Article Text

Abstract
Purpose The North Texas Concussion Registry (ConTex) was established in 2015 as a multi-institutional collaboration intended to study risk factors, recovery patterns and clinical outcomes associated with concussion across the lifespan, with a particular emphasis on sport-related concussion.
Participants Prospective enrolment of individuals who sustained a concussion within the past 6 months who were seen at one of four North Texas ConTex concussion clinics which employ common diagnostic criteria and assessment metrics to evaluate effects of a concussion as well as longitudinal tracking of recovery.
Findings to date The ConTex database and multidisciplinary oversight team has been established, and over 1700 participants aged 5–88 years have been enrolled. A majority of concussions were sport-related (60%), with a mean age of 17.5 years and similar numbers of males and females. Three-month follow-up compliance has been excellent (86%), with a majority of subjects reporting good recovery by that time. ConTex has provided a rich data source for multiple research projects focused on concussion characteristics, risk factors and outcomes, and led to the development of a statewide youth concussion registry.
Future plans ConTex data are being analysed to add to the body of knowledge regarding concussion mechanisms, factors related to recovery and improving outcomes for concussion patients. ConTex will serve as a platform for future treatment studies and may serve as a model for other concussion surveillance programmes.
- sports medicine
- neurology
- psychiatry
- rehabilitation medicine
- neurosurgery
- statistics & research methods
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a large prospective longitudinal study of concussion, which includes a wide range of age and injury mechanisms to allow for robust data analysis of variables including age, sex, injury mechanism, risk factors, symptoms, objective test results and recovery metrics using standardised assessment tools at initial clinical assessment and 3-month follow-up.
The study design, oversight team structure, methods of data capture and variables relevant to concussion may serve as a model for other concussion surveillance programmes.
Enrolment of subjects from multiple clinical sites and involvement of varied providers allows for a real-world analysis of concussion assessment and management.
The variety of clinicians across several sites could lead to variance in outcomes, although standardisation of procedures, regular meetings of site leadership and routine monitoring of data quality are in place to address this.
Data collection is from four primary concussion clinics in North Texas, with limited sample diversity, a reliance on self-report instruments and an emphasis on sport-related concussion; thus, extension to other populations will be important.
Introduction
The Centers for Disease Control (CDC) estimates that there are over 3.8 million concussions annually, with some 2.5 million US students in grades 9–12 sustaining a sport-related concussion (SRC) each year.1 2 These CDC estimates of concussions are based on cases reporting to emergency departments, and likely represent only a proportion of all concussions, as many go unrecognised, unreported or present to general practitioners or specialty clinics.2 Due in part to growing awareness in professional sports and publicity from high-profile athletes, SRC has received increasing attention in recent years.2–4 Despite a dramatic increase in concussion-related research, relatively little is known about the true epidemiology, risk factors and predictors of recovery.3 5 Multiple studies have reported increased concussion rates over time, although this may be due to greater vigilance and awareness of SRC.6 Although there are a number of large concussion studies, many do not reflect clinical practice, are limited in scope/depth, are retrospective and/or are designed around global injury-related or specific investigative efforts (eg, geared towards more serious traumatic brain injuries (TBIs) or specific age ranges).7–11
In order to help address these gaps in knowledge, the North Texas Concussion Registry (ConTex) was launched in the fall of 2015. The goal of this project is to prospectively obtain detailed information from participants across the lifespan who sustain a concussion in order to study local concussion trends, demographic factors, injury mechanisms, clinical outcomes and identify risk factors for prolonged recovery. Although the focus of ConTex is on SRC, and participating clinics were selected to reflect this emphasis, non-SRC injuries are also included to allow for analysis and comparison of various mechanisms and trends.
Cohort description
Study design and overview
ConTex is a longitudinal cohort study that includes an initial injury and clinical characterisation component and a 3-month follow-up. Participants are recruited from local concussion clinics in the North Texas area, including Texas Scottish Rite Hospital for Children, Children’s Health, the University of Texas Southwestern Medical Center and Texas Health Resources Ben Hogan Sports Medicine (recruitment from the Texas Health Resources ceased 1 October 2017 when the clinic closed for reasons unrelated to our study). Primary care physicians, athletic trainers, team physicians, school nurses and emergency department physicians determine an initial diagnosis or suspicion of a concussion and then refer the potential subject to a ConTex clinic, where patients are seen as a part of routine clinical care and whose staff include faculty from the University of Texas Southwestern Medical Center. ConTex providers trained in the recognition and treatment of concussion then determine a diagnosis of concussion based on the Berlin Consensus Statement,12 an internationally accepted concussion resource. If a subject receives a concussion diagnosis and also meets ConTex eligibility criteria (table 1), they are informed of the study by ConTex personnel during their initial clinic visit. Those who express interest in participating provide written informed consent (assent is obtained from minors in addition to consent from parents or legal guardian) (see online supplementary file).
Supplemental material
ConTex inclusion/exclusion criteria
Each ConTex site has a designated site leader that serves on the ConTex Steering Committee, which provides scientific oversight to the project. This multidisciplinary group meets quarterly to review study progress, recruitment issues, scientific review of data and vetting of new projects as they are proposed. Each ConTex site also has a research coordinator that is responsible for screening and consenting participants, conducting semi-structured interviews, administering questionnaires and inputting data at the initial visit.
Data collected during the initial visit include information obtained from participants, parents/guardians as applicable and a review of the medical record (injury characteristics, concussion history, demographics, personal and family medical history, etc). Subjects are included if they have sustained a concussion within the past 6 months in order to provide a realistic depiction of concussion referrals to our clinics and to allow for a broader analysis of data and groups based on time-since-injury. Additional information specific to SRC such as level of play (school/club), activity at time of injury (game/practice) and sport-specific factors (helmet/no helmet) are recorded. Participants complete questionnaires that address some of the major clinical outcome domains of interest, including screening for depression, anxiety, sleep quality and current symptoms. Treatment and recovery information (eg, what treatments were prescribed, duration of symptoms and extent to which subjects feel they have recovered, etc) is also collected. Parents are asked to complete questionnaires on behalf of their children for subjects under age 12, and a primary email address and phone number is obtained for follow-up participation.
Three months following the initial clinical visit, an email notice is sent to participants that includes a link to a secure database consisting of a subset of questionnaires administered at the initial visit in addition to questions regarding symptom recovery, return to play/normal activity timeline and functional status. Telephone contact is made if subjects do not complete online follow-up materials. Participants are compensated US$15 at enrolment and another US$25 after completion of the online follow-up via a Visa debit card (Greenphire ClinCard).
Data collection
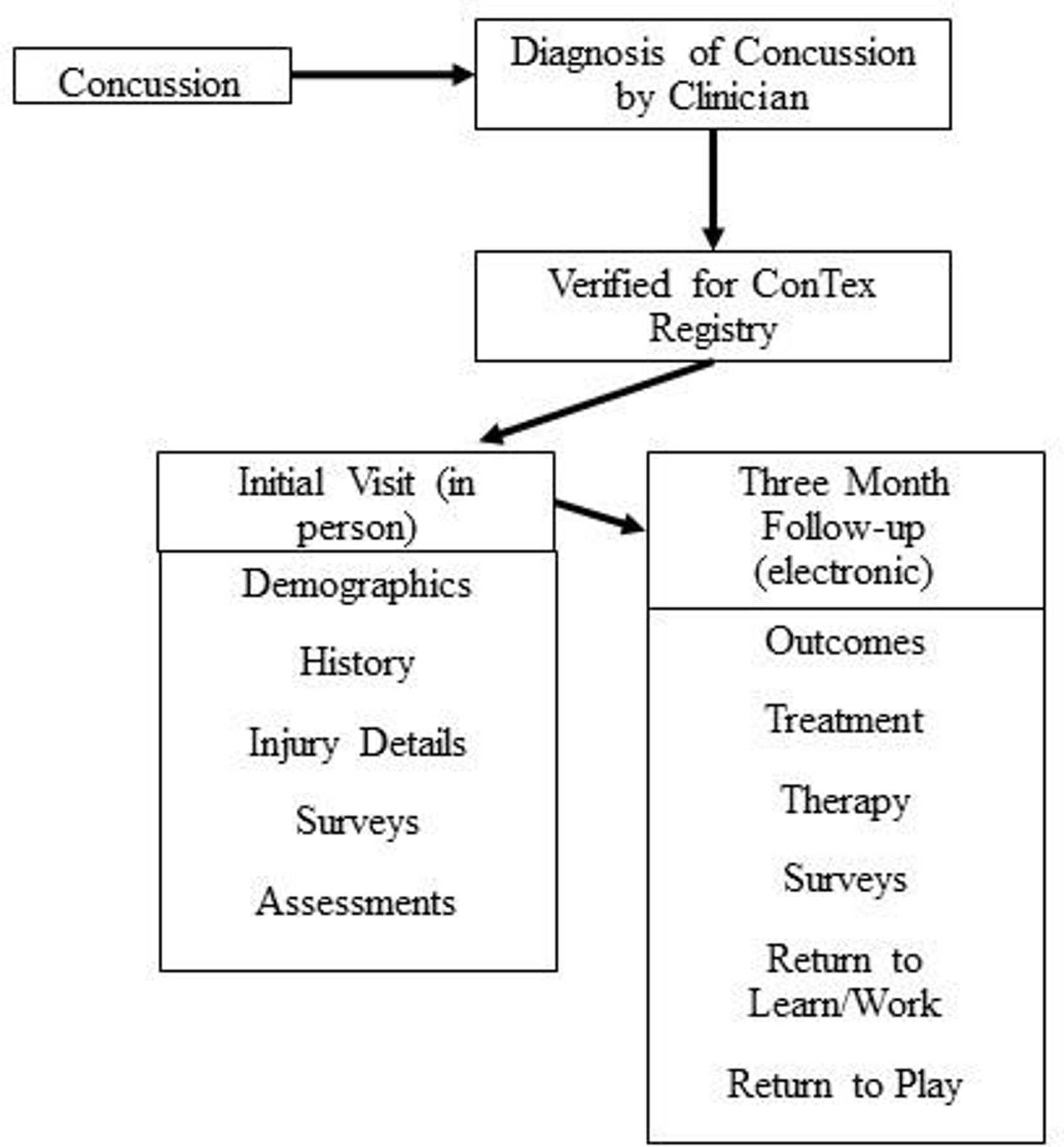
ConTex was designed as a flexible data collection platform, allowing for special projects as they develop while maintaining core variable collection. ConTex uses Research Electronic Data Capture (REDCap),13 which provides a secure, HIPAA-compliant database with user-friendly data entry, error checking capabilities and allows exporting for statistical analysis. Each ConTex site maintains necessary identifiers to ensure quality and proper follow-up in accordance with IRB policy. Study personnel at each site enter data directly into REDCap from the electronic medical record and during an in-person semi-structured interview with participants to ensure data uniformity and integrity. Data entered in the database are monitored by a Data Specialist using a REDCap data quality control module that reports missing values, validation errors and outliers. The ConTex Scientific Review Committee, consisting of co-investigators and coordinators, monitors projects, manages changes in study procedures and authorises research proposals and data access. Figure 1 provides an overview of the flow of ConTex data.

TheNorth Texas Concussion Registry (ConTex) data flow.
ConTex variables
Table 2 provides a summary of the core measures being uniformly collected across ConTex sites by trained research coordinators under the supervision of site principal investigators.
Primary ConTex measures
Each ConTex clinic collects a core set of measures: the Concussion Symptom Log (a subset of the Sport Concussion Assessment Tool or SCAT5/ChildSCAT5, depending on subject age) to record symptoms,14 the Generalised Anxiety Disorder 7-item Scale to assess anxiety symptoms,15 16 Patient Health Questionnaire-8 (PHQ-8) to assess depressive symptoms17 and the Pittsburgh Sleep Quality Index to assess sleep quality over the past month18 because sleep disturbance is common following concussion.19 Approximately 92% of participants have completed all core measures.
As part of each clinic’s routine concussion assessment procedure, balance is tested by one of three measures: the Balance Error Scoring System (BESS), an observer-scored balance test commonly used to assess SRC20; the shortened version of the BESS, the Modified Balance Error Scoring System (mBESS)21 or the Sway Balance test, which objectively measures balance using a computer tablet or smartphone and has a strong correlation with the BESS (r=−0.77), and has demonstrated good test–retest reliability.22 23
As a flexible data collection platform, ConTex can collect a wide range of measures that may be used in individual participating clinics at the discretion of the site principal investigators. These additional assessments vary across sites and may vary over time, but ConTex collects the data when available. Neurocognitive functioning is assessed in some of the ConTex clinics using the Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT), a computer-administered battery of cognitive ability tests.24 When available, subjects’ baseline and postinjury ImPACT data are collected. Visual processing/attention is assessed at some ConTex sites with the King-Devick test, a brief timed measure of visual tracking.25 26 The Brief Resilience Scale is used to measure an individual’s self-reported resistance and response to various health or injury-related setbacks.27 28 The Standardised Assessment of Cognition,14 another portion of the SCAT5, is also sometimes used to assess an injured athlete’s mental status. Lastly, the Acute Concussion Evaluation29 is also used in the evaluation of injury at some clinics.
Results from neuroimaging and other diagnostic procedures are also collected and added to the ConTex database when available in order to facilitate the development of pilot data for research projects. Likewise, investigators may propose the addition of specialised assessments or data collection tools for specific research questions or pilot data. If approved by the Steering Committee, those measures will be included for a specified time point or for a specified number of subjects, with findings reviewed by the group to see if there is interest in continuing those measures. Annually, all assessment tools included in ConTex are reviewed and a consensus of investigators determines whether various instruments will be dropped or added to the protocol.
Patient and public involvement
ConTex was designed by the multidisciplinary research team without patient or public involvement nor were patients invited to contribute to the writing of this document.
Findings to date
As of May 2019, 1701 subjects have been enrolled in the ConTex registry. Since we began keeping screening statistics in May 2018, 43% of all patients seen in ConTex clinics with suspected concussions were enrolled. Of those who were not enrolled, 38% did not meet inclusion criteria (of those excluded, 58% were seen >6 months postinjury, 17% had a more serious TBI, 12% were determined in clinic to not have a diagnosis of concussion and 6% were not fluent in English).
Of the 1701 subjects enrolled since the beginning of ConTex in 2015, there were approximately equal percentages of female (52%) and male subjects (48%), a mean age of 17.5 years and median age of 15 years (range 5–88) (figure 2). Subjects between ages 12 and 18 comprised 70% of all participants. The ethnic makeup of subjects was 82% non-Hispanic and 18% Hispanic. Regardless of ethnicity, almost 80% of subjects identified as white, and those identifying as black or African-American comprised the second largest racial group at nearly 15%. High school students comprised the largest group of ConTex subjects (47%), with middle school students (24%) as the second largest group. Nineteen per cent of ConTex subjects were college graduates.

{kind=link}
{kind=link}
The North Texas Concussion Registry concussions by age.
Thus far, SRCs account for 60% of all concussions recorded (table 3), with most occurring in tackle football (27%) and soccer (22%), followed by basketball (13%), volleyball (7%), cheerleading (4%) and softball (3%). Among non-SRCs, motor vehicle accidents, falls and hitting/being hit with an object accounted for the most concussions.
Mechanism of injury
A primary goal of ConTex is to collect quality data at subjects’ initial clinical visit and again at a 3-month follow-up to capture information regarding recovery. The median time from injury to enrolment was 6 days, with 71% of initial evaluations occurring within 30 days of injury. A majority of subjects (63%) are referred to a ConTex clinic from either emergency personnel or an athletic trainer that provided a preliminary assessment prior to the ConTex clinical evaluation (see table 4 for a list of primary provider types referring patients to ConTex). Of those eligible for follow-up (ie, subjects that are 3 months postinitial ConTex visit), the completion rate was 86%. By that time, 81% of these subjects reported feeling ‘back to normal’, which is consistent with general concussion recovery statistics.30
Providers of initial concussion assessment
Discussion
Recent increases in concussion awareness have led to a substantial increase in concussion research worldwide. Although much has been learnt, a number of important questions remain unanswered, and work in this area is in its early stages. SRC, in particular, has gained attention in recent years with a general focus being on football and male sports. Knowledge gaps exist concerning presenting features, risk and recovery factors and differences in treatment and recovery patterns in females and across various age ranges and types of injuries. ConTex is broad in its enrolment, with the goal of obtaining a balanced assessment regardless of sex, age, injury mechanisms and pre-existing factors. This inclusive enrolment strategy helps to elucidate factors that may influence early identification of specific premorbid and comorbid factors that characterise individuals who may be at increased risk for prolonged symptoms. This growing data bank from over 1700 subjects begins to allow for sufficient sample sizes to engage in quality data analysis, which may lead to a better understanding of how to identify key symptoms, risk factors and improve recovery and likelihood that patients return to baseline.
Several manuscript workgroups within the ConTex research team include premorbid risk factors, psychological factors in symptom maintenance, headache, sex differences,31 sleep32 and models for recovery prediction following SRC. A future goal of ConTex is to establish an effective framework for studies aiming to evaluate assessment, surveillance and treatment of concussion as well as the critical evaluation of diagnostic technologies as they are developed to advance the field of concussion research. Another future goal is to improve the specificity of symptom diagnoses within the dataset. For example, this includes efforts to further categorise ‘headache’ into specific phenotypes (ie, migraine, tension-type, etc), to identify specific causes for impaired sleep quality (ie, central sleep apnoea, obstructive sleep apnoea, iatrogenic causes, etc), and to better characterise risk and recovery factors related to premorbid personality, psychological status and resilience.
ConTex may serve as a model for other local, statewide and national concussion studies in order to aid in the understanding of concussion, its frequency and risk and recovery factors across a wide age range and multiple mechanisms of injury. An important outgrowth of ConTex has been the development and implementation of a statewide concussion registry for public schools through a collaboration between the University of Texas Southwestern Medical Center and the governing body of public school athletics in Texas, the University Interscholastic League, which will be described in a separate report.
Strengths and limitations
Other large prospective sports injury databases exist10 11; however, few focus specifically on concussion and capture detailed concussion and recovery characteristics in both sexes across the lifespan over time. ConTex is also unique in that the team has established an easy-to-use database, common data collection procedures, a proactive research oversight team and dedicated workgroups with special interests in various aspects of concussion and recovery.
Despite a roughly even balance of males and females, our ethnic/racial representation is currently limited. According to 2018 population estimates, 29% of the North Texas area was identified as Hispanic,33 although only 18% of those enrolled in ConTex were identified as Hispanic. This may reflect the geographic locations of ConTex clinics as only 25 subjects were excluded due to non-fluency in English (a requirement since most of the standard questionnaires have not yet been validated in Spanish). Other factors that may limit ConTex diversity include location of our clinics, community concussion awareness and regional interests in research participation. ConTex investigators are attempting to address these limitations through the translation of assessment materials and raising concussion awareness through outreach events in the community via health fairs and school presentations.
Similarly, there may be a sampling bias to ConTex data at this point. While most participants were evaluated within 2 weeks of concussion, 30% presented >30 days after injury and >250 potential subjects were excluded due to their injuries occurring >6 months prior. The current ConTex clinical providers represent specialists and tertiary care providers, and as such, patients often present in the subacute or chronic phase of injury. This population is more likely to still be experiencing symptoms and may disproportionally represent those with prolonged recovery. While this might be a limitation of the overall data to date, it affords a unique opportunity to examine the characteristics of specific cohorts within our larger dataset, that is, those who have persistent symptoms, which is a group in need of particular research attention since less is known about this sizeable minority of concussed individuals.
Although many symptom measures such as those used in ConTex are based on self-report and cannot be externally validated, they are globally accepted and widely used tools for research and clinical application. We did not include specific symptom validity measures, but participants had no obvious motivation to deny or enhance symptom reporting as they had already received a clinical diagnosis of concussion prior to data collection, and all were recruited for ConTex as a part of routine clinic visits. It is through future research efforts such as those afforded by ConTex that less reliance on subjective assessment of concussions such as self-reporting and more reliance on objective measures for assessment of concussion can be developed and validated.
ConTex is an interdisciplinary, multi-institutional project, representing the combined efforts of doctoral-level scientist-practitioners in the areas of neurology, physical medicine and rehabilitation, neuropsychology, neurosurgery and sports medicine from four Dallas-area academically affiliated concussion clinics. Collection of data from multiple sites, by clinicians with varied backgrounds could present limitations to reliability and generalisability, although ConTex has addressed this by use of common definitions and procedures agreed on by site leaders with regular review and monitoring of procedures and data for quality control. ConTex clinicians adhere to a consensus-based multimodal approach to the evaluation and treatment of concussions.12 34 This approach allows ConTex to replicate the ‘real world’ of clinical practice.
Collaboration
ConTex findings are disseminated at scientific conferences, local lectures and through peer-reviewed journals. The database provides an investigative repository for ConTex investigators for analyses. There are no plans to disseminate ConTex data to study participants per se outside the aforementioned scientific outlets.
References
Footnotes
Twitter @Munro_CullumPhD, @StephenCBunt, @DidehbaniNyaz
Collaborators ConTex collaborators include: (1) Texas Scottish Rite Hospital: Shane Miller MD, Jane Chung MD, Aaron Zynda BS CCRP, Megan Sabatino BS, CCRP; (2) Children's Medical Center: Tonia Sabo MD, Marsha Siebenmorgen PhD, Mathew Stokes MD; (3) UT Southwestern Medical Center: C. Munro Cullum PhD, Hunt Batjer MD, Kathleen Bell MD, Bert Vargas MD, Nyaz Didehbani PhD, Heidi Rossetti PhD, Mark Goldberg MD, Chris Paliotta MBA, Linda Hynan PhD, Charlene Supnet PhD, Bruce Jones PhD, Stephen Bunt EdD, Elida Godbey MRC, Cason Hicks MS, Sarah Sprinkle MA, Doris Escobedo MS, Caryn Harper MS, Nasreen Sayed MS, Tahnae Tarkenton MCRC.
Contributors MC is the Principal Investigator for the ConTex study. SM, BV, TS, KB and HHB are Co-investigators and clinical directors at ConTex clinics. SB and CH are ConTex Research Coordinators. MC, SB, CH, ND, SM, BV, TS, KB and HHB developed the ConTex protocol and study design. MC, SB and CH drafted the initial manuscript. SB and CH were responsible for data collection and analysis. All authors provided input on reporting of initial study findings. All authors participated in revision and gave approval of the published version.
Funding This prospective registry was funded by a grant from the Texas Institute for Brain Injury and Repair (TIBIR), a state-funded initiative as part of the Peter J. O’Donnell Jr. Brain Institute at The University of Texas Southwestern Medical Center.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the UT Southwestern Institutional Review Board (STU 012015-032) and the Texas Health Resources Institutional Review Board (Pro00006054).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are not publicly available at this time.