Article Text

Abstract
Objectives Preoperative anaemia is associated with increased risks of postoperative complications, blood transfusion and mortality. This meta-analysis aims to review the best available evidence on the clinical effectiveness of preoperative iron in anaemic patients undergoing elective total hip (THR) or total knee replacement (TKR).
Design Electronic databases and handsearching were used to identify randomised and non-randomised studies of interventions (NRSI) reporting perioperative blood transfusion rates for anaemic participants receiving iron before elective THR or TKR. Searches of CENTRAL, MEDLINE, Embase, PubMed and other databases were conducted on 17 April 2019 and updated on 15 July 2020. Two investigators independently reviewed studies for eligibility and evaluated risk of bias using the Cochrane risk of bias tool for randomised controlled trials (RCTs) and a modified Newcastle-Ottawa scale for NRSIs. Data extraction was performed by ABS and checked by AB. Meta-analysis used the Mantel-Haenszel method and random-effects models.
Results 807 records were identified: 12 studies met the inclusion criteria, of which 10 were eligible for meta-analyses (one RCT and nine NRSIs). Five of the NRSIs were of high-quality while there were some concerns of bias in the RCT. Meta-analysis of 10 studies (n=2178 participants) showed a 39% reduction in risk of receiving a perioperative blood transfusion with iron compared with no iron (risk ratio 0.61, 95% CI 0.50 to 0.73, p<0.001, I2=0%). There was a significant reduction in the number of red blood cell units transfused with iron compared with no iron (mean difference −0.37units, 95% CI −0.47 to -0.27, p<0.001, I2=40%); six studies (n=1496). Length of stay was significantly reduced with iron, by an average of 2.08 days (95% CI −2.64 to −1.51, p<0.001, I2=40%); five studies (n=1140).
Conclusions Preoperative iron in anaemic, elective THR or TKR patients, significantly reduces the number of patients and number of units transfused and length of stay. However, high-quality, randomised trials are lacking.
PROSPERO registration number CRD42019129035.
- anaemia
- hip
- knee
- orthopaedic & trauma surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This review has a pragmatic approach to inclusion criteria and is focused on one particular type of elective surgery, which is considered as one of the most appropriate fields for preoperative anaemia optimisation.
Comprehensive database and handsearching techniques have been employed to identify the best available evidence on this topic, and rigorous sensitivity analyses of results have been undertaken.
The results of this review are limited by the quality of the included studies. A lack of well-conducted randomised controlled trials means insufficient evidence is available to reliably inform future clinical practice or guideline development.
The quality of reporting in the included studies, particularly around the underlying cause of anaemia, other coexisting patient blood management strategies and patient adherence also limit the results of this review.
Introduction
Over 175 000 primary, elective total hip (THR) or total knee replacements (TKR) were performed in the UK in 2018–2019.1 Up to one in three of those patients would be expected to have preoperative anaemia, the majority of which is caused by absolute or functional iron deficiency in this population.2–6 Preoperative anaemia is an independent risk factor for increased perioperative complications, mortality, allogenic red blood cell (RBC) transfusion and longer length of hospital stay (LoS).7 RBC transfusion itself is also independently associated with poorer postoperative outcomes and longer LoS.7 Elective orthopaedic surgery is described as one of the most appropriate fields for implementation of preoperative anaemia optimisation.8 Erythropoietin (EPO) is one option for optimising preoperative anaemia; however, there are concerns that routine use is not cost effective.9 10 The National Institute for Health and Care Excellence in the UK and multiple international guidelines recommend iron treatment(s) be used to optimise anaemia caused by iron deficiency, in the preoperative period.10–13 However, a recent report from the Royal College of Anaesthetists found 70% of anaemic patients received no treatment for anaemia in the 3 months before surgery.14
There is mounting evidence that multimodal patient blood management (PBM) programmes can be effective at improving postoperative outcomes and reducing perioperative blood transfusions and costs.15 16 A PBM programme typically consists of three ‘pillars’; (1) optimising red cell mass, (2) reducing blood loss and (3) harnessing and optimising physiological reserve of anaemia.17 While some elements of PBM have a strong evidence base in hip or knee replacement, such as the use of tranexamic acid (TXA)18 and reduced transfusion thresholds,19 the evidence for preoperative anaemia optimisation with iron is less robust.13 This coupled with organisational barriers and misconceptions around treatment options may be contributing to poor uptake.20 21
The question addressed by this review is, does preoperative iron improve postoperative blood transfusion rates and outcomes, in patients with preoperative anaemia undergoing primary, elective THR or TKR? Although the majority of preoperative anaemia in this population is likely to be due to iron deficiency, iron alone will not address preoperative anaemia for all patients and guidelines recommend the underlying cause of anaemia should be ascertained before starting treatment.2 3 10 13 In recognition that iron will not be appropriate for all patients and in an attempt to make the results more generalisable, we included studies using another intervention to treat preoperative anaemia, such as EPO, for up to 20% of participants. This figure is based on a multicentre cohort study showing approximately 85% of preoperative anaemia in elective surgical patients is due to iron deficiency (functional or absolute) or low iron stores, and may respond to iron.2
Methods
CENTRAL, MEDLINE, Embase, PubMed, ISI Web of Science, Transfusion Library, ClinicalTrials.gov, ICTRP, ISRCTN and ProQuest databases were searched using the search strategies in online supplemental appendix 1A. An example of search terms used include (“iron” OR “iron compounds” OR “ferrous compounds” OR “ferric compounds”) AND (“anemia” OR “anemia, iron deficiency”) AND (“preoperative period” OR “preoperative care” OR perioperative period” OR “preoperative care”) AND (“orthopedics” OR “hip” OR “hip joint OR “hip prosthesis” OR “arthroplasty, replacement, hip” OR “knee” OR “knee joint” OR “knee prosthesis” OR “arthroplasty, replacement, knee”). Searches were performed on 17 April 2019 with no date or language restrictions applied and were updated on 15 July 2020.
Supplemental material
The reference lists of the most recent clinical guidelines for preoperative anaemia from Europe, Australia and the USA, existing systematic reviews on a similar topic and expert opinion pieces were scanned for additional studies. Abstracts from relevant conferences from January 2009 to April 2019 were hand searched, and field experts and relevant pharmaceutical companies were contacted to obtain any unpublished trials. Where trial protocols were found by the searches we also searched for any results papers. Forward and backward reference searching of the included studies was performed. Search results were collated in Covidence systematic reviews software (Veritas Health Innovation, Melbourne, Australia).
This review includes randomised controlled trials (RCTs) and non-randomised studies of interventions (NRSI) with a control group that report perioperative blood transfusion rates for adult, anaemic participants who received iron treatment (enteral or parenteral) before undergoing elective THR or TKR. Anaemia is traditionally defined as haemoglobin (Hb) values less than 130 g/L for males and 120 g/L for non-pregnant females.22 However, in recognition of views that a non-gender based cut-off of 130 g/L for males and females is more appropriate,12 we accepted any clear definition of anaemia by the study investigators. Eligible comparators were another form of iron treatment, placebo, no anaemia treatment or standard care.
The primary outcome was perioperative blood transfusion rate. Other outcomes of interest were quantity of blood transfused (units), change in Hb or ferritin concentration, morbidity including infection and other adverse events, mortality, LoS, critical care admission rate, readmission rate, compliance with iron and any validated quality of life (QoL) measure. Studies that include participants undergoing THR or TKR following trauma or where the intervention included autologous transfusion methods were excluded.
Following deduplication, two authors (ABS and AB) independently reviewed titles and abstracts to assess study eligibility against the predefined criteria. Full manuscripts of any potentially eligible records were obtained and screened using the same method. Multiple accounts of the same study were excluded. A record of excluded studies is provided in online supplemental appendix 1B.
One author (ABS) extracted data from each study using a prepiloted data extraction form. Data were checked by a second author (AB). Disagreements on inclusion of studies and data extractions were discussed and a consensus reached. Where information was unclear, attempts were made to contact study authors for further details. Where available as a subgroup, only data for participants receiving iron were extracted.
The two reviewers (ABS and AB) independently assessed the risk of bias and quality of studies using the Cochrane Risk of Bias (RoB2) tool for randomised studies and the Newcastle-Ottawa scale (NOS) for NRSIs.23 24 Again, disagreements were discussed, and a consensus reached. A modified version of the NOS, excluding fields of ‘demonstration that outcome of interest was not present at start of study’ and ‘was follow-up long enough’, was used as these were not applicable to this review. The maximum score using our modified NOS is 7 stars. To reduce variability in applying the NOS between authors, detailed criteria were developed specific to this review (see online supplemental appendix 1C).
Standard criteria for defining high-quality or low-quality studies using this modified NOS do not exist. For this review, studies scoring ≤4 stars or at high risk of bias on RoB2 were defined as being of low quality. This is based on a previous review which used a similarly modified NOS.25
We planned to perform meta-analysis of postoperative outcomes and where sufficient data were available, subgroup analyses comparing types of iron, types of surgery and the use of concurrent treatments. However, sufficient data were only available to perform subgroup analysis for different types of iron. To control for the one study that used EPO in two participants, it was excluded as part of the sensitivity analyses. In addition, we undertook an exploratory analysis of correlation between pre-iron Hb and type of iron treatment on the change in Hb concentration following iron. We have also conducted sensitivity analyses to assess the robustness of our results.
Meta-analysis was undertaken using Review Manager V.5.3 (The Cochrane Collaboration, Oxford, UK). The Mantel-Haenszel method was employed using risk ratios (RR). A random-effects model was used due to expected methodological heterogeneity among studies in relation to iron drug, dose and timing, definitions of anaemia and transfusion thresholds. Mean differences (MD) were calculated where appropriate depending on homogeneity of units of reporting (ie, RBC units). The I2 statistic was used to assess heterogeneity. In keeping with previous Cochrane reviews, moderate and substantial heterogeneity were defined as an I2 of more than 50% or 85%, respectively.19 26
Differences were seen in how studies reported data on the number of RBC units transfused. Some studies reported an average only for the subpopulation who received a transfusion and others an average for the entire cohort undergoing surgery. In studies reporting only for those who had a transfusion, it is known the rest of that cohort population, those not transfused, all received zero RBC units. In order to allow meaningful pooling of results, methods of combining means were used to convert these into averages for the entire cohort undergoing surgery (online supplemental appendix 1D).
This review includes studies with any clear definition of anaemia, this resulted in the inclusion of two studies in which participants have a presenting Hb level (130–140 g/L) that by traditional WHO definitions would be considered non-anaemic.27–30 It is also thought intravenous iron leads to a greater Hb increase than oral iron.30 Subgroup and meta-regression analyses were performed to investigate these associations further.
When pooling data on pre-iron and post-iron Hb concentrations, correlation is expected as these data are from the same participants. As such, a correlation coefficient (CC) is required to accurately calculate a MD and variance. As no published CC were identified, these were calculated for oral (0.56) and intravenous (0.70) iron from a local dataset, made available to reviewers.31 Comprehensive Meta-analysis (V.2, Biostat, USA) was used to calculate the MD, SD and SE for each study reporting pre-iron and post-iron Hb data and meta-regression was performed in Stata (V.15.1 StataCorp) using the ‘metareg’ command.32
In accordance with recommendations from the Cochrane Collaboration, as 10 studies were included in the meta-analysis of the primary outcome a funnel plot was generated and visually inspected to assess for publication bias.26 For all statistical tests a p<0.05 was considered statistically significant. Sensitivity analysis of the pooled results was performed excluding studies where the underlying cause of anaemia was not specifically reported as being iron deficiency; low-quality studies; those with any imputed data; those using a concurrent anaemia treatment (ie, EPO); and those with an average presenting Hb >130 g/L.
Where studies report outcomes separately for oral and IV iron, outcomes were analysed separately for the effects on Hb concentration, but the oral and intravenous groups data were combined for inclusion in meta-analysis on postoperative outcomes (online supplemental appendix 1E), using methods recommended in the Cochrane handbook.26
Patient and public involvement
There was no patient or public involvement in this meta-analysis.
Results
Literature search
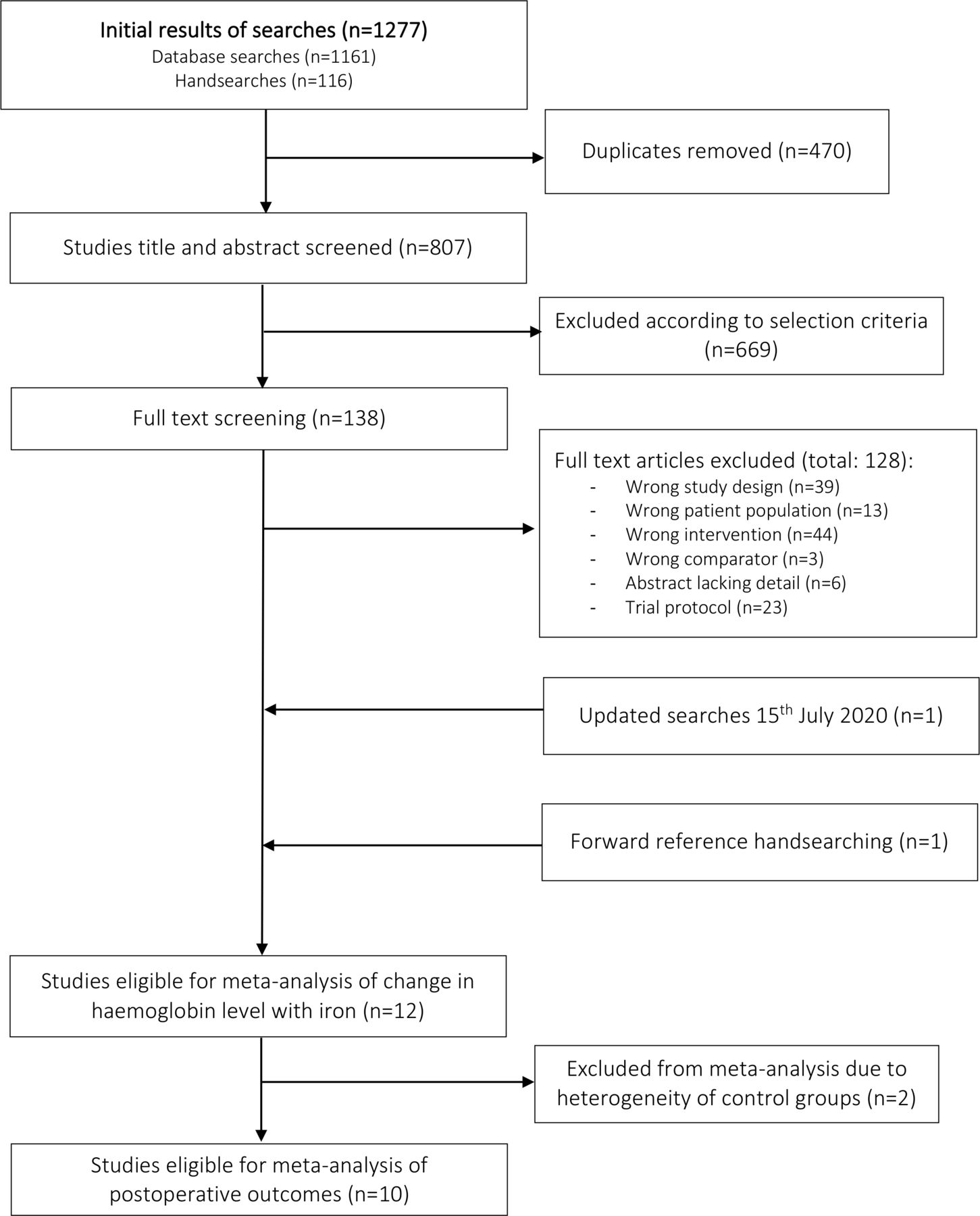
Following deduplication 807 records were identified from the search strategy (figure 1). Based on screening of titles and abstracts 138 records underwent full-text review. Of these, nine met the inclusion criteria. One additional study was identified by handsearching for the final publication related to a trial protocol found. This study was identified in a non-PubMed indexed peer-reviewed journal, which is why it was not identified by our database searches. Both authors agreed this study met the inclusion criteria for this review. Forward citation searches of the ten eligible studies identified one further study for inclusion, in the KoreaMed database. A search of this database identified no other relevant studies. Electronic database search updates in July 2020 identified 175 studies. Following deduplication and screening, one additional study was eligible for inclusion in this review.33

Flow chart of study selection.
A total of 12 identified studies were eligible for this review.28 29 31 33–41
Study characteristics and quality
The characteristics of the 12 included studies are given in tables 1–3 and figure 2. Three studies tested the effects of oral iron salts, two of oral sucrosomial iron, four of intravenous iron and three of a combined approach of oral and/or intravenous iron. The average timing of iron treatment before surgery ranged from 2 to 60 days. Intravenous iron was typically given in 1–2 sessions within 4 weeks of surgery, while oral iron was typically given for 4 weeks, a month or more before surgery. Comparators were no preoperative iron (standard care), oral iron or intravenous iron. Eight studies report routine use of restrictive transfusion triggers across all groups, two report using non-restrictive triggers40 41 and two did not report this.34 35 Four studies report the ‘routine use’ of TXA28 31 33 38; however, only one of these studies formally assess this.33 Three studies report that cell salvage was not routinely used.28 29 38 Two studies were excluded from the meta-analysis on postoperative outcomes due to heterogeneity in their control groups. Ten studies included an anaemic control group that received no iron, while in one study two types of IV iron were compared34 and another only included a non-anaemic control group.41

Quality assessment of the included randomised controlled trial. IV, intravenous.
Included study characteristics
Population characteristics and outcomes
Quality assessment of included non-randomised studies of interventions
Of the 10 studies included in the meta-analysis of postoperative outcomes, nine were comparative cohort studies and one a RCT. Nine were full peer-reviewed publications and one a conference abstract, which was later excluded in the sensitivity analysis due to poor quality.35 Two studies were in non-English language and required translation by a third (PS, French) and fourth (IHL, Korean) reviewer familiar with systematic review techniques and fluent in the relevant language. For these studies data extraction and quality assessment was performed by the translating reviewer under the guidance of ABS. Detailed guidance of the Newcastle-Ottawa scoring criteria used for this review can be found in table 4. Of the 10 studies, four were of low quality.33 35 39 40 Visual inspection of the funnel plot for the primary outcome, perioperative blood transfusion rate, (figure 3) suggests an asymmetrical appearance, with a possible absence of published, smaller studies that show no statistically significant effect. This suggests there may be publication bias towards the positive effects of iron, with the risk that the pooled estimate may be an overestimation of the true intervention effect; however, other explanations cannot be ruled out and the number of studies in the plot just meets the minimum required.26

Funnel plot for primary outcome, perioperative blood transfusion rate. RR, risk ratio.
Definitions used with the Newcastle-Ottawa scale to assess quality of non-randomised studies of interventions in this review
Risk of transfusion
Eight studies reported the number of participants receiving perioperative allogenic RBC transfusion with iron treatment compared with no iron treatment.29 31 33 35–37 39 40 This outcome was estimated from related data in a further two studies.28 38 In one of these studies the intervention includes iron±EPO, here subgroup data for participants receiving only iron has been extracted.38 This paper states that there was no significant difference in the transfusion rate between participants who received iron alone or iron and EPO, so we have estimated the number of participants transfused in the iron only subgroup based on the proportion reported (12%). In the other study only the number of RBC units transfused has been reported (n=7).28 In order to reduce the risk of inflating the effect size of iron, we have assumed these units have been given to the smallest plausible number of participants (n=1).
Ten studies (n=2178 participants) were pooled (figure 4). The transfusion rate in the iron groups combined was 15.1% (106/700) compared with 27.2% in the control group (402/1478). Treating anaemic participants with iron before THR or TKR significantly reduces the risk of receiving a perioperative blood transfusion by 39% (RR 0.61, 95% CI 0.50 to 0.73, p<0.0001). There was no evidence of heterogeneity (I2=0%), there were no significant subgroup differences (p=0.35).

Forest plot comparing number of anaemic participants transfused in those receiving preoperative iron to no iron. IV, intravenous.
Sensitivity analyses excluding studies where the underlying cause of anaemia was not reported as iron deficiency,33 35 37 low-quality studies,33 35 39 40 studies with any estimated values,28 38 studies using concurrent EPO,28 studies with a presenting Hb >130 g/L,28 29 or all of the above, had no discernible effect on the effect size estimate (see online supplemental appendix 1F).
Number of RBC units transfused
Five studies (n=1496 participants) report the number of RBC units transfused,29 31 36–38 three of these required conversion to population level statistics.31 36 37
There was an average reduction of 0.37 RBC units (95% CI −0.47 to −0.27, p<0.001) transfused per anaemic patient undergoing elective THR or TKR in the preoperative iron group compared with control (figure 5). Heterogeneity was low (I2=40%) and there were no significant subgroup differences (p=0.06).
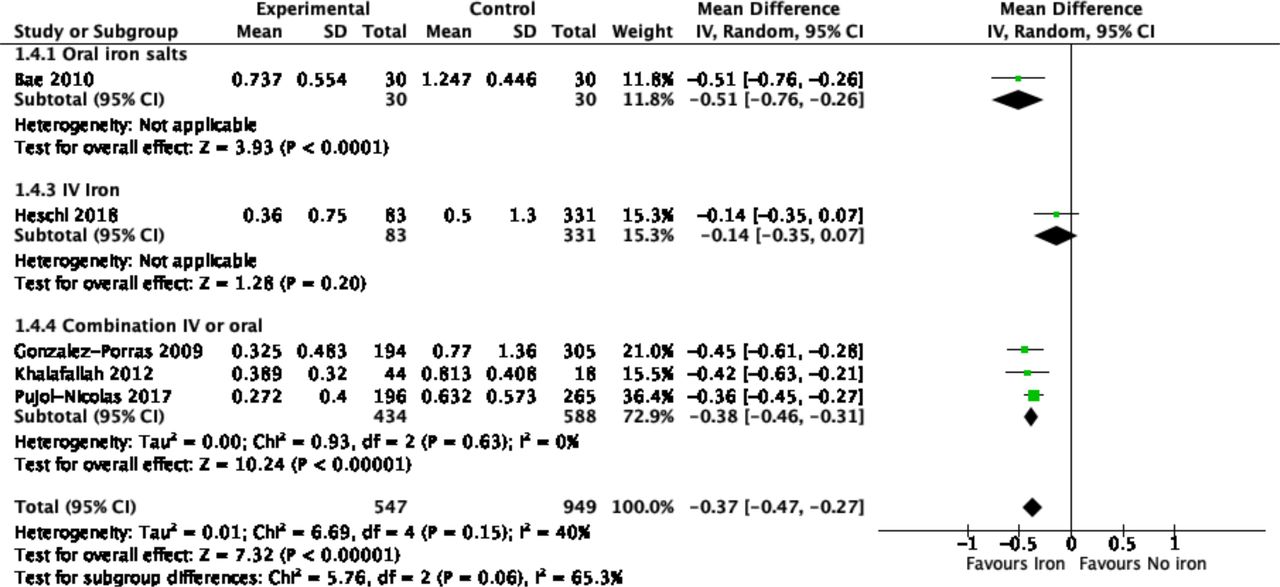
Forest plot of units of blood transfused with outcome standardised to units per patient undergoing surgery. IV, intravenous.
None of these studies were of low quality or used a concurrent treatment, all studies report the cause of anaemia as being iron deficiency. Sensitivity analyses excluding studies where the variance had been estimated,37 data required conversion to the mean,31 with a presenting Hb >130 g/L,29 or all of the above, had no discernible effect on the effect size estimate (online supplemental appendix 1).
Length of hospital stay
Five studies (n=1140 participants) report mean LoS but two do not report any measure of variance, or other statistics that would allow this to be calculated.28 37 In line with Cochrane recommendations the mean of the SDs from the three other studies was used for these studies.26
The combined mean LoS in the no iron group was 8.72 days (SD 4.97) and in the iron group was 6.12 days (SD 4.19). LoS was reduced by an average of 2.08 days in the preoperative iron group compared with no iron (95% CI −2.64 to −1.51, p<0.001) (figure 6). Low heterogeneity (I2=40%) and no significant subgroup differences were observed (p=0.09).

Forest plot comparing the length of stay of in anaemic participants receiving preoperative iron or no iron. IV, intravenous.
All of the studies report the cause of anaemia as iron deficiency. When studies of low quality,39 with an estimated SD,28 37 using a concurrent treatment,28 or with a presenting Hb >130 g/L28 were excluded a significant effect in favour of iron remains. When all exclusions are applied only two studies remain, reducing the power of pooled estimates.31 36 A beneficial effect of iron persists (MD −0.98 days), but the 95% CI is much wider (-2.02 to 0.05 days, p=0.06, I2=0%, online supplemental appendix 1F).
Change in Hb concentration
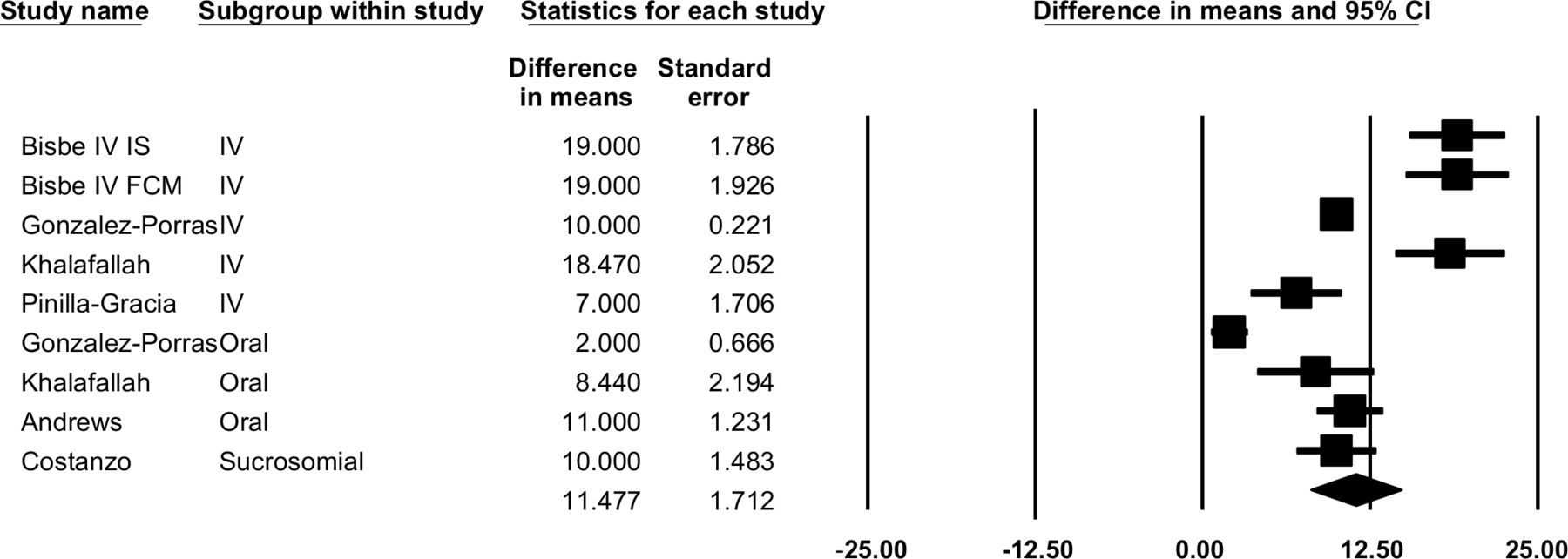
Six studies (n=325 participants) report average Hb concentrations pre- and post-iron treatment.29 33–36 41 Two studies combined oral or intravenous iron as the intervention,29 36 one used oral iron salts,41 one used intravenous iron only,33 one compared two intravenous iron formulations34 and one used sucrosomial iron.35 The duration of treatment, and hence time between Hb measurements, was reported in five29 33 35 36 41 of the six studies. The average time was 28 days. However, often this was not accurately reported, and where reported there was often a wide range of timings.
Iron was associated with a significant increase in mean Hb concentration (MD 11.48 g/L, 95% CI 8.12 to 14.83 g/L,figure 7) .

Forest plot of change in Hb pre-iron to post-iron accounting for correlation between result. FCM, Ferric Carboxymaltose; Hb, haemoglobin; IV, intravenous.
In an exploratory analysis, a higher presenting Hb was associated with less of a Hb increase following iron treatment (figure 8, slope of the regression line −0.30, 95% CI −0.59 to −0.19, p=0.04) and oral iron was associated with less of a Hb increase compared with intravenous iron (figure 9, slope of the regression line 7.50 g/L, 95% CI −2.24 to 17.24 g/L, p=0.11).

L'Abbe plot showing change in Hb from pre-iron to post-iron treatment by presenting Hb level. Each circle represents a group treated with one type of iron, some studies have two circles. Size relates to precision of estimate. Hb, haemoglobin.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
L'Abbe plot showing change in Hb by oral or intravenous iron (excludes sucrosomial iron as only one study used this and reported pre-iron and post-iron Hb data). Hb, haemoglobin; IV, intravenous.
Hb concentrations after surgery were rarely reported, and where reported significant heterogeneity in timing was seen, therefore pooling studies in a meta-analysis was considered inappropriate. One study reported no difference36 with iron while two studies showed beneficial effects of preoperative iron on postoperative Hb.28 37
Other outcomes
Three studies report some cost estimates, all favour iron. Savings estimates include $A400 000 per year (2012) for a 300 bed hospital with intravenous iron,36 €1763.25 (2019) per patient with sucrosomial iron28 and £162.46 (2017) per patient with a combined oral or intravenous iron approach.31
Other outcomes such as infection, medical complications and readmissions were rarely reported and, where they were, no differences were reported. Four studies (n=167 participants, 94 IV iron, 73 oral) report adverse events.33 34 36 41 Four participants (4%) in the intravenous and three participants (4%) in the oral iron groups report minor complications. One study reported a significantly reduced critical care admission rate favouring iron (control 4.9% vs intervention 0.5%, p=0.007).31 Another reports improved QoL outcomes with IV vs oral iron36 using a modified short-form 36 questionnaire, however, there were concerns acknowledged by the study authors around these data and confounders.
Discussion
Preoperative anaemia is common in patients undergoing elective THR or TKR and is associated with poorer postoperative outcomes and increased transfusion rates. This review has shown that the use of preoperative iron in anaemic participants is associated with a reduction in the number of participants requiring perioperative transfusion, the number of units transfused and LoS. The presenting Hb concentration and type of iron used appear to correlate with the degree of Hb increase, but insufficient data were available to examine correlation with postoperative outcomes.
However, the results should be interpreted with caution as only one of the included studies was an RCT at risk of bias. The analyses and meta-regression are, therefore, effectively observational and may exaggerate the true treatment effect. Higher quality evidence, such as a well conducted, adequately powered RCT is required to inform future clinical practice or policy change. A future RCT in this field could consider three treatment arms; no iron, oral iron and intravenous iron, and could include clinical, economic and QoL outcomes. Although, in the setting of existing guidelines, a no iron control group may prove difficult to implement and should be carefully considered.
Our results are in keeping with previous systematic reviews on preoperative anaemia optimisation in orthopaedic42–45 and other surgical populations.46–49 However, this is the first review to include NRSIs and focus solely on the use of preoperative iron in elective arthroplasty patients, as a means of patient optimisation before surgery. This group of patients have been described as one of the most appropriate for preoperative anaemia optimisation, due to the prevalence of iron deficiency anaemia and typical time available for anaemia optimisation on elective surgery pathways.8 Unlike other reviews, we have intentionally not included studies that include arthroplasty following trauma as the time available for preoperative optimisation with iron is minimal and this population is typically older, with more comorbidities and are more likely to encounter postoperative complications than elective arthroplasty patients.50
Our results are also similar to those seen in meta-analyses on other PBM interventions such as the use of restrictive transfusion triggers, which have been estimated to reduce the risk of blood transfusion by 43% across a range of clinical specialties,51 and TXA, which has been estimated to reduce the risk of blood transfusion in surgical patients by 38%.52 However, it should be noted the quality of evidence for reduced transfusion triggers and TXA is much stronger as their estimated effect sizes are based on 31 and 129 randomised trials, respectively.
Treatment options
National and international guidelines recommend that treatment for preoperative anaemia is directed by the underlying cause.10 12 For the majority of patients undergoing elective THR or TKR this is likely to be iron deficiency (functional of absolute) which would be expected to respond to iron.2 33 However, this will not always be the cause. Algorithms for diagnosis and management of perioperative anaemia have been proposed, but the effectiveness of these is beyond the scope of this review.12 Three studies in this review appeared to give iron without assessing the underlying cause of anaemia. All three showed a beneficial effect of iron, possibly because iron was used in the setting of iron deficiency, but this was not clearly reported, or because only a minority of patients had anaemia of another cause.
Three studies in this review used a predefined decision-making algorithm to determine preoperative anaemia treatment.29 31 38 This approach seems logical given there may be a different underlying cause of preoperative anaemia, differing tolerance to oral iron and variations in timing of screening in relation to surgery. This approach is also in keeping with international guidance.12 One study included a ‘safety-net’ of referral for further investigation if the Hb and/or ferritin levels were considered too low,31 in keeping with guidance from the British Society of Gastroenterology.53
As identified in this review there are different iron treatments available including oral iron salts, oral sucrosomial iron and intravenous iron preparations. While this review lacks high quality RCTs, which might allow us to recommend an optimum treatment modality, our exploratory analysis suggests intravenous iron correlates with a greater Hb increase than oral iron. However, no significant subgroup differences between iron preparations were seen for postoperative outcomes, although this analysis may have been underpowered and was not a randomised comparison between modes of delivery.
Debate continues around the optimal dose and administration technique for oral iron salts, to maximise absorption and reduce side effects. Recent recommendations involve lower daily or alternate day doses (40–100 mg elemental iron) along with specific administration advice54; newer phospholipid bound sucrosomial iron formulations offer a potential oral alternative. High-quality RCTs comparing the effectiveness of different dosing regimens, or testing newer oral iron preparations are required to direct future clinical practice.55
Concerns around the safety of intravenous iron exist based largely on the risks of anaphylaxis seen with older preparations. A network meta-analysis found them to be safe and effective at increasing Hb concentrations in anaemic and non-anaemic iron deficient participants, across a range of medical specialties.56 However, even with newer intravenous iron preparations further work may be needed to identify the optimum formulation. Bisbe et al34 compared intravenous iron sucrose with intravenous ferric carboxymaltose, and found they produced a comparable Hb response, but participants receiving intravenous ferric carboxymaltose required fewer treatment sessions to receive their total iron dose (mean 4 sessions vs 2 sessions, p<0.001). This is likely to be attractive to patients, clinicians and policy-makers, so an intravenous iron preparation that allows a total dose infusion may warrant further investigation.
Timing
There was considerable variability in the timing of commencing iron treatment before surgery. A recent international consensus statement on the management of perioperative anaemia and iron-deficiency recommends oral iron be given for 6–8 weeks prior to surgery and IV iron used if surgery is planned within 6 weeks.12 However, work by Muñoz et al found that even very short-term perioperative intravenous iron, given either 2–5 days preoperatively and/or 2–3 days postoperatively, significantly reduced transfusion rates and length of stay.57 Where oral iron was used in the studies included in this review it was typically for less than the 6–8 weeks recommended, which may be limiting the beneficial effects of oral iron seen.
Definition of anaemia
Two studies included participants with a presenting Hb greater than 130 g/L (tables 1 and 2)28 29 reported a beneficial effect of iron on postoperative outcomes (number of participants and units transfused and LoS). This may support the opinion that gender-specific definitions of preoperative anaemia are not appropriate, and might even suggest Hb thresholds of 130 g/L are too low.12 13 20
Strengths and limitations
Our review methodology followed a preregistered protocol and is reported in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidance.26 58 However, as with any meta-analysis, this review is limited by the included studies and despite our efforts it is possible some studies may have been missed. Comprehensive searching techniques were used and NRSI designs with a control group were included. Handsearching identified four additional studies, not found in the database searches.29 34 36 37 This initially raised concerns and prompted a review of the search strategy, but no major issues were identified. When looking closer at the source of these four studies it became clear that the database searches would not have been expected to identify them. Our comprehensive searches identified two non-English language studies. Despite our extensive searches, which included the grey literature to reduce the risk of publication bias, a funnel plot suggests there may be evidence of publication bias, though there were only ten studies and other explanations cannot be excluded.
Observational study designs and studies with low event rates, as seen in most studies in this review, are at higher risk of bias and may exaggerate treatment effects compared with well conducted, adequately powered RCTs.59 60 Although measures have been taken to explore the impact of low quality studies in our sensitivity analysis, the sparse data seen in many of the included studies, and the lack of any high quality RCTs in this review does limit the reliability of our results and the conclusions that can be drawn from them.60 Ideally RCTs and NRSIs would have been pooled separately due to differential risk of bias; however, given there was only a single small RCT we pooled this with the NRSIs.
Differences in how data on the quantity of blood transfused are reported, meant calculations to standardise these were required. Further work to define a standard definition for reporting, which would aid interpretation and data pooling, may be warranted.
Few studies measured patient adherence for those assigned to receive oral iron. It is well documented that adherence to oral iron salts can be an issue.61 There was also considerable variation in the timing and duration of treatments even within studies, with one giving oral iron for between 6 and 151 days. Given it would be expected to take 2–4 weeks to see a Hb response to oral iron, 6 days is almost certainly too short for any meaningful effect to take place.62 Both of these limitations may underestimate the true treatment effects of iron, yet despite this, significant clinical benefits are seen in this meta-analysis. In several studies there was little adjustment for confounders which may impact on a patient’s risk of receiving a blood transfusion notably presenting Hb concentration or cardiorespiratory comorbidities, which were often used to trigger blood transfusion. In addition, the use of other PBM interventions in routine use was poorly reported across the included studies, with most not reporting on these at all. Where they were, this was typically not quantified and only referred to as being in ‘routine practice’. These potential confounders were therefore typically not well controlled or adjusted for across studies. This review also included studies where a treatment in addition to iron was given for up to 20% of participants, this was designed to be pragmatic but may have amplified the results in relation to the true effectiveness of iron. However, only two participants received concurrent EPO, and this study was excluded during sensitivity analysis. In addition, observed improvements in LoS should be considered on a background of general reductions in LoS for elective THR or TKR over time.63 64
Conclusion
Based on the best available evidence, preoperative anaemia management with iron in participants undergoing elective THR or TKR significantly reduces the number of participants requiring RBC transfusion, the number of units transfused and LoS. However, these results should be interpreted with a caution as high-quality evidence is lacking.
Acknowledgments
We would like to thank Prasanna Sarathy and Iyn-Hyang Lee for their assistance in the translation, data extraction and quality assessment of the two non-English papers.
References
Footnotes
Twitter @abscrimshire, @AliBooth42
Contributors ABS: designing the meta-analysis, collecting and analysing the data, preparing and writing the manuscript. AB: assisted in study design, collecting and analysing data, approving the manuscript. CF: assisted with statistical analysis, approving the manuscript. AK: assisted with conceptualising the study and approving the manuscript MR: assisted with conceptualising the study and approving the manuscript. CM: assisted with study design and approving the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.