Article Text

Abstract
Aims To determine the potential impact fraction of alcohol and tobacco consumption, high body mass index and low physical activity on colorectal cancer burden in Colombia for the period 2016–2050.
Methods Based on age-specific and sex-specific data on colorectal cancer incidence, data from population-based surveys for the exposure data and population projections, the macrosimulation model Prevent V.3.01 was used to model expected colorectal cancer incidence for the period 2016–2050. Baseline models were those where exposure levels were not subject to change because of interventions. Two intervention scenarios were specified: one with elimination of exposure to the risk factor as of 2017 and a second one where over a 10-year period the current prevalence data gradually declined until they reach 90% of the 2016 levels.
Results Under the reference scenarios, a total number of 274 637 colorectal cancers would be expected to occur in the period 2016–2050. Under the scenario of 10% gradual decline in the prevalence of alcohol and tobacco consumption, physical inactivity and high body mass index, a total of 618, 488, 2954 and 2086 new cases, respectively, would be avoided. Under scenarios of elimination, these numbers of avoided cases would be 6908 (elimination alcohol), 6104 (elimination tobacco), 16 637 (optimizing physical inactivity) and 25 089 (all on ideal weight).
Conclusions In order to reduce the burden of colorectal cancer, it is important to take measures to halt the current trends of increasing sedentary behaviour and overweight in the Colombian population. Proportionally, alcohol and tobacco consumption are less important population risk factors for colorectal cancer.
- gastrointestinal tumours
- public health
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Use of macrosimulation modelling to quantify the relative effects of reduction to behavioural risk factors for colorectal cancer on the incidence in the population.
Local age-specific exposure data for the Colombian population were used as input for the modelling.
Risk estimates from published meta-analyses were used as input for the modelling.
Unfortunately, demographic projections may be influenced heavily by the ending of the conflict, influx of Venezuelan migrants, which may affect absolute numbers differently than modelled with available projections.
Introduction
In many low-income and middle income countries (LMIC), populations are ageing and in transition to an ever-increasing Western diet which is characterised by diets relatively rich in meat, poor in fruits and vegetables and containing high amounts of processed foods and animal-based proteins, fats (particularly saturated) and cholesterol, refined carbohydrates and sugars, while low in dietary fibre and polyunsaturated fats.1 Additionally, the transition to a more western lifestyle usually implicates increased consumption of alcoholic beverages, smoking and reduction of hours of physical activity (PA) in comparison with the more traditional behavioural patterns of LMIC. As a consequence, the more traditional cancer patterns in LMIC are slowly changing from being predominantly infection-related cancers (cervix, stomach, liver), to the ‘western-style’ cancer patterns, with relatively high incidence rates of breast, lung, prostate and colorectal cancers.2
Colorectal cancer has ranked the fourth most common cancer in age-standardised incidence rates (ASIR, all expressed per 100 000 person-years) and the third most common cancer cause of death worldwide, and ranks fifth in upper middle income countries.3 Highest ASIRs are observed in Oceania (~37), followed by Northern and Southern Europe (ASIR~32) and North America (ASIR~26).
In South America, rates in Barbados and Uruguay (ASIR>35) outweigh the incidence of Canada (ASIR~32), but most countries are in the range of ASIR 11–17 with increasing tendencies.2 In Colombia, most recent population-based cancer registry (PBCR) data show ASIR between 8.4 and 16.2 with increases of 1.9% annually,4–8 placing it in the middle range of ASIR in South America, a bit higher than Peru and Ecuador, similar to Chile and substantially lower than Argentina and Uruguay.
Colorectal cancer risk is determined by a range of risk factors, some genetic in nature or resulting from medical conditions, others environmentally determined and therefore in principle avoidable. Known risk factors include: family history of colorectal cancer including certain mutations, inflammatory bowel disease, diabetes, overweight and obesity, alcohol consumption, consumption of processed meat, low vegetable and fruit intake, and tobacco smoking.4
Public health strategies that focus on reducing exposure to risk factors for chronic diseases, can benefit from comparing the potential impact on disease of distinct population interventions. The International Agency for Research on Cancer (IARC) has classified the evidence as ‘sufficient’ for the causal association between consumption of alcoholic beverages, tobacco smoking, X-radiation, gamma-radiation and consumption of processed meat and the risk of cancer of the colon and rectum (IARC group 1), exposure to red meat was classified as probably carcinogenic to humans (IARC group 2A).9 10 All of these are are amenable to modification, but modification of PA, diet, smoking and alcohol consumption requires considerable efforts. Effective modifications should reduce the burden of multiple chronic conditions. To prioritise such preventive strategies in terms of cancer benefits, it is important to quantify the theoretical impacts of changes on site-specific cancer incidence at the population level. Prevalence of these risk factors for the Colombian population is available through several surveys with national representation, and estimates of sex-specific and age-specific national colorectal cancer incidence are available.
Colombia is a country in a nutritional and dietary transition and has some distinct dietary patterns, which are changing from a traditional one—which protects against excess weight—to one that is characterised by a high protein and fibre consumption and has been observed to be associated positively with excess weight.11 12 In Colombia, alcohol is not typically consumed with meals but rather done weekly or biweekly and at toxic levels.13 14 Excess weight increased rapidly between 2005 and 2010.15
The objective of this study was to model the potential, and theoretical impact of interventions resulting in lower prevalence of overweight, obesity, tobacco and alcohol consumption, and sufficient levels of PA on the incidence of colorectal cancer for the Colombian population.
Methods
The analyses were based on a macrosimulation model, Prevent V.3.01, previously used in European studies of estimating population attributable risks and attributable fractions16–18 and for calculating the population-attributable risk of red and processed meat consumption for colorectal cancer in Colombia.19 In short, this model uses the known formula for population attributable risks based on prevalence of risk factors, relative risks (RRs) of those risk factors and population-based incidence data for the disease under study, as well as population projections as provided by bureaus of demographics and statistics. More details of the model are provided elsewhere.18 In the following section, we will briefly summarise which specific input data for Prevent were used in this study.
Baseline prevalence and interventions and risk functions
In table 1, we resume the international or national recommendations used for this project in terms of recommended levels for alcohol consumption, PA and body mass index (BMI) in relation to cancer risk and the way we operationalised these recommendations for this work, with the respective literature to support these recommendations. Prevalence of the risk factors were derived from population survey data and are detailed in the table 2.20–22 In summary, any alcohol consumption during past month (yes vs no) prevalence was between 29% and 62% in men, and between 11% and 49% for females, differing widely between age groups. Compliance with PA guidelines (At least 150 min of moderate PA yes/no) was low and better among men(between 52% and 34% of men complied) than women (20%–23% complied). Of note, younger men complied more often, compliance among women was more stable among age groups. Current cigarette use (yes/no) varied between 1.6% and 12.7% among men aged 10 years and older, and between 0.7% and 7.1% among women in this age group. For BMI in particular, individual-level data of the surveys23 24 were used to describe the distribution of BMI by age and sex group and summarised using mean and standard deviations (see online supplemental figure 1 for the density curves for BMI by sex). Excess weight increased rapidly between 2005 and 2010—particularly among older and urban populations,15 where 78% of the population is concentrated (see online supplemental table 1). The baseline scenario models the 2016 prevalence levels of the risk factors under study to remain stable, with the exception of BMI where past trends towards increasing prevalence were projected into the future. Baseline prevalence modelled was that of 2016 and onward according to these projections.
Supplemental material
Supplemental material
Summary of the reference values and relative risks (RRs) used in the macrosimulation models
Baseline prevalence and prevalence in 2050 under scenario of 10% reduction (ideal scenario would result in exposure of optimal levels hence zero risk exposure)
The risk functions used as input for the models were selected based on a non-systematic literature review. Papers that described associations between the risk factors under study and colorectal cancer were evaluated if they used the same or very similar exposure categories as those available from the population surveys available in Colombia. Two researchers evaluated these studies, scoring their quality on forms containing AMSTAR items for meta-analyses. The final decision on papers to include depended on this score on quality criteria and in case of equal or very similar quality scores, adding additional weight depending on sample size and if Colombian or Latin American populations were included. Finally, we included RR estimates from four meta-analyses.25–27 The risk functions for BMI were modelled based on the results of a meta-analysis with 70 000 events28 and fitting a regression line to connect the RR estimates and obtain the risk function presented in table 1.
Lat and lag times
For alcohol and consumption and PA an LAT time (time of change in prevalence without noticeable change in RR) of 2 years and an LAG time (time since end of LAT until full effect in terms of RR of exposure) of 10 years were modelled. For BMI corresponding values were 3 and 20 years and for tobacco 5 and 10 years.
Age-specific and sex-specific incidence rates and population projections
We used national age-specific and sex-specific estimates of colorectal cancer incidence for Colombia, which were based on extrapolations of data from four high-quality population-based cancer registries (of Cali, Bucaramanga metropolitan area, Manizales and Pasto, all published their data in editions X and XI of Cancer Incidence in Five Continents) and mortality data on departmental level, the age-standardised rate used in the input was 12.1 (males) and 12.4 (females), slightly different from the report because of the different age categories available but based on the same rates, which were available for age groups 15–45, 45–55, 55–65, 65+.29 30 The population distribution from 2016 was taken from the Colombian National Statistics Agency (Departamento Administrativo Nacional de Estadística (DANE)), whereas the demographic projects used in this project were those calculated by the Comisión Económica para América Latina y el Caribe (CEPAL) for Colombia up to 2050.31 32
Scenarios modelled
Similar to previous models applied on European data, we made a reference model for each of the risk factors under study, where the prevalence to the risk factor remained unchanged and two alternative scenarios; (A) an ‘ideal’ but not very realistic model where the prevalence of exposure to the risk factors was completely eliminated from the population (no alcohol or tobacco consumption, optimum PA or optimal BMI) and (B) a model where the prevalence to the four risk factors was reduced gradually during 10 years as of the year 2017, until reaching a 10% reduction compared with the original levels of exposure. The ideal model, where exposure is eliminated from the population, serves to obtain a population-attributable risk estimate as it provides incidence projected under a scenario of no exposure. Scenario b would be the results of a successful but less extreme intervention, acknowledging that in order to obtain a 10% reduction of exposure, drastic measures should already be taken. This range between 10% and 100% reduction illustrates the range of effects of substantial interventions. In the modelling, we gradually adjusted the prevalence of risk factors in an age-specific and sex-specific manner, reaching the reduction 10 years after the initiation of the model; we calculated the changes in projected incidence of the disease as a result of those changes in prevalence, assuming that the projections of demographic developments would remain unaffected by the changes in risk factor prevalence.
Patient and public involvement
In this modelling study, no patients or public were involved.
Results
In age groups between 15 and 50 years of age, around 50% of all men had consumed alcohol in the past month, versus a third or less of women. The proportion not complying with PA norms was high in all age groups, but substantially less women complied than men. Tobacco consumption was 19% or lower for all age groups, and more or less similar between sexes. The modelled distribution of BMI in the population is provided in online supplemental figure 1 and its values are provided in table 2. In general, the prevalence of exposure of the risk factors under study are higher among women. Age-specific and sex-specific prevalences of the risk factors under study are given in table 2. With the exception of alcohol consumption, risk factor prevalence was similar (tobacco) or higher among women compared with men.
Table 3 shows the decrease of projected colorectal cancer incidence under the scenarios of elimination and 10% reduction of exposure to the risk factors, for the four risk factors under study. Under the reference scenario (without interventions to change risk factor prevalence), a total of around 127 500 male and 147 000 female colorectal cancer cases would be expected to occur between 2016 and 2050. In the reference scenario of elimination of exposure to risk factors, the number of newly diagnosed colorectal cancer cases is expected to reduce between 3.1% (elimination of tobacco consumption) and 13% (optimum PA levels) among men, and between 3.7% (elimination of tobacco consumption) and 16.4% (optimum PA levels) for women. Should the exposure to risk factors be gradually reduced over a 10-year period up to reaching levels 10% lower than under the baseline scenario, then these proportions are 0.3% (tobacco consumption) to 1.2% (PA) for males and 0.1% (for reducing alcohol and tobacco consumption equally) and 0.9% (PA). In terms of absolute annual numbers by the year 2050, between 26 and 149 cases annually could be avoided by reducing the exposure by 10% (between 261 and 1463 for complete elimination).
Number of expected colorectal cancers in Colombia during the whole period 2016–2050 and for the year 2050 only, with or without interventions to reduce exposure to alcohol consumption, low physical activity levels, tobacco consumption and high body mass index (BMI)
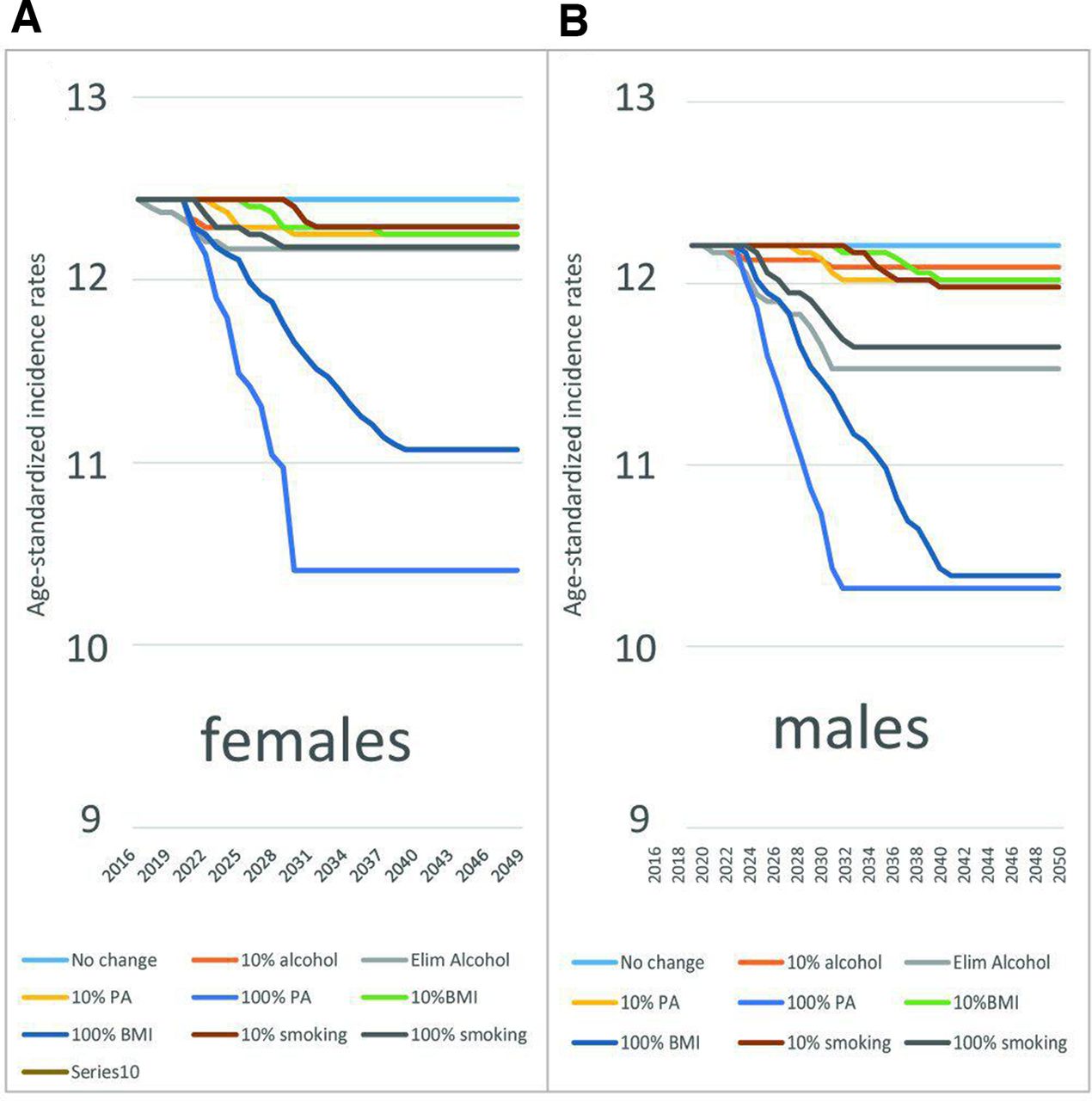
These changes take place gradually over time. Figure 1 shows these changes over time in terms of age-standardised colorectal cancer incidence rates for the period 2016–2050 under the reference and intervention scenarios. The results clearly show the relative importance of PA and BMI for the risk of colorectal cancer: under the scenario of elimination of these behavioural risk factors, 10%–13% of cases could be avoided in men, and 8%–10% in women—corresponding to differences in ASIR of 2–3 per 100 000. Elimination of smoking among men has only a slightly larger effect compared with reducing the exposure of low PA levels or high BMI among men by 10% (figure 1B). Among women, reductions of 10% in the exposure levels of smoking, high BMI and low PA have more or less similar effects in terms of incidence rates, alcohol is of less importance (figure 1A).

{kind=link}
Potential effect of reducing the exposure to the four risk factors in the expected rates of colorectal cancer incidence, period 2016–2050 under the reference and intervention scenarios. (A) Females, (B) Males. BMI, body mass index; PA, physical activity.
Discussion
The results of this study clearly illustrate the relative importance of four modifiable risk factors for colorectal cancer: alcohol and tobacco consumption, physical inactivity and high body mass index—showing that interventions aimed at increasing PA or decreasing BMI will have the largest impacts—similar in size to impacts to reduce consumption of red meat, and slightly less than a hypothetical elimination of processed meats.19 It is important to realise that results of macrosimulation modelling as performed in this study will never be a precise prediction, but rather allows for comparison of different scenarios and provides an idea of the magnitude of potential effects. Comparative estimates of the relative impact of reducing the distinct risk factors can help decision-makers in prioritising certain interventions over others. Of course, not only their impact on colorectal cancer is important, a number of other factors come into play such as their impact on other cancers and other chronic diseases, the relative difficulty of decreasing exposure in the population and economic factors and environmental influences.
Whereas the importance and causality of each of the included risk factors for colorectal cancer control is generally recognised, there is a lack of action in actually reducing exposure to these risk factors. For example, only three of ten Colombian children reaches recommended PA levels.33 Some interesting initiatives exist though and the weekly closure of main roads to cars to provide an opportunity for PA is an important example.34 35
This modelling exercise, as any modelling study, is as valid as its input data and assumptions. The independence assumptions on which Prevent is based18 implies limitations: we could not model all risk factors simultaneously as they probably have some synergistic effects; for example BMI is partially influenced by tobacco and alcohol consumption combined with PA levels. However, comparing the scenarios of each risk factor independently is also of interest as most population-based interventions are aimed at individual lifestyle related risk factors. These comparisons show independent effects of each and may help prioritising.
The baseline scenario modelled the 2016 prevalence levels of the risk factors under study to remain stable, with the exception of BMI, where past trends towards increasing prevalence were projected into the future. In reality however, there are indications that alcohol and overweight levels in Colombia are increasing and PA levels are reducing.13–15 36 In real life, every population intervention will have different effects depending in the characteristics of the particular population in which it is implemented. In Colombia, considering the limited information on time trends in the risk factors compared with the 2016 situation, the real effects of interventions to reduce population exposure to these risk factors is probably even greater than modelled in this study. The strength of this study is that it is based on data from mostly nationwide representative surveys measuring exposure to the factors under study. Ideally, one would have studied exposure such as PA and alcohol consumption in more detail than was done in this study—for example by type or number of minutes of physical exercise daily and by frequency of consumption and type of alcoholic beverage. However, data to such levels of detail became less reliable in the surveys with many missing data or data being collected in units that were not comparable to the RRs observed in the literature. As any modelling exercise is a simplification of reality, we decided to use the most reliable and reproducible exposure data. The mean and SD of the BMI and PA data were calculated from the original data by age and sex group, providing a very high level of detail of exposure in the population. The continuous nature of the BMI data allow to calculate effects of rather modest changes in BMI (not necessarily all persons with overweight moving to within the ‘normal weight’ categories) on population risk of colon cancer.
An important factor in the number of future cases expected lies in demographic developments of the country. Our demographic projections were based on those provided by CEPAL.32 However, considering the recent peace process, social and economic instability, and many other potential events in Colombia in the present or near future may strongly influence demographic tendencies which could not be taken into account in this study.
The LAT and LAG times used in this study were defined by the authors, because of a complete lack of information on these variables. The values used were equal or similar to those used in previous predictions16 18 19—they may be incorrect, however, the estimates for 2050 would be certainly after the LAT and LAG times combined and should not be influenced by the values used.
The risk estimates used came from meta-analyses, where possible those identified closest to the Colombian risk profile. Within Colombia, no good quality RR estimates were available. Some small studies, however, seem to indicate similar RRs as those presented in the meta-analyses. The RRs and risk functions modelled all come with their own levels of imprecision and potential biases derived from the study population and study design used. However, we believe that for the modelling exercise, aiming to show comparative effects of interventions rather than aiming to provide precise predictions of future cancer incidence, the input data were of sufficient quality. We used data from large Colombian population-based surveys with detailed and careful sampling procedures and adjustments taken into account into the survey designs. However, there is always a level of imprecision in measurement of exposure, and details in subpopulations (regional differences, behaviour in certain ethnic groups) were not taken into account, with the exception of age in our models.
The modelled effects of a 10% reduction in population-exposure to risk factors are notorious, yet a reduction of 10% may seem only modest. However, in practice, reducing exposure to unhealthy lifestyle habits on a population level is extremely difficult, and even obtaining small improvements over a 10-year period would involve major efforts by a multitude of actors.
Colorectal cancer incidence can be reduced by reducing exposure to its risk factors, but also by implementing an organised colorectal cancer screening programme. Currently, the Colombian health system facilitates opportunistic screening by faecal occult blood tests but the participation of the population in this ‘screening’ so far is very limited.37 The authorities should optimise participation of the population in this opportunistic screening opportunity and work on reducing exposure to risk factors, which could reduce not only colorectal cancer risk but also risks for other cancers and other diseases such as diabetes and cardiovascular disease. Further improvements in timely access to diagnostic and curative care should in addition be implemented to reduce colorectal cancer mortality.37 The situation for red meat consumption and colorectal cancer risk is complicated in a country where malnutrition is still a big issue. The Ministry of Health considers that the red meat consumption of the population does not reach levels declared as ‘risky’ for colorectal cancer and therefore is not making any recommendations—the consumption of meat is very unequally distributed, similar to the socioeconomic inequities in the country.24 38
In summary, the results of this study show that interventions aimed to reduce exposure to alcohol, but in a larger extent to high BMI and low PA, may help to avoid a substantial number of colorectal cancer cases and hopefully will be able to reverse the currently increasing trends. Effects of reductions to tobacco consumption are relatively small for colorectal cancer, as the RRs associated with tobacco consumption for colorectal cancer are limited. Lifestyle interventions to reduce exposure to these risk factors will have a positive impact on non-transmittable chronic disease control in general, yet for the moment few population-wide initiatives are developed in this field—an opportunity for those in charge.
Acknowledgments
We are grateful for the kind contribution by the late Dr. Jan J Barendregt from the Department of Public Health at Erasmus MC in the Netherlands, director and owner of the website EpiGear, who developed the PREVENT software and provided it free of charge for use in this project. Also grateful to the Instituto Colombiano de Bienestar Familiar (ICBF), who provided us with the databases of individual BMI values reported by the ENSIN 2005 and 2010 questionnaires. And ‘muchas gracias’ to Violeta Avendaño for providing the supplementary figures of the BMI distributions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @EstherdeVries16
Contributors The authors contributed in the following activities. EdV: Conception and design of the work, data acquisition and analyses, interpretation of results, writing and revision of manuscript. MZT: project management, data acquisition and analyses, interpretation of results, writing and revision of manuscript. MPR: data acquisition, interpretation of results, writing and critical revision of manuscript. GD: interpretation of results and critical revision of first manuscript. OFH: data acquisition, interpretation of results and critical revision of first manuscript.
Funding This study was funded by the Colombian Instituto Nacional de Cancerología E.S.E. (INC) with proper resources in the period 2016-2019 [budgettary code 41030110020 (2016), C190103001-15 (2017-2018). The same institute financed the personnel costs between 2016-2019 without further subsidies. The project as confinanced and coexecuted by the Pontificia Universidad Javeriana (Convenio PPTA7602, project medical ethics code 2016/157), the Universidad Industrial de Santander and the Universidad El Bosque, which provided investigator time and resources.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study. The data used as input in the modeling exercise are all publicly available through the references cited in the manuscript. PREVENT software used to be available on request from the website of EPIGEAR, but with the unfortunate passing away of the owner, this is not longer downloadable.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.