Article Text

Abstract
Aims This cross-sectional study aimed to assess resilience, professional quality of life and coping mechanisms in UK doctors. It also aimed to assess the impact of demographic variables, such as sex, grade and specialty on these factors.
Methods During October and November 2018, medical doctors in the UK were eligible to complete an online survey made up of validated psychological instruments. Royal Colleges and other medical organisations invited their membership to participate via newsletters, email invitations, websites and social media.
Results 1651 doctors participated from a wide range of specialties and grades across the UK. The mean resilience score was 65.01 (SD 12.3), lower than population norms. Of those who responded, 31.5% had high burnout (BO), 26.2% had high secondary traumatic stress and 30.7% had low compassion satisfaction (CS). Doctors who responded from emergency medicine were more burned out than any other specialty group (F=2.62, p=0.001, df 14). Those who responded from general practice scored lowest for CS (F=6.43, p<0.001, df 14). 120 (8%) doctors met the criteria for all three of high BO, high STS and low CS. The most frequently reported coping mechanism was the maladaptive strategy of self-distraction.
Conclusions One-third of UK doctors who responded are burned out and suffering from STS. Those who responded from emergency medicine and general practice appear to be suffering the most. Over 100 doctors fell into the at-risk category of high BO, high STS and low CS. Future analysis of the free text responses from doctors may help to identify factors that are playing a role in the high levels of BO and STS being reported by medical staff.
- resilience
- burnout
- doctor
- physician
- clinician
- psychological well-being
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the largest published study of its kind with a considerable number of participants from a wide range of grades and specialities across the UK.
This is the first time resilience and these other psychological factors have been assessed in combination with National Health Service medical staff across the UK.
The scores for the individual psychological tests are generally consistent across all four countries in the UK.
Doctors self-selected to participate, making the study subject to selection and response biases.
A cross-sectional study of this kind can only imply association, not causation.
Introduction
A career as a doctor can be incredibly rewarding, but it can also be challenging.
Doctors are known to be at higher risk of anxiety, depression, substance abuse and suicide when compared with the wider population.1 2 The nature of their work can mean exposure to high-pressured environments resulting in high levels of stress. These factors, in addition to a heavy workload and long working hours, can have an adverse effect on both physical and mental well-being.3 4 Furthermore, the complexity of doctor–patient relationship can introduce a wide variety of both positive and negative emotions for doctors. A finite budget, administrative constraints and the perceived litigious climate faced by doctors are also undoubtedly contributory factors to the increasing levels of burnout (BO) being reported by medical staff.5–7
BO can be defined as exhaustion of physical or emotional strength or motivation usually as a result of prolonged stress or frustration.8 9 It is a noteworthy issue among medical staff globally.6 7 Aside from the implications for an individual doctor’s mental well-being, BO has an impact on healthcare systems, such as the UK National Health Service (NHS). Concerns over the mental-ill health of people working in the NHS have been highlighted by the British Medical Association (BMA) and in journals such as T he Lancet.6 7 In 2017, the BMA declared that the mental-ill health of NHS staff is a major healthcare issue, leading to presenteeism (the practice of going to work despite illness or anxiety, which often results in reduced productivity), absenteeism and loss of staff from the workforce.6
Psychological resilience is difficult to conceptualise and define, but it is generally accepted as the ability to recover from significant stress or adversity. The literature contains a wide range of resilience scores for physicians, with most studies into resilience in medical doctors undertaken in Australian and American healthcare systems.10–15 These studies have highlighted the complex, multifactorial nature of resilience.16 Factors influencing a doctor’s resilience include personality factors, organisational factors, social support (both from colleagues and on a personal level), interests outside of medicine and overcoming previous adversity.16
Consequently, the concept of resilience among doctors in the UK has gained increasing importance since the General Medical Council introduced resilience training to the medical school curriculum in 2014.17 Despite this, limited information exists on resilience in NHS doctors. A pilot study in a single NHS trust in Northern Ireland in 2016 demonstrated that workplace and systemic factors seemed to play a role in low resilience.18 It found that doctors were using maladaptive coping mechanisms to manage stress and when compared with the wider population, they had higher levels of BO and secondary traumatic stress (STS). However, there was a lack of information on whether or not these findings are applicable to doctors working elsewhere in the UK. The national study reported here fills this gap. It aimed to investigate resilience, stress, BO and coping in doctors across the UK. It also aimed to determine the impact of demographic variables, such as sex, grade and specialty on these factors. Finally, it aimed to assess the factors most strongly related to BO in UK doctors. As far as we are aware, it is the first study to report on these factors in the UK medical workforce.
Methods
During October and November 2018, all medical doctors working in the UK were eligible to complete an online survey made up of validated psychological instruments. The survey was created using online survey software, SurveyMonkey. Royal Colleges and other medical organisations invited their members to take part using the hyperlink to the survey that was advertised in newsletters, email invitation, websites and on social media (online supplementary appendix 1). Promoting the survey in this way meant that an unknown number of potential participants were invited to take part in the study. Doctors self-selected to participate and responses were anonymous. Participants were asked to complete the online questionnaire once and only if they were a medical doctor currently working within the UK.
Supplemental material
The online survey began with a brief introduction following which participants were asked to confirm that they consented to taking part in the study by selecting ‘Yes’, from a drop-down menu. The survey, which had been successfully piloted within a single NHS trust in 2016,18 consisted of a 90-item questionnaire made up of a selection of demographic questions and three empirically validated instruments. These self-reported, validated instruments ask the participant to consider a statement and then rank themselves appropriately on a Likert scale (eg, not true at all (0), rarely true (1), sometimes true (2), often true (3) and true nearly all of the time (4)).
Resilience was measured using the Connor Davidson Resilience Scale (CD-RISC).19 This is a 25-item test that yields a score between 0 and 100. Higher scores indicate higher resilience. There is no population norm score for this instrument, but the CD-RISC manual includes tables of mean CD-RISC scores compiled from published studies worldwide. It has been demonstrated to be a reliable and valid measure in assessing resilience.20 In a review of validated resilience measurement instruments, Windle et al assessed the quality of 15 resilience scales. Overall, the CD-RISC received the highest ratings and scored highest on the total quality assessment.20
Professional quality of life was measured using the Professional Quality of Life Scale (ProQOL V).21 This 30-item questionnaire is composed of three subscales and aims to measure the positive and negative effects of helping others and as a result it is specifically tailored to healthcare professionals. The first subscale is BO; feelings of anger, exhaustion or frustration related to work. The second is STS; fear and negative feelings derived from work-related trauma. The third subscale is compassion satisfaction (CS); the pleasure an individual derives from being able to help others and from doing their work well. Each subscale is scored out of 50 and can be compared with a sample of normative data in the ProQOL manual.21 The population mean score for BO is 20, STS is 11 and CS is 37. Additionally, each component can be transformed to a t-score and then divided into low (≤43), moderate (44–56) or high (≥57) to facilitate interpretation of scores.
Finally, the 28-item BRIEF COPE scale measures 14 different dimensions of coping. It assesses a broad range of coping responses (self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioural disengagement, venting, positive reframing, planning, humour, acceptance, religion and self-blame), asking two questions for each dimension in order to increase reliability.22 Each coping strategy is scored from 2 to 8 with higher scores reflecting more frequent use of the strategy. Coping mechanisms can be classified as adaptive or maladaptive.
Data were analysed using SPSS V.25 (IBM Corp). Only fully completed instruments were included in the analysis. The assumption of normality was assessed visually. Differences between country, specialty, number of years since graduation and grade were analysed using a one-way analysis of variance. The differences between gender and the specialty groups were analysed using independent samples t-test. Linear regression was used to analyse the relationship between BO (as an outcome variable) and the remaining variables (as covariates) using backward elimination.
Results
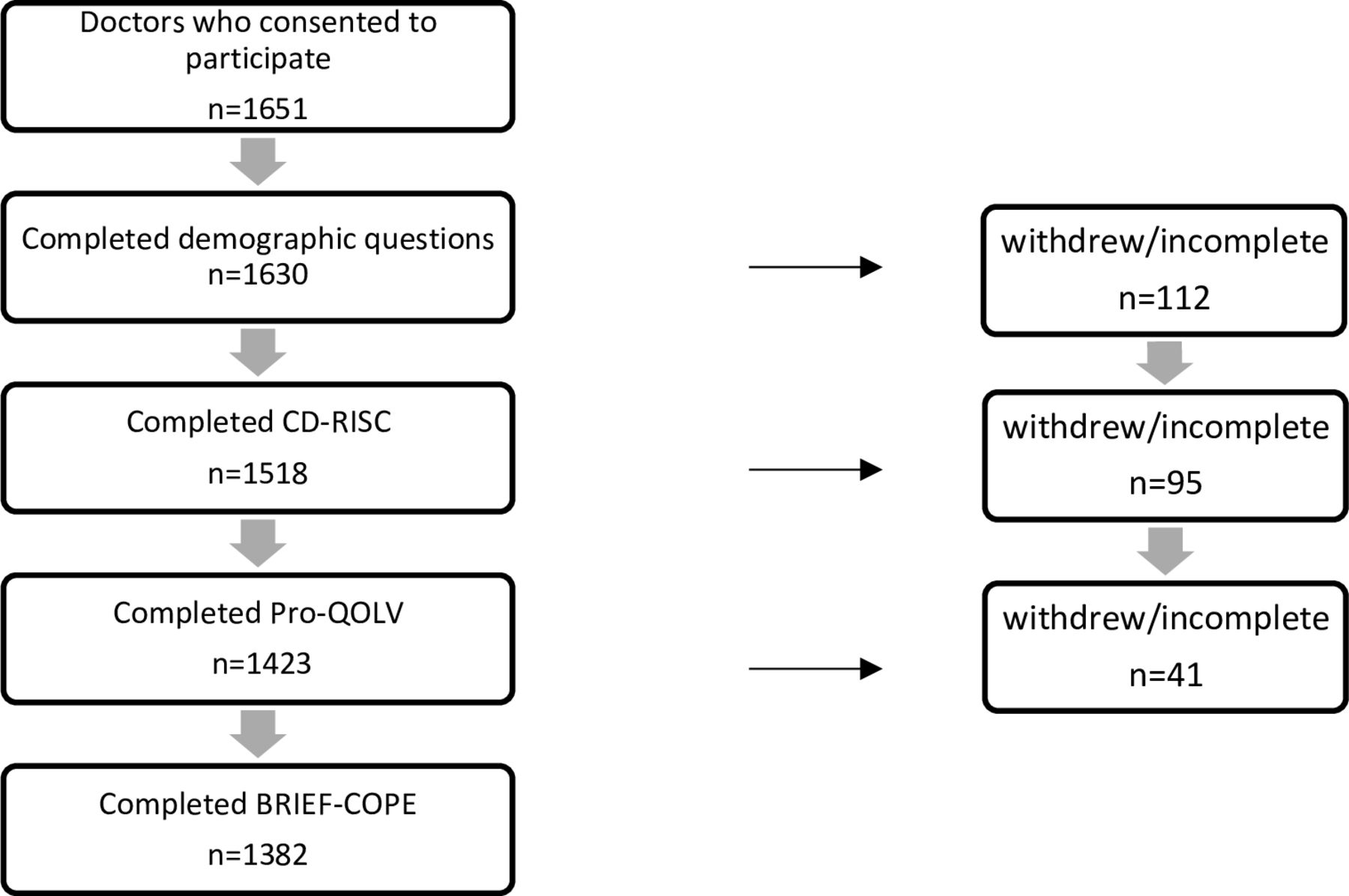
Surveys were completed by 1651 doctors (1305 women, 331 men and 15 who preferred not to say their gender or did not respond to this question) from a wide range of specialties and grades across the UK (tables 1–3). The methods used to promote the survey mean that an unknown number of potential participants were invited to take part in the study and therefore a response rate cannot be calculated. Survey software estimated that the average time to complete the questionnaire was 8 min. Figure 1 shows the withdrawal of participants or the number of incomplete psychological tests through the survey.

{kind=link}
Withdrawal of participants or number of incomplete psychological tests through the survey. Demographic questions gave participants the option of, ‘I’d prefer not to say’. The number of participants choosing this option ranged from 5 to 20 for each individual question. Given these small numbers, participants who chose this option are omitted from the demographic analysis. CD-RISC, Connor Davidson resilience scale. ProQOL V, Professional Quality of Life Scale.
Number of participants by speciality and resilience score on CD-RISC (mean, SD)*
Number of participants by grade and resilience score on CD-RISC (mean, SD)*
Number of participants by country and resilience score on CD-RISC (mean, SD)*
Resilience was measured in 1518 doctors. The mean resilience score was 65.0 (SD 12.4). Although no population norm score exists for the CD-RISC, other published UK studies have found higher mean CD-RISC scores,23 24 suggesting lower resilience in this cohort of doctors.
There was no significant difference between male and female resilience scores among the respondents in our survey (men 66.4, women 64.6) (t=2.06, p=0.05, df 410). However, in this cohort, hospital-based doctors scored higher for resilience than general practitioners (GP) (t=−3.64, p<0.001, df 911). Surgical specialities scored higher than non-surgical specialities (t=4.22, p<0.001, df 331). Foundation doctors and specialty and associate specialist (SAS) grade doctors had lower resilience scores than core trainees, specialty trainees and consultants (F=3.71, p=0.002, df 5).
Doctors working in Northern Ireland responding to the survey scored higher for resilience than those working in England, Scotland and Wales (F=7.92, p<0.001, df 4). Notably, the resilience score for Northern Ireland was similar to the CD-RISC score obtained in the pilot study in a single healthcare trust in Northern Ireland in August 2016.18
Professional quality of life was measured in 1423 doctors. Mean BO was 28.1 (SD 6.0) (population mean score 20). Mean STS was 23.7 (SD 5.8) (population mean score 11). Mean CS was 35.4 (SD 6.6) (population mean score 37). Tables 4–6 display the means and SD of the ProQOL V subscales for each specialty, country and group of doctors.
ProQOL V subscale scores by speciality (mean, SD)*
ProQOL V subscale scores by country (mean, SD)*
ProQOL V subscale scores by group (mean, SD)*
BO and STS scores in this cohort were significantly higher than the normative sample scores in the ProQOL manual and higher than other published studies of medical staff (mean BO 28, population mean BO 20) (mean STS 23, population mean STS 11) (t=50.99, p<0.001, df 1416) (t=81.96, p<0.001, df 1422).21 25–27 Doctors’ CS scores were comparable with the normative sample score (mean CS 35, population mean CS 37).20
Among the respondents, BO scores were generally consistent for men and women, country, different grades of doctor and the number of years since graduating as a medical doctor. However, those doctors who responded from emergency medicine were more burned out than other specialty groups (F=2.62, p=0.001, df 14). In addition to being more burned out, they also scored higher than any other group of physicians for STS. Foundation doctors and SAS grade doctors also had higher mean STS scores than other grades of doctor (F=7.39, p<0.001, df 5).
General practice scored lower for CS than other specialty groups (F=6.43, p<0.001, df 14). When surgical specialities were compared with non-surgical specialities, surgeons scored higher for CS than non-surgical colleagues (t=4.82, p<0.001, df 1420).
When characterised into low, medium and high BO, 31.5% of doctors had high BO with 24.8% having low BO scores. Of note, 26.2% had high STS and 30.7% had low CS. For clinicians to be functioning well in their vocational role, ideally, they would score low for BO, low for STS and high for CS.21 Only 87 (6%) clinicians fell into this desired group. Conversely, 120 (8%) doctors met the criteria for high BO, high STS and low CS.
Coping mechanisms were measured in 1382 doctors. Each coping strategy is scored from 2 to 8 with higher scores reflecting more frequent use of the strategy. Coping strategies are classified as adaptive or maladaptive. Table 7 displays the means and SD for the 14 coping mechanisms that were assessed.
Mean score for each coping mechanism on brief cope scale (mean, SD)*
The coping mechanism most frequently reported by this cohort was the maladaptive strategy of self-distraction (drawing one’s thoughts or attention away from the problem or stressor). Commonly reported adaptive coping strategies were active planning (thinking about how to confront the stressor) and emotional support (seeking reassurance, acceptance and encouragement at a time of stress). Another maladaptive strategy, self-blame (placing undeserved blame on oneself based on character or actions), was also frequently used.
Reported use of coping strategies was generally consistent across country, specialty and grade. However, surgeons in this study were significantly less likely to use self-distraction as a coping mechanism than non-surgical colleagues. Doctors working in Northern Ireland were significantly more likely to employ religion as a coping mechanism than doctors working in other parts of UK. Men who responded used the maladaptive coping strategy of substance use more commonly (eg, I’ve been using alcohol or other drugs (a medium amount or a lot) to make myself feel better), but this was infrequently reported. Men were also significantly more likely to use denial and humour to cope whereas women more frequently used emotional support, instrumental support and positive reframing.
Regression analysis
A linear regression model was used to investigate potentially predictive factors for the development of BO. CS, STS and resilience were important co-variates in the model. Maladaptive coping strategies, behavioural disengagement, substance abuse and venting also made significant contributions to the development of BO. The final coefficients are presented in table 8.
Final coefficients of linear regression model analysing the relationship between BO (as an outcome variable) and the remaining variables (as covariates) using backward elimination*
Discussion
This study demonstrates that one-third of UK doctors who responded to the survey demonstrate BO and are suffering from STS. Similar to other published studies worldwide, in this cohort, doctors are primarily using maladaptive coping strategies to manage work-related stress.28 However, of particular concern might be the finding that 120 (8%) of responding doctors scored high for BO, high for STS and low for CS. This is important to acknowledge as the developers of the ProQOL V scale would suggest that these doctors may be suffering from clinical depression and would benefit from treatment, time off work or even changing their job.21
The respondents in this study had a mean CD-RISC score of 65.0 (SD 12.4) scoring lower for resilience than participants of other published UK studies from different populations.23 24 For example, in a study of 1534 English university entrants the mean CD-RISC score was 75.1 (SD 12.8).23 In another UK-based study of parents of children with cleft-lip and palate, the mean CD-RISC score was 72.0 (SD 13.5).24 As demonstrated elsewhere, resilience does appear to be a protective factor for BO being an important covariant in the regression model in this study.10 However, it is not clear if resilience is really what is required of doctors to prevent exhaustion and frustration, the characteristics of BO. In other published studies of medical staff, some physicians still exhibited evidence of BO despite high levels of resilience.12 14
The results of this study suggest specific groups of doctors who are most fatigued and rate their professional quality of life lowest. Unsurprisingly, it includes the respondent doctors who are working at what has been described as the ‘NHS Frontline’, namely in general practice and emergency medicine. They are often working under pressure due to the nature and number of patients, time constraints and understaffing.29 30 Our findings have suggested that the respondent doctors in these specialities are the most exhausted, stressed and compassion fatigued. This is supported by other published studies of medical staff worldwide.1 31 The Shanafelt et al study of 7288 US physicians identified a substantial difference in BO rates by specialty, with those doctors working at the front line of care access having the highest rates of BO.1 More recently, the Medscape National Physician Burnout, Depression and Suicide Report 2019 confirmed that doctors working in emergency medicine and family medicine were among the most BO. In light of similar findings in this study of UK doctors, interventions to improve doctors’ professional quality of life might be best placed if it were possible to specifically target interventions to those doctors most at risk.
There are limitations to this study. Primarily, the fact that doctors self-selected to participate makes the study subject to selection and response biases. Also, a response rate cannot be calculated due to the methods used to promote the survey. Given the sample size, even small differences in scores on the psychological tests can be statistically significant. Two countries (Wales and Scotland) are under-represented, and a preponderance of female doctors responded, which is typical of online survey participation.32 However, the scores for the individual psychological tests are generally consistent in men and women and across all four countries in the UK. It is also important to remember that a cross-sectional study of this kind can imply only association, not causation. Its observational nature means that these findings are only representative of the subset of UK doctors who chose to respond, at a specific point in time. However, it is the largest published study of its kind with a considerable number of participants from a wide range of grades and specialities across the UK. It is also the first time resilience and these other psychological factors have been assessed in combination NHS medical staff across the UK.
Future analysis of the free text response section of this survey that is not reported here may help identify factors that are playing a role in the high levels of BO and STS being reported by this cohort. The information gleaned from these responses may be useful in guiding interventions to improve the psychological well-being of the NHS medical workforce. An evidence-based psychological intervention, such as a self-care skills training programme, that has been shown to improve professional quality of life in similar populations, may benefit UK doctors.33 However, it has been demonstrated elsewhere that organisational contexts influence resilience, work engagement and professional quality of life in medical staff.10–16 31 Individual physician well-being and healthcare system well-being may be better addressed by acknowledging and improving modifiable organisational factors within the NHS such as workload, working environment, social support and degrees of clinical freedom within the workplace.
Finally, although well intended, it is unlikely that solely addressing emotional resilience will improve doctors’ professional quality of life. In fact, it can be argued that the concept of resilience training simply places additional responsibility for good mental health onto doctors themselves.34 Doctors cannot be expected to recover from the emotional stress and adversity they encounter in their role as clinicians while managing a heavy workload in an under-funded, over-worked system. It is unlikely that emotional resilience is all that is required to cope with increasing regulation, litigation and administration.
Conclusion
One-third of UK doctors who responded demonstrate BO and are suffering from STS. Of note, 120 (8%) responding doctors fell into the at-risk category of high BO, high STS and low CS. However, the question remains, would UK doctors benefit from an evidence-based psychological intervention to improve professional quality of life? Or would physician well-being be better addressed by acknowledging and improving workplace factors? Analysis of the free text responses from the survey may answer this question and help to guide any future intervention to improve doctors’ well-being. Finally, it could be argued that if the NHS is to continue to remain among the highest-rated healthcare systems globally,35 ensuring the psychological well-being of its doctors should be seen as a matter of national importance.
Main messages
Doctors scored lower for resilience than other published UK studies.
Respondent doctors had higher levels of burnout and secondary traumatic stress than the population norm and other studies of medical staff.
Doctors are most commonly using maladaptive coping strategies.
Current research questions
Although resilience may be protective against burnout, is emotional resilience really what is required of doctors to prevent exhaustion and frustration?
Would an evidence-based psychological intervention improve professional quality of life for UK doctors?
Would physician well-being be better addressed by acknowledging and improving modifiable workplace factors?
References
Supplementary materials
- Press Release -
Press Release
- Press Release -
Footnotes
Contributors NM and RSM contributed equally to this study and can be considered joint first authors. NM designed the study, designed data collection tools, monitored data collection, cleaned and analysed the data and drafted and revised the paper. RSM designed the study, designed data collection tools and revised the paper. LC monitored data collection, analysed the data and drafted and revised the paper. MD designed the study, analysed the data and revised the draft paper. MC monitored data collection, analysed the data and revised the paper. WJC designed the study, analysed the data and revised the paper. SJK designed the study, monitored data collection, analysed the data and revised the paper.
Funding The authors would like to acknowledge the Innovation, Research and Development Office within the South Eastern Health and Social Care Trust who granted the article processing charge (APC) for this open access publication.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approval was granted from the South Eastern Health and Social Care Trust NHS Research Governance Committee (SET17.55) and ethical approval was granted by Queens University Belfast, School of Medicine, Dentistry and Biomedical Sciences, Ethics Committee (Ref 18.40).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.