Article Text

Abstract
Objectives Socially assistive humanoid robots are considered a promising technology to tackle the challenges in health and social care posed by the growth of the ageing population. The purpose of our study was to explore the current evidence on barriers and enablers for the implementation of humanoid robots in health and social care.
Design Systematic review of studies entailing hands-on interactions with a humanoid robot.
Setting From April 2018 to June 2018, databases were searched using a combination of the same search terms for articles published during the last decade. Data collection was conducted by using the Rayyan software, a standardised predefined grid, and a risk of bias and a quality assessment tool.
Participants Post-experimental data were collected and analysed for a total of 420 participants. Participants comprised: older adults (n=307) aged ≥60 years, with no or some degree of age-related cognitive impairment, residing either in residential care facilities or at their home; care home staff (n=106); and informal caregivers (n=7).
Primary outcomes Identification of enablers and barriers to the implementation of socially assistive humanoid robots in health and social care, and consequent insights and impact. Future developments to inform further research.
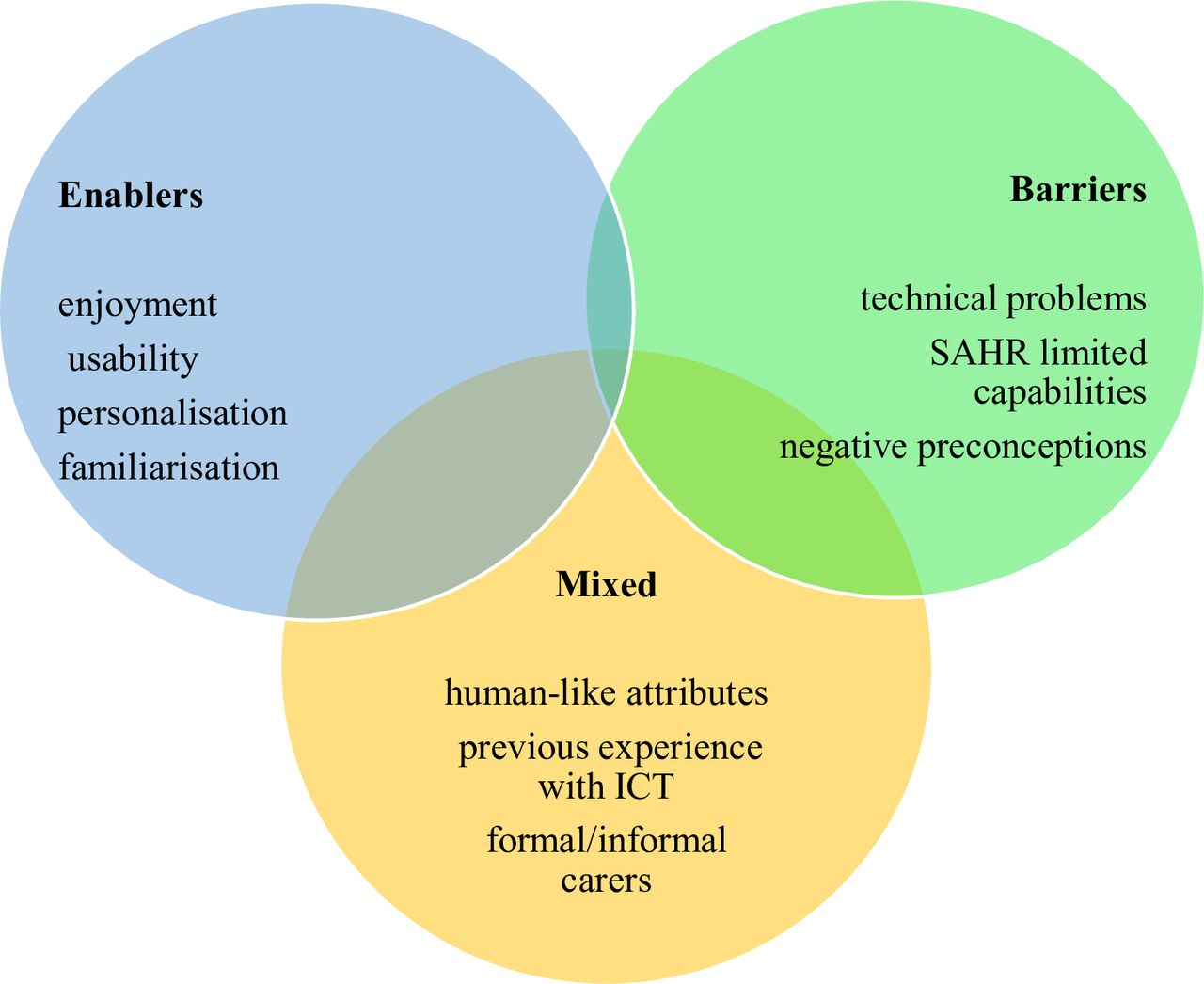
Results Twelve studies met the eligibility criteria and were included. None of the selected studies had an experimental design; hence overall quality was low, with high risks of biases. Several studies had no comparator, no baseline, small samples, and self-reported measures only. Within this limited evidence base, the enablers found were enjoyment, usability, personalisation and familiarisation. Barriers were related to technical problems, to the robots’ limited capabilities and the negative preconceptions towards the use of robots in healthcare. Factors which produced mixed results were the robot’s human-like attributes, previous experience with technology and views of formal and informal carers.
Conclusions The available evidence related to implementation factors of socially assistive humanoid robots for older adults is limited, mainly focusing on aspects at individual level, and exploring acceptance of this technology. Investigation of elements linked to the environment, organisation, societal and cultural milieu, policy and legal framework is necessary.
PROSPERO registration number CRD42018092866.
- socially assistive humanoid robots
- artificial intelligence
- health and social care
- older adults
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
- socially assistive humanoid robots
- artificial intelligence
- health and social care
- older adults
- systematic review
Strengths and limitations of this study
This review is the first to date focusing on the issues related to the pragmatic implementation of socially assistive humanoid robots in health and social care settings catering to the needs of older adults.
Quality assessment of the included studies was based on two combined tools to account for the heterogeneity of the underlying study designs.
Three authors were involved in critical steps of the review (article selection, data extraction, quality assessment of the included studies), and this constitutes a strength of this study.
The heterogeneity between studies on key issues, such as participants’ cognitive health and residential context, study designs and outcomes, prevents quantitative synthesis and hampers consistent assessment of the implementation of socially assistive humanoid robots in health and social care.
Introduction
Rationale
The current global landscape in health and social care is highly challenging, demanding innovative and effective actions from policy makers and service providers. For example, it is projected that by 2050 the world’s population over the age of 60 years will be about two billion, an increase of 900 million from 2015.1 Shortages of healthcare professionals and a growing ageing population place enormous pressures onto the health and social care systems of many countries. Older adults are living longer with chronic problems and/or disabilities. At the same time, the size of formal and informal healthcare workforce is shrinking.
The use of artificial intelligence (AI) and robotics provides a major opportunity towards meeting some of the care needs of older adults.2 3 An advanced form of AI is the one used in socially assistive humanoid robots (SAHRs). These robots use gestures, speech, facial recognition, movements and, in general, social interaction to assist their users.4 The robot’s goal is to create close and effective interaction with the human user for the purpose of giving assistance and achieving measurable progress in convalescence, rehabilitation, learning and well-being.
In a systematic review of the literature about the use of different available technologies directed to assist older adults, robotic devices and robots were viewed as an encouraging technology that can assist and prolong older adults’ independent living.5 Corroborating this finding, a few additional reviews of the literature have indicated that: (i) SAHRs could have multiple roles in the care of older adults such as in affective therapy and cognitive training6 and (ii) they could be beneficial in reducing anxiety, agitation, loneliness and improving quality of life, engagement and interaction (especially when used as a therapeutic tool when caring for patients with dementia).7–9 In addition, reviews related to the acceptance of robots have found it being influenced by numerous factors, such as the perceived need for the technology, the user’s previous experiences with it, age, level of education, expectations about what the technology can do, attitudes and cultural background;10 in fact, robots that were programmed to use verbal and non-verbal communication familiar to the user and to their cultural background were more easily accepted by users.11 Furthermore, a review of qualitative studies on older adults’ experiences with socially assistive robots revealed the complexity of issues associated with their use with older adults, and how these impacted on their attitudes towards robots.12 For example, issues related to the ‘role’ that the robot could acquire and to the nature of the human–robot interaction (HRI) revealed a mixture of opinions and emotions. Parallel enquires among health and social care professionals have identified various areas where humanoid and animal-like robots can be helpful, but reported mixed views about their use in healthcare settings, raising issues of staff and patients’ safety, and the protection of their privacy.13 On a similar note, a recent qualitative exploration among different stakeholders in the healthcare context revealed that ethical and legal challenges, the lack of interests from professionals and patients, and concerns related to the robot’s appearance and robotic expectations were major barriers to their potential use.14 Frennert et al’s review15 focused mainly on concerns that need attention when considering the social robots and older adults interface, and urged developers to adopt a more pragmatic and realistic idea of an older adult. Their recommendations addressed the inclusion of older adults in the development process, without considering them incapable of expressing their needs and offering possible solutions to their own problems.
All current reviews shed some light on certain aspects of this complicated relationship: older adults and socially assistive robots. However, in order to effectively meet the care needs of an ageing population, it is imperative to identify and disseminate the full range of evidence-based information of this form of technology. Such evidence will enable people to discuss the possible solutions offered by SAHRs, in a more measured and informed way. This is particularly important in our days, since public attitudes towards robots may be also influenced by the media, often in negative ways. As an instance, while the use of robots will undeniably change the workforce, many people believe that these changes will only be negative. Example of catastrophic depictions of the use of AI in health and social care are that robots will take over human professionals’ jobs, that robots will be dangerous, or that they are incapable of providing care that is culturally appropriate and compassionate.16–19 In fact, the McKinsey Global Institute, along with a recent analysis led by PricewaterhouseCoopers, revealed that ‘smart automation’ that uses AI and robotics will be disruptive for many industries; yet some industries will be affected more than others. For example, in transportation and financial industries many low skills jobs that require repetitive tasks will be heavily affected. On the other hand, the healthcare sector will neither be affected in the same magnitude nor in a similar way.20 Overall it is estimated that about 75 million to 375 million workers will have to change their occupation by 2030.21 In the USA, employees in manufacturing, retail and accounting appeared more worried that AI would impact their jobs, whereas teachers, doctors and nurses were less so.22 The Topol Review—that focuses on how the UK National Health Service (NHS) needs to prepare for the digital revolution—projects that, over the next 20 years, 90% of all NHS jobs will require the handling of data and the need for some digital skills.23 The healthcare workforce will need to be educated in digital literacy according to their professional role, and new roles will be created as well. Similarly, in other industries it is projected that AI requires very specialised skills, and therefore the need for new technical jobs will increase in order to use robots in practice.22 24 However, at least in the healthcare sector, nurses and other health professionals are seen working along with robots.25 It is estimated that about 8%–16% of nursing time is consumed on a variety of non-nursing tasks that could be delegated.26 Using robots for such tasks could free nurses’ time to be spent in patient care.
Objective
Our review aims to understand what the current enablers and barriers to the use and implementation of SAHRs are, and concentrates on articles that describe the actual use of SAHRs among older adults. The primary focus is on exploring and identifying the factors that might facilitate or hinder the implementation of SAHRs in health and social care for older adults.
Methods
Information sources and search strategies
The search strategy was developed for MEDLINE with appropriate modifications to match the terminology used in other databases. Databases were searched between 9 April 2018 and 8 June 2018. In view of the recent adoption of this form of technology, we limited the search date to the previous ten years. Subject headings and free text terms were used according to the specific requirements of each database. Box 1 presents full search strategy with search terms across the following bibliographic electronic databases: the Cochrane Central Register of Controlled Trials; 2017 MEDLINE via OVID; Embase via OVID; Science Citation Index; Cumulative Index to Nursing and Allied Health Literature; Latin American and Caribbean Health Sciences Information database; IEEE Xplore digital library; PsycINFO; Google Scholar; European Commission and Eurobarometer. We also conducted the following additional searches: ACM Digital Library; Computer Source Lecture Notes in Computer Science; Science Direct. In addition to traditional searching, reverse citation screenings of the reference lists of relevant articles (ie, including the key terms such as SAHRs and home care) and forward citations (articles which have cited the identified papers) were conducted. The references of eligible reports and key review articles were examined for other potentially relevant studies.
Core set of search terms
‘socially assistive robot*’ OR ‘socially assist*’ OR ‘social assist*’ AND robot*
AND ‘social care’ OR ‘home care services’ OR ‘home care’ OR ‘care home*’ OR ‘nursing home*’ OR ‘residential facilit*’ OR ‘assisted living facilit*’ OR ‘group home*’ OR ‘home* for the aged’ OR ‘community health services’ OR ‘self-help devices’ OR self* AND care* AND management AND help OR ‘social support’ OR ‘interpersonal relations’ OR ‘nursing care’ OR ‘point of care’ OR ‘aged care’ OR ‘activities of daily living’ OR care* OR healthcare OR social*
NOT Animals NOT Infant OR Child* OR pediatr* OR paediatr*
All records were uploaded into Rayyan software, a systematic review software, similar to Covidence,27 for managing citations for title and abstract screening and study selection.28 The software was used for the process of de-duplicating, and independently exploring, screening abstracts and full texts, excluding and including studies based on pre-specified criteria. Any disagreements regarding eligibility were discussed, and, if required, a third researcher was consulted, and consensus reached. Figure 1 summarises the selection of studies in accordance with PRISMA guidelines.29

PRISMA flow chart.
Selection criteria
Studies that considered the application of SAHRs only (ie, not animal-like robots) in health and social care were included. These were not restricted to experimental designs (table 1). In view of the likelihood of a paucity of potentially eligible studies relevant to this clinical topic, we also considered observational, cohort, case-control and qualitative studies. Editorials, conference abstracts and opinion pieces were excluded. Only adult and older adult care settings were included (eg, long term, rehabilitation, inpatient and outpatient hospital care, community and social care). The target population covered all stakeholders who were part of the process of implementation of SAHRs in health and social care in the broadest perspective (eg, users, staff, caregivers), and it was not limited to the aged population. Studies that included any type of direct exposure to SAHRs were selected.
Risk of bias and quality assessment of included studies
Data extraction and synthesis of the results
Study details and outcome data were collected independently by two researchers with a piloted data extraction form (see online supplementary file 1). The process was validated by assessing the data extraction form on a small number of studies (n=4) that two researchers assessed independently and compared. Type of study/design, date of publication, country and specific setting (ie, care facility), intervention (ie, type of SAHR), sample and characteristics of participants, and primary outcomes were identified (table 2). Primary outcomes entailed the identification of enablers and barriers to the implementation of SAHRs in health and social care. Barriers were defined as those impeding the implementation of SAHRs which may include factors, issues or themes at local, system or policy level. Enablers were defined as mechanisms and initiatives whereby patients, providers or policy makers contribute to facilitating the positive uptake and implementation of a SAHR.
Supplemental material
Summary table of included studies
The heterogeneity of the studies included in this review did not enable a standard quantitative synthesis (ie, meta-analysis) to be performed. Instead, a narrative synthesis of the results was conducted and presented in the form of a summary table (table 2) and figure (figure 2). All results were discussed and weighted by three researchers with the aim of identifying a frequency-based ranking of importance in relation to enablers, barriers and mixed results. Any uncertainties were resolved via a consensus-based decision. The protocol for this systematic review has been registered and published on PROSPERO.
{kind=link}
{kind=link}
Summary of results. ICT, information and communications technology; SAHR, socially assistive humanoid robots.
Results
Search results and included studies
A total of 12 studies were included in our analyses: 6 mixed-method, non-randomised user experience trials30–35; 2 pre-post experimental surveys36 37; 1 mixed-method, longitudinal experience trial38; 2 post-experimental surveys39 40; and 1 ethnographic study41 (see Figure 1).
Assessment of risk of bias and quality of included studies
The quality of studies was assessed for all included studies with the following two assessments tools: the Cochrane Collaboration’s tool for assessing risk of bias42 and the critical appraisal for public health43 (table 1). The research team decided that two researchers independently assessed four (ie, 1/3) of included studies and compared their results in order to ensure the validity and reliability of the process. Disagreements were resolved via the involvement of a third member of the research team and group discussions.
None of the selected studies had an experimental design; hence overall quality was low with high risks of biases (table 1). Most studies had no comparator and no baseline.30–35 38 40 41 Additional methodological limitations affecting the non-randomised, quasi-experimental design of the studies were: very small samples’ sizes, with only one study involving more than 100 participants38; and self-reported measures,30 34–37 39 40 not always in combination with observation and/or data retrieved from the robot.31–33 38 Seven studies33–35 37 38 40 41 used validated instruments informed by existing theoretical models44–47; two studies reported the drop-out rate but did not mention the handling of missing data.32 37 Three studies did not report any information on ethical approvals or consent received from the participants.31 38 39 Protocols, trial pre-registration and fidelity checks were not found in any of the studies. Four studies reported no information about funding.33 35 38 40
Characteristics of selected studies
Table 2 presents characteristics and outcomes of the 12 included studies.
Population
Post-experimental data were collected and analysed for a total of 420 participants, including 73% of older adults (n=307), 2% of informal carers (ie, older adults’ children, n=7) and 31% of formal caregivers and staff (n=106). The cohort of participants in two of the selected studies was the same34 35; however we resolved to count participants twice because aims, measures and results of the two studies were different. In 11 of the 12 selected studies, participants were older adults aged ≥60, with an overall mean age of 79.8 years. Among these 11 studies, 1 also included professional and informal caregivers,30 and 2 considered residential care facility (RCF) staff.32 41 One study only involved staff in a RCF for younger adults affected by neuropsychiatric conditions.37 Three studies included older adults affected by dementia and other conditions of ageing-related, cognitive impairment.31 32 38 One study compared older adults affected by mild cognitive impairment with a cognitively intact healthy (CIH) group,33 whereas another one did not compare the two groups.36 Five studies selected CIH older adults,30 34 35 40 41 whereas in another one participants’ condition was not reported.39 Since one study did not report the gender of the 55 older adults taking part in the study,41 out of 365 participants, 69% were women. Participants’ level of education was only considered in three studies where over 80% of participants had at least a bachelor’s degree.33 36 39
Similarly, in the four studies where data were collected on general information and communications technology (ICT) skills, 76% (n=66) of 87 participants reported regular computer use.31 33 36 39 In other two studies,34 35 highly experienced technology users were excluded, following assessment. In these two studies, information around previous contact with a SAHR on behalf of research participants is not explicit. However, if we assume that high ICT experience implies previous contact with a SAHR, none of the participants across all the studies had had any hands-on experience with SAHRs before taking part in the studies.
The largest post-experimental group consisted in Australian participants (n=123). All the earlier figures includes neither data of subjects who dropped out in pre-post studies37 39 nor all data collected via observation of HRIs or interviews, as sometimes this information was irretrievable or not reported.32
Settings and interventions
Four trials were carried out in RCFs,32 37 38 41 six in smart environments or university laboratories,30 33–36 39 and two in a combination of private apartment, RCF and laboratory.31 40 None of the studies was conducted in an acute healthcare setting. Studies were conducted in the following countries: six in a European context (Austria, UK, Netherlands, France);30–35 and two of these six in Israel as well;34 35 two in Australia;37 38 two in Japan;40 41 one in Canada;39 and one in the USA.36
All studies included interventions where participants had their first hands-on experience interacting with a SAHR. Eight different types of SAHRs were used which had different appearances, bodily movements’ abilities, often an additional mode of interaction beyond voice-based (ie, built-in touch screen, touch sensors, tablet remote control). All were customised with software packages providing a range of specific services.
In most studies, a pilot field test was conducted to establish familiarisation. Pilot testing was deemed necessary particularly in those experiments where participants had to interact with the SAHR in highly structured scenarios performing specific tasks, sometimes following instructions.30 31 33–36 40 This type of HRI lasted between 45 min30 and up to 6 hours.38 Three studies adopted a design whereby HRI was not structured, and RCFs residents and members of staff freely chose to interact with the SAHR.32 37 41
The HRIs in the 12 exposures involved the following services and activities: playing cognitive games such as Bingo, Hoy and general knowledge games, including an orientation game with the support of pictures, ‘21 questions’ and ‘Simon says’ game;31 33 36–39 listening to music, singing, storytelling, relaxation, dancing (including joint chair exercise) and physical training (including walking);34–38 40 48 carry and delivery tasks;30 31 call to a friend, calendar and reminders such as to drink water, to do exercise, to take medication;30 31 33 34 weather information;34 37 restaurant finding;39 and reception, greetings and interactions;32 41medical measurement.35
Narrative synthesis
Findings in terms of enablers and barriers are presented below and summarised in figure 2.
Enablers
Enjoyment
An enjoyable experience was found to be a crucial factor conducive to SAHR’s use and implementation. In ten trials (83%) participants highly valued enjoyment and engagement when interacting with the SAHR, both in terms of general positive HRI experience (eg, SAHR’s kindness, friendliness, provision of comfort and motivation) and in relation to specific activities (eg, listening to music and playing games). In one study only,34 it is reported that participants to the long-term trials of the intervention commented negatively with respect to their enjoyment in interacting with the robot, and furthermore that this would decrease over time.
Usability
Intuitiveness and easiness of use proved to be essential enablers towards the implementation of SAHRs in six studies (50%).30 31 33 34 36 38 Usability is to be broadly intended in terms of lack of technical issues, intuitive interface and design factoring participants’ disabilities.
Personalisation
Engagement and enjoyment were found to be interlinked with the personalisation of services, hence ultimately with overall use and implementation. Personalisation should account for: adaptation to users’ taste and preferences;38 40 user’s care needs,30 context and routine;31 41 and users’ impairments.33 38 41
Familiarisation
Inasmuch as the robot should offer individualised services, users also should learn about and adapt to the robot’s status and intentions.31 While the model of human–robot co-dependent relationship is prominent in one study only,31 other studies found familiarisation to be an important factor positively affecting implementation.33 34 36 38 Interestingly, in one of these studies participants felt that not only over time ease of use would improve, but also that the relationship with the SAHR may turn into a friendship.34
Barriers
Technical problems
Over half of the studies30–32 34 35 37 41 explicitly stated that technical issues with the robot itself constituted a barrier to SAHR’s implementation in health and social care.
SAHR’s limited capabilities
The limited performance (ie, mobility, robots’ voice, lack of interactive element) of the robot was found as a crucial barrier to use. This impediment was explicitly reported in four studies,30 32 35 41 while more implicitly in other three, where the robot’s restricted skills were described in terms of limited personalisation of services,38 adaptability34 and co-learning/self-training abilities.31
Negative preconceptions
In a study, health professionals’ assumptions on older adults’ capacity to interact with SAHR were included among the barriers to implementation.37 Two other studies elaborated on the negative views towards robots in terms of dehumanisation of care and society,32 33 and of stigmatising effects associated to being a dependent individual in decline.33 In three studies, negative preconceptions came from formal and informal carers rather than from older adults themselves.30 32 37
Mixed views
Human-like attributes
One study showed that human-like appearance was appreciated by one-third of the participants.36 Another study reported that human-like communication was preferred over human-like appearance.39 In the same study, 80% of the subjects completing the trial were older women who declared to prefer a male looking SAHR with male voice.39 A third study concluded that SAHRs based on human-centred system with human-like characteristic are likely to enable acceptance and use.38 However, in the same study, it was also reported the fact that the SAHR was not judgemental facilitated interaction.38 The ambivalence of having a non-judgmental conversational partner (ie, non-human) who was also given the overt social role of a human child was found beneficial to implementation in a fourth study.41 SAHR’s child-likeness was also found positive in a fifth study, and SAHR’s small size was appreciated, although contributing to reduced acceptance with low scores in attributed animacy and naturalness.35 Similar ambivalent results are found in a sixth study where again SAHR’s small anthropomorphic shape was at the same time responsible for low levels anxiety, but also for low scores in perceived social presence.34 In relation to social presence participants had contrasting views (ie, SAHR seen as pet or a conversational partner). Differently from these last studies, in a seventh one participant did not choose to walk side-by-side with the SAHR, as it would be natural with a human partner, but chose to follow the SAHR, giving it the role of a guide.40 Finally, in an eighth study, the lack of more complex social interaction was identified as a barrier to implementation.30 None of the other studies provided any indication regarding the cultural attributes of the SAHR. In one study only, it is reported that the fact that the SAHR was speaking the same language of the users was responsible of higher perceived ease of use compared with the cohort where the SAHR was not using the users’ native language.34 In another study, it was argued that the positive reception of the robot may be also attributed to the nature of the local culture (ie, Japanese) towards robots.41
Previous experience with ICT
While one study found that previous experience with technology positively correlated with use,30 another trial found that there was no relationship between previous experience and ease to use.39 In other two studies, highly experienced ICT users were excluded from participating in light of the argument that acceptance is positively influenced by ICT experience.34 35
The role of formal and informal caregivers
As mentioned earlier, the negative attitudes of formal and informal carers have been shown to constitute an impediment to SAHR’s implementation.30 32 37 Conversely, two studies highlighted the enabling effect of the encouragement for SAHR’s use on behalf of relatives and professionals.33 41
Discussion
Summary of evidence
Our review focused on the identification of factors that could facilitate or hinder the implementation of SAHRs in health and social care. We focused on actual interactions of older adults with social humanoid robots in different settings, in order to better understand what the current issues are in regard to implementation. Enablers, such as enjoyment and personalisation, were mainly related to the use of robots at an individual level. The element of enjoyment in the HRI was also elsewhere found to be crucial among hospital patients,49 opening the doors for considering social humanoid robots as an intervention to combat social isolation in hospital settings.
Barriers were related to technical problems and to current limited capabilities of the robots. Technology malfunction and/or technology limitations were reported as areas of concern, similar to the results of a recent survey of Korean nurses.50 Surprisingly for the heavily regulated field of healthcare, the issues of safety, ethics and safeguarding were not identified in this review as significant implementation-related factors, even though nurses and healthcare workers have been raising these issues. Safety and ethical issues were reported as major concerns in previous systematic reviews, and it is imperative that future research investigates these issues and understands their implications. The field of social humanoid robots poses many ethical challenges especially because robots could be designed to assume different roles and for different purposes: from service robots assisting in concierge types jobs to companion robots. In agreement with Vandemeulebroucke et al,51 we believe that an ethical approach demands that all stakeholders should have a voice in the current debate, but also in the design of future technologies, their application and implementation. We also agree with Chou et al 52 that future planning should view all these factors under a broader policy framework, and policy makers should work collaborative to ensure the ethical and safe implementation of robots. The European Commission advocates for the use of a new framework to address the ethical issues in healthcare robotics called ‘Responsible Research and Innovation’.53 Under this framework, society, users and innovators are mutually responsive and engage in an interactive and transparent process in order for acceptable, sustainable and desirable products to be developed and embedded in our society. Similarly, the Alan Turing Institute calls for the use of a framework of ethical values that need to guide every AI project, and they introduce the use of four actionable principles: (i) fairness, (ii) accountability, (iii) sustainability and (iv) transparency.54 These principles are reflected onto the current UK code of conduct for data-driven health and care technology,55 and onto the current policy paper for the safe and ethical introduction of AI in the NHS.56 Fairness refers to the avoidance of bias and discrimination, for example, and according to it, the AI system should use only fair and equitable data. Accountability refers instead to the auditability of the system, ensuring that responsibility of all actions is established throughout the AI system, from the design to the final implementation. Sustainability of the system refers to the safety, reliability, accuracy and robustness of the system. Finally, transparency covers the ability of the designers to always explain how the system is working and how it will affect its users. Ensuring the use of ethical guidelines in the design of AI and robotics interventions is critical since many interventions are still designed without the consideration of ethics.57
Robot’s appearance30 36 38 39 and views of carers and relatives provided mixed results.30 32 33 37 In regard to the appearance, Mori’s theory of the ‘uncanny valley’ is illuminating.58 Between the animated and the perfectly realistic, human-like appearance of robots, there is an area where depictions can create uncomfortable feelings in humans. Therefore, life-like attributes of the robots, such as voice, facial expressions, gestures, bodily appearance, cultural attributes and gender, have an impact on how the user experiences the robot, and on the HRI. The indeterminacy of robots’ appearance is reflected onto the dramatic variations of SAHRs found in the literature. We also know that one’s cultural background influences views and perceptions of the robot’s aesthetics,11 but none of the studies provided any indication regarding the cultural attributes of the SAHR. Culturally specific research on the relationship between appearance, acceptance and implementation is therefore promising in HRI studies.
According to our protocol, we searched for factors affecting the implementation of SAHRs by key stakeholders, such as health professionals. The role of formal and informal caregivers has been found as crucial.59 However, the information we could yield was limited and mixed, and this is an area that urgently requires further research, involving longitudinal studies and larger samples. Longitudinal studies can provide the opportunity to investigate whether fear of using a new and unfamiliar technology, or losing interest in a new technology (diminishing novelty effect), are related to negative attitudes. Abbott et al 8 in their review of the use of social robotic pets (animal-like social robots) found similar mixed feelings from the different stakeholders. The fact that people have very strong feelings on the opposite sides of the spectrum, either very positive or very negative, is significant to implementation and requires a careful investigation. The current Topol Review23 addresses the changes and accompanied needs of the healthcare workforce that will be imposed by the digital revolution. It calls for an urgent need to educate and prepare the healthcare workforce for the imminent digital changes and for an organisational cultural change. However, it is hard to think how these transformations will happen when the current evidence reveals the existence of mixed opinions and negative attitudes at least towards the use of socially assistive robotic technologies.
The completeness and overall applicability of the evidence are limited, mostly because it provides only insights into individual-level factors related to the acceptance of technology. This can be partly attributed to the main theoretical framework used in the studies. The technology acceptance model (TAM) proposes in fact an explanation for a person’s actual and intentional use of a technology, through an exploration of their attitudes towards it.44 The lack of evidence related to other main key stakeholders, such as formal and informal carers, along with factors related to the environment, policy, society and organisation is a major limitation. Exploring attitudes of other populations, such as formal caregivers, as well as the use of other theoretical models, is considered critical. The field would benefit, for example, from the use of the diffusion of innovations theory (DIT),60 when considering research questions related to the use of SAHRs in healthcare; but also from theories that explore the co-existence of technology and caring, such as the theory of technological competency as caring in nursing.61 King and Barry62 recently introduced a theoretical model that highlights caring theories when considering the design of healthcare robots. Understanding how nursing care will change, or what will be the best interface of nurses with SAHRs is critical. In addition, how compassionate care will be understood, expressed and studied is also essential. The Papdopoulos model that integrates compassion into culturally competent care would be useful in exploring the interrelations between service users, nurses, health professionals, family members and SAHRs.63 Furthermore, researchers working in the area of HRI among older adults are calling for new ways to conceptualise ageing and consequently robotic technologies. In particular, they advocate that the use of socially assistive robots should be studied under a model that focuses on ‘successful aging’ rather than a ‘deficit model of aging’. They argue that the latter model—viewing ageing a process of continued losses and older adults needing assistance—restricts the design of new technologies. A successful model of ageing that focuses on the preservation of the user’s autonomy can instead provide new ways of using, designing and implementing socially assistive robots.64
Limitations
As per protocol, our intention was to explore enablers and barriers to the implementation of SAHRs in both health and social care but, in fact, most of the activities assessed were more relevant to social care. Even medication reminders, which are obviously health-related, form an important part of social care. There is therefore little to inform health practitioners as to the possible application of SAHRs in health settings. Furthermore, very few studies have deployed and implemented SAHRs in health and social care settings; hence the available information is scant. In addition, quality of the studies is problematic (table 1).
The heterogeneity of study designs led to the identification of factors in single studies. For example, only one study reported on the level of education as enabling factor of SAHR’s acceptance.36 Another study found that fear of making mistakes with technology was a barrier to implementation.32 However, in another study, uneasiness with technology seemed to be counterbalanced by a sense of discovery and being up-to-date with ICT.33 The evidence is too scant to generalise these initial findings, and further research is needed to assess the impact of these, and other factors, onto SAHR’s acceptance and implementation in health and social care.
Conclusion and perspectives
The use of SAHRs is promising in responding to some of the care challenges of an ageing population. This systematic review summarised the enablers and barriers to the implementation of SAHRs in health and social care. Evidence suggests that enjoyment and personalisation are the chief enablers to the implementation of robots, while the two most important barriers had to do with technical problems and the limited capabilities of the robots. However, there are limitations to the evidence, as most studies were at high risk of bias involving very small samples. Gaps in the evidence include factors related to environment, organisation, socio-cultural milieu, policy and legal framework. Furthermore, the research focus has currently been placed on understanding the acceptance of robots by adult users, but there is no discussion of the needs of the healthcare workforce on a professional level, and how these needs are being met by educational institutions, professional organisations, and employers.
Acknowledgments
We would like to thank Dr Zbys Fedorowicz for his contributions and helpful advice.
References
Footnotes
Contributors IP and CK conceived and designed the study. CK and SA acquired, screened and conducted the initial data extraction. IP acted as a referee in the screening, analysis and interpretation of the data, which was conducted by CK and RL, who both drafted the manuscript, and IP provided the critical review of it. All authors approved the version to be published and agreed to be accountable for all the aspects of this work.
Funding This work was supported by CARESSES project (Horizon 2020, Grant Agreement ID: 737858).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval was not required for this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.