processes. This finding of poor recollection and understanding has been repeatedly shown in studies and literature reviews.41–48 A finding that worsens with increasing age.48 There is conflicting evidence as to efficacy of44 and strategies to49–51 improve this. Good documentation of the consent process remains key to ensure transparency and legal protection for doctors and patients.39 52
Limitations
There are limitations to this study. First, the interviews were shorter than many qualitative studies, which may have led to a lack of detail in the data. One reason for this is that much of the interview topic guide was designed to elicit and elaborate on material risks that were relevant to the patient; however, given that patients could not identify many, this reduced the interview length compared with what was initially anticipated. Second, the interviews were preoperatively, which limits the time for in-depth interviews. A previous preoperative qualitative study used interviews as short as 15 min.53
The authors made a deliberate decision to conduct the study after consent was taken but before the operation was conducted for the methodological reasons explained above. One potential flaw of this however is that material risks at this time could be ‘unknown unknowns’, a concept used in other fields including risk management.54 In the case of this study, patients could be unaware of material risks until they occur to them later down the line. This does however show the challenges to the surgeon trying to second guess these. Potential future methodologies to look for these could involve following patients up postoperatively and conducting multiple interviews or looking through cases coming from the clinical negligence system.
Another limitation could be considered—the decision taken to interview patients having trauma operations with definitive treatment of injury in a single surgical procedure. This aimed to exclude polytrauma where multiple procedures and operations would be needed therefore making interviews about operative risks and benefits indistinct. However, a potential consequence of this is that the included operations have lower risks and the results of this study may reflect this. Risk is a spectrum and is described and perceived differently by different individuals. An important question that this study was not developed to address was looking at major risks that would have had the patients declining surgery as the level of risk is lower for relatively minor procedures included in this study.
Conclusions
This work establishes that in trauma surgery, the patients immediately following the surgical consent process are unable to crystallise what material risk is, which confirms the hypothesis of the study. Montgomery1 states, “that a reasonable person in the patient’s position would be likely to attach significance to the risk”. There is a contradiction between the understanding and/or ability to vocalised and the expectation imposed by Montgomery. This is the first study to show this state of patient knowledge and expression, which is critical in a meaningful application of the Montgomery principle.
This study provides early data about the challenges of applying the Montgomery ruling to a trauma surgeon’s practice as patients could identify no material risks when giving consent. This does not alleviate the clinician in advising the patients of what is their view are the martial risks during the consent process. Patients in this study did attribute significance to past experiences of friends and family, thus, prompting us to suggest that the surgeon asks about these experiences. Patients’ functional recovery was an important factor but did not prevent them undergoing surgery.
Further work is needed to explore this issue in order to improve this apparent intellectual mismatch, a divergence between patients and clinicians as it has also been reported in other medical disciplines, such as in percutaneous coronary interventions.31
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AH and JW are joint first authors.
Contributors Conceptualisation: AH, PVG. Methodology: JW, NQ, AH. Formal analysis: JW, NQ, AH. Investigation: NQ, AH. Writing, original draft preparation: JW, AH. Writing, review and editing: JW, NQ, AH, PVG. Supervision: AH, PVG. All authors have read and agreed to the published version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The protocol of the study conformed to the Declaration of Helsinki. The HRA and Health and Care Research Wales granted ethical approval (REC reference: 19/LO/0197).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. The data has been de-identified and stored on a University drive.