Article Text

Abstract
Objectives This study aimed at opening the black box of the relationship between leadership and motivation of health workers by focusing on a high-performance hospital in Morocco.
Design We adopted the realist evaluation approach and used the case study design to test the initial programme theory we formulated on the basis of a scoping review on complex leadership. We used the Intervention-Context-Actors-Mechanism-Outcome Configuration as a heuristic tool to identify plausible causal configurations.
Settings Since 2000, the Ministry of Health in Morocco initiated many reforms in the frame of the governmental deconcentration process called ‘advanced regionalisation’. The implementation of these reforms is hampered by inadequate human resource management capacities of local health system managers. Yet, the National ‘Concours Qualité’, a national quality assurance programme implemented since 2007, demonstrated that there are many islands of excellence. We explore how leadership may play a role in explaining these islands of excellence.
Participants We carried out a document review, 18 individual interviews and 3 group discussions (with doctors, administrators and nurses), and non-participant observations during a 2-week field visit in January–February 2018.
Results We confirmed that effective leaders adopt an appropriate mix of transactional, transformational and distributed leadership styles that fits the mission, goals, organisational culture and nature of tasks of the organisation and the individual characteristics of the personnel when organisational culture is conducive. Leadership effectiveness is conditioned by the degree of responsiveness to the basic psychological needs of autonomy, competence and relatedness, perceived organisational support and perceived supervisor support. Transactional and overcontrolling leadership behaviour decreased the satisfaction of the need for autonomy and mutual respect. By distributing leadership responsibilities, complex leaders create an enabling environment for collective efficacy and creative problem solving.
Conclusions We found indications that in the Moroccan context, well-performing hospitals could be characterised by a good fit between leadership styles, organisational characteristics and individual staff attributes.
- human resource management
- complex leadership
- motivation
- leadership
- low middle income countries
- Morocco
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study may contribute to fill the gaps in complex leadership studies by unveiling psychological processes, mechanisms and conditions through which leaders motivate health workers.
This study applies the realist evaluation (RE) approach to the study of leadership, which has been rarely done.
The Intervention-Context-Actors-Mechanisms-Outcome is a useful heuristic tool to identify plausible causal configurations.
Further research could focus on the role of responsiveness to basic psychological needs, trust, perceived organisational support and perceived supervisor support in explaining the motivation of staff and effectiveness of leadership in healthcare settings.
We acknowledge that our study findings might be affected by recall bias and temporality, commonly encountered in retrospective REs, and in any retrospective study in general.
Introduction
In many low-income and middle-income countries (LMICs), the performance of health workers is below expectations,1 leading to low quality of care2 and inadequate implementation of health policies.3 Leadership and organisational characteristics are recognised to play a major role in health workers’ performance.4 Unfortunately, leadership of public healthcare organisations in LMICs is often characterised as authoritarian and hierarchical, which reduces their effectiveness.3 5 6
Not surprisingly, scholars, policymakers and global health institutions are paying increased attention to the role of leadership in health workers’ performance in LMICs.3 7–14 However, the empirical evidence on leadership effectiveness in LMIC remains weak.15 16 The Alliance of Health Policy and System Research called for multidisciplinary research to explore the contribution of leadership in health systems,17 reinforcing the call by Rowe and colleagues for innovative research methodologies.1 17 In response, this paper aims at exploring the underlying processes that link leadership to health workers’ motivation, and the organisational characteristics and contextual conditions within which these processes are enabled or hindered.
Background
The Moroccan health system
Since 1997, the Moroccan government engaged in a general deconcentration process called ‘advanced regionalization’ (régionalisation avancée) through which administrative authority is decentralised to three subnational government levels: the region, the prefecture or the province and the municipality.18–20 In healthcare, the deconcentration was accompanied in 2000 by hospital reforms and the extension of universal health coverage (UHC).21 These reforms aimed at improving the quality of care through the implementation of quality assurance programmes and renewal of hospital infrastructure and equipment. It also aimed at strengthening hospital management capacity, and more specifically focused on accounting and financial management systems, strategic staffing frameworks, hospital management information systems, hospital development plans and decentralisation of human resources (HR) management functions.
The current structure of the health system in Morocco is presented in figure 1, which shows the healthcare networks, the links between the actors, and the interactions within and across regions, provinces and health districts.19 Managers at regional, provincial and district level oversee the operations of the health system within their respective well-described administrative areas. Besides being responsible for maintaining an optimal functioning of the health services, they play a key role in implementing health policies and adapting them to local contexts. They have administrative responsibilities with considerable discretion in decision-making, planning, monitoring and implementing regional health programme and UHC policies, budgetary and financial management, personal administration, coordination of health networks and partnership with local actors.22 However, they have limited discretion in personnel selection, recruitment, training and financial incentives.21

Element of the Moroccan health system.
Leadership in the health sector
Evidence indicates that in Morocco, lack of motivation, leadership and HR management capacity of local managers constrains the performance of healthcare organisations in terms of health service delivery, quality of care, effectiveness, efficiency, implementation of change and scaling up of proven effective interventions,23 24 but also the implementation of policies25–29 and quality assurance programmes.30–32 Yet, the data of the national Concours de qualité, a national quality assurance programme initiated in 2007,23 24 33 demonstrate that there are islands of excellence where leadership seems to play a key role.30 How leadership may play a role in explaining these islands of excellence remains unclear and this study aims at exploring this.
‘Traditional’ leadership theories, including transactional and transformational leadership, typically focus on leader–follower exchange relationships. Both theories are said to be oriented towards control and stability of the organisation. A promising recent development that fits dynamic situations better is complex leadership, which suggests that human societies are best considered to be organic systems that are characterised by uncertainty and unpredictability.34 Similarly, other authors consider healthcare organisations as complex adaptive systems.35–38 In such systems, traditional leadership approaches tend to fail to the extent that they do not stimulate staff members to develop adequate responses to uncertainty. Complex leadership theorists argue that in such situations, leaders should enable or empower the employees rather than direct them through command-and-control or transformational leadership practices. In effect, they stimulate sharing of information, provide effective support to lower-level cadres and distribute leadership. Complex leaders know when to use transactional, transformational or distributed leadership practices, and adapt their practices to the nature of the cadres and their task.39–41 A complex leadership approach is therefore called for when work processes are characterised by unplanned situations or emergent problems.
Complex leadership
Our scoping review of the complex leadership literature indicated that despite its potential, complex leadership has been little studied in the field of health in LMICs.39 It confirmed the multidimensional nature of leadership. We thus set out not to explore the effects of a single leadership style, but to see whether the complex leadership approach could explain our observations, starting from the hypothesis (or initial programme theory) we derived from the scoping review (see figure 2). We thus searched for transactional leadership, transformational leadership and team-centred leadership or distributed leadership practices in the settings of the study hospitals. In practice, the review led us to formulate the following hypothesis (or initial programme theory): “Public-oriented health care organizations that are well performing are likely to be characterized by a high congruence between leadership styles and practices, organisational characteristics and individual staff attributes. More specifically, managers adopt an appropriate mix of transactional, transformational and distributed leadership styles that fits the mission, goals, organisational culture, and nature of tasks of the organisation as well as the individual characteristics of the personnel in terms of age, gender, professional profile and motivation” (figure 2).
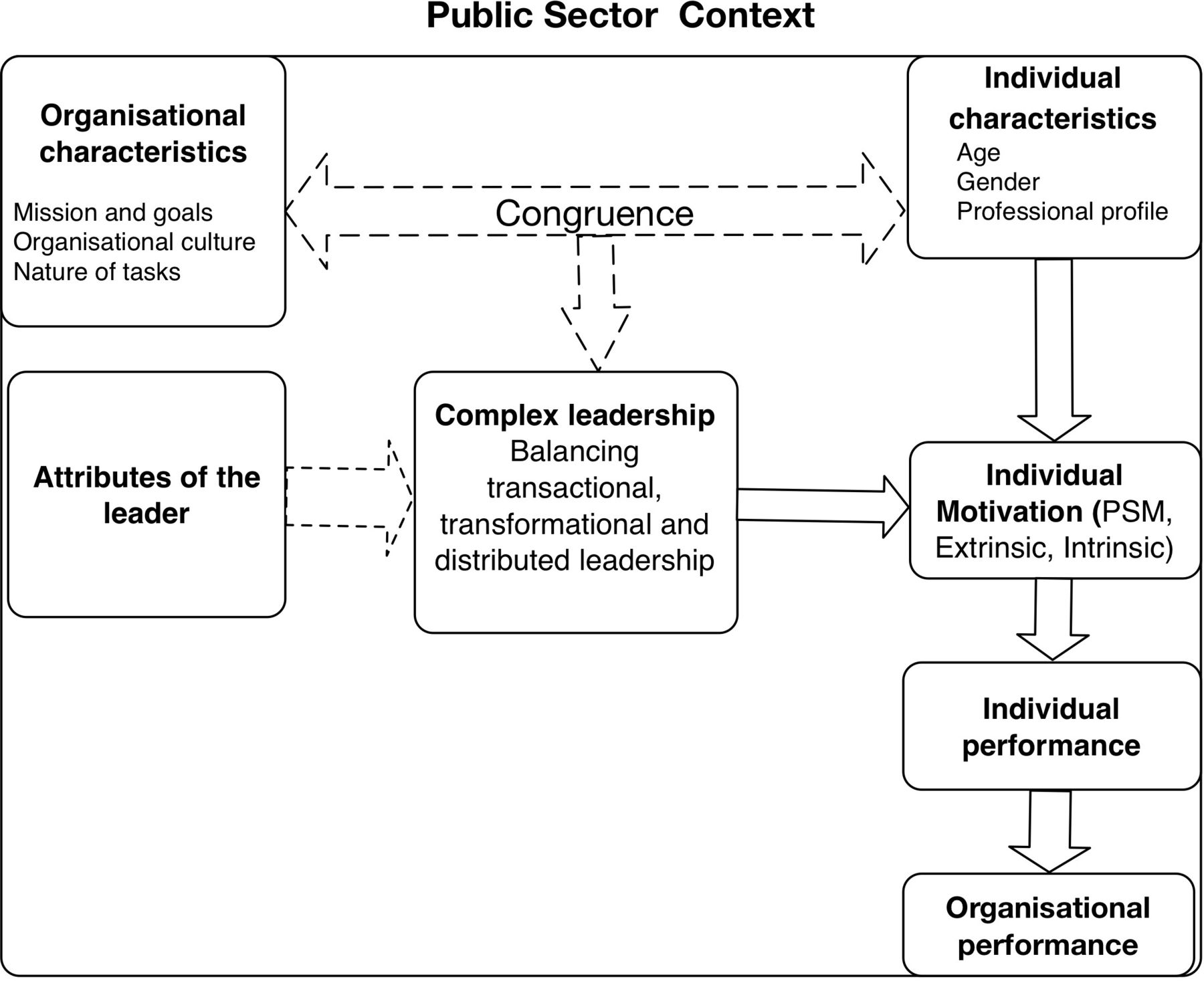
Initial programme theory. Arrow: effect; double-dotted arrow: degree of congruence (fit).
The relationships between leadership, motivation, performance and organisational culture are complex in nature.42 43 In this study, we look at leadership from a dynamic, multilevel perspective, which accepts that leadership is embedded within a social and organisational context (and thus culture).39 44–49 The organisational culture influences how leadership is interpreted, enacted and consequently shapes its effectiveness on staff motivation and behaviour.50–52 This web of relations is the subject of the larger PhD study, of which this paper is part, but it is outside the scope of this paper.
The mechanisms underlying the effect of leadership
From a realist perspective, mechanisms are understood as “the underlying processes or ‘hidden causal levers’’ that account for how and why a program works to bring about desired changes in the reasoning and behaviour of participants”.53
We adopt two perspectives on mechanisms. The first has its origins in the nature of commitment and focuses on perceived supervisor support (PSS) and perceived organisational support (POS), which have been shown to be important constructs or factors in the relationship between leadership and motivation and/or commitment.54–56 POS means the beliefs of staff about the extent to which the organisation (ie, the top management team) values their efforts and contribution, and their psychological well-being. PSS is similar but focuses on the relationship between supervisor and employee54 57 58 (see online supplementary file 1).
Supplemental material
The second perspective focuses on motivation and more specifically on the notion of basic psychological needs, which has been extensively developed within Self-Determination Theory (SDT). In short, the motivation of health workers is best considered as a continuum from extrinsic motivation to intrinsic motivation59 (figure 2). According to SDT satisfaction of the basic psychological needs of autonomy, competence and relatedness contributes to increase intrinsic motivation and well-being (box 1) and may explain the link between leadership and nature of motivation of health workers.60 61 Elements of SDT have been used in research in health in LMICs.62–66
Basic psychological needs
Feeling of psychological well-being is conditioned by the satisfaction of three basic psychological needs (autonomy, competency, relatedness).
Autonomy corresponds to the sense of volition and willingness one feels when undertaking specific behaviours. This allows staff to self-endorse their actions.
Competence needs refer to the feeling of self-efficacy when experiencing work opportunities that allow individuals to express and use their abilities and skills.
Relatedness means that staff have a specific need for mutual respect, consideration from others, connectedness and a sense of belonging to a social group.
The organisational context
In figure 2, we present how the influence of leadership on staff motivation depends on contextual conditions, including organisational culture, the nature of tasks and individual characteristics. We mean by organisational culture (OC) “the shared values, underlying assumptions and expectations that characterise organisational membership”.67 OC is rooted in history, evolving with the context and somewhat resistant to manipulation from managers.50 68 Box 2 presents the main types as defined by Cameron and Quinn69 (see online supplementary file 1).
Typology of organisational culture adapted from Cameron and Quinn69
Hierarchical culture: strong emphasis on stability, predictability and efficiency. Formalisation, procedures and rules govern individual behaviour.
Clan culture: emphasis on cohesion, teamwork, high levels of employee morale, employee involvement and commitment within an autonomy supportive environment.
Market culture: emphasis on employee productivity, results and profit orientation, individualism and competitiveness, in an environment that is considered as hostile.
Adhocratic culture: emphasis on creativity, innovation, individuality, experimentation, risk taking and adaptability. Power is decentralised to task teams.
Organisational climate is considered as an artefact, the tip of deeper cultural level of the organisation culture ‘iceberg’ and represents ‘the visible behaviour of group members’.50 Organisational climate is a temporal perception, tightly connected to the feelings, thoughts and behaviours of staff and reflects the way staff experience leadership practices.68 70–73 We agree that there is a truly complex relationship between leadership, motivation and organisational culture, but this is outside the scope of this paper.
Methods
We adopted the realist evaluation (RE) approach to open the black box of the relationship between leadership, motivation and individual performance, and framing these against the organisational characteristics and the context. RE is a suitable approach to deal with complex issues.4 74 75 Ontologically, RE acknowledges the multilayered aspect of social reality in healthcare settings and epistemologically allows for causal complexity.53 76
We adopted the case study design because it allows for an in-depth exploration of multifaceted complex phenomena as they play out in real-world settings.77 We defined the case as the relationship between leadership and managerial practices on one hand and individual motivation and performance on the other hand. We purposefully selected a well-performing hospital (positive deviant case) that obtained high scores in the quality assurance programme (Concours qualité) between 2011 and 2016, despite being situated in the prevailing hierarchical and resource-constrained context of the Moroccan public health system. Furthermore, there was a significant turnover of directors, which allowed us to compare leadership styles over time. It should be noted that this study is part of a PhD study that explores the relationship between leadership, public service motivation and performance of Moroccan hospitals.
The overall PhD study aimed at (1) describing how complex leadership is being conceptualised and applied in healthcare; (2) unravelling the underlying processes that link leadership to health workers’ motivation, the organisational characteristics and contextual conditions within which these processes are enabled or hindered; (3) exploring how the notion of public service motivation is defined by health workers, exploring the differences in the definition by cadre and identifying the factors that may influence PSM. For further details, see previous works.39 78 79 Indeed, the general design of the larger PhD study is a multiple embedded case study that proved appropriate in testing and refining theoretical propositions guided by the RE cycle presented in figure 3.

Methodological approach (adapted from Pawson et al 86 and Marchal et al (2012).
The selected public hospital, coded NHMH, is a small-sized provincial hospital built in 2004 in a periurban area with five municipalities. It has 50 beds and serves a population of 369 000 inhabitants. It provides basic non-specialised care (paediatrics, obstetrics, gynaecology, internal medicine, surgery, reanimation and emergency care). The population is also served by 18 primary health centres and 5 private general practices. In 2017, the hospital had a low hospitalisation rate (1.89%) and a short average length of stay (2.4 day), a low bed occupancy rate (25%) and a high rate of interhospital transfers (1.719 referrals) to the nearby teaching university hospital. In 2018, the hospital had 26 physicians (19 specialists and 7 general practitioners), 58 nurses and 9 administrative and technical support staff. Its revenue is mainly dependent on government subsidies, which constituted US$385 009 or 74% of the hospital budget in 2017; patient fees represented the remaining 26% of the budget. Most of the hospital users are indigents and are covered by the national health insurance plan ‘RAMED’ (Source: Strategic hospital report, key informant data).
Data collection and analysis
We based the choice of the data collection methods on our initial programme theory (figure 2) and used interviews, focus group discussions (FGDs), a document review and observations to collect data. The on-site data collection was carried out during a 2-week field visit in January–February 2018.
Interviews and FGD
In order to identify respondents, we carried out a qualitative purposive sampling (Patton80) among hospital staff. In line with realist principles, the selection of respondents was guided by our initial programme theory. We aimed at having respondents with a good variation of work context (eg, emergency unit vs outpatient unit) and cadres. Interviewees working at different managerial levels and all categories of health workers were represented (doctors, nurses and technical staff) (see table 1 and online supplementary file 2). We used the snowballing technique to identify key informants who no longer worked at the hospital. Thirty-two respondents were recruited (4 senior, 3 intermediate and 5 operational managers, 6 doctors and 1 pharmacist, 10 nurses and 3 technical staff).
Supplemental material
Individual characteristics of respondents
We collected qualitative data until saturation was attained. In total, we carried out 18 open-ended interviews and 1 FGD with nurses (n=9). Two planned FGDs became in-practice group discussions because of the low number of participants: doctors (n=3) and administrators (n=3). The shortage and availability of doctors and administrators explained the limited number of participants.
For the open-ended interviews, we developed interview guides that were tested in a pilot provincial hospital with a similar study population. The guides were used as a reminder for the interviewer and not to conduct semistructured interviews (see online supplementary file 3). The interviews were carried out in Moroccan dialect at the hospital and in places convenient for the interviewees. The average interview duration time was 59 min (minimum 20 min–maximum 118 min).
Supplemental material
The FGD and group interviews were animated by the first author and were carried out in the nurse duty room, the meeting room for doctors and the workplace for administrators. Vignettes and follow-up questions were used to guide the discussion (see online supplementary file 4). During the discussion, key themes were summarised and verification was sought from participants.81 82 At the end of the FGD and group interviews, we noted the disposition of participants, and salient themes, intuitions and interpretations.
Supplemental material
All interviews and the FGD were audio recorded with the exception of the group discussion with technical staff. In this specific case, we took notes and transcribed the interview using memory recall at the end of the group interview.83
Document review
We collected documents from key informants, including strategic hospital plans, and data on hospital key performance indicators, including HR data. We obtained the quality performance scores of the national quality contest (concours qualité) of 2010, 2011, 2013 and 2016. The concours qualité is a programme carried out by the Ministry of Health and consists of a self-assessment and an external audit. The assessment tool has 78 items that represent 8 dimensions of performance: (1) accessibility/availability/continuity; (2) patient security and responsiveness; (3) satisfaction; (4) ethics; (5) quality assurance; (6) resource utilisation; (7) technical competencies and (8) leadership.
Observations
The first author carried out non-participant observations during the fieldwork (between appointments), following observational guidance described by Spradley.84 Close attention was paid to the interaction between supervisors and staff: who interacts with hospital staff, what is the sequence of events, where and how were meetings held (physical space, feelings and goals expressed during formal and informal interactions). Notes were taken, transcribed and entered in the NVIVO database.
Analysis
During the data collection process, the first author kept track of salient issues, themes and self-reflection arising from each field contact and from the observations by drafting contact summaries as described by Miles et al.85 Preliminary analysis started during the field work.81
Once all data were collected, all recordings were transcribed verbatim and entered in an NVIVO database. We coded all transcripts, field notes and contact summaries using concept and in vivo coding.86 This was followed by a thematic analysis which was guided by the initial programme theory (see figure 2). The resulting themes included leadership styles (laissez-faire, transactional, transformational, distributed leadership), organisational characteristics (organisational culture, organisational climate (eg, clan culture, perceived organisational politics, job pressure, perceived supervisor support, perceived organisational support), individual characteristics (public service motivation, intrinsic motivation, extrinsic motivation and basic psychological needs (autonomy, competence and relatedness needs)). We used an iterative process inspired by the causation coding method85 86 to identify respondents’ reasoning about the causal pathways between leadership, motivation and performance (see figure 3).
In RE, cumulative validation refers to the iterative processes of theory construction, testing and refinement. In the process, causal linkages between structures and agents within a system are identified to build a plausible explanation for the observed outcome. We used the Intervention-Context-Actors-Mechanism-Outcome configuration (ICAMO) as a heuristic tool to explicitly describe and identify plausible causal configurations.87 We defined ‘mechanism’ as the individual reasoning and resources as described by Pawson and Tilley88 and Westhorp.89 We identified the reasoning of the interviewees about causal pathways: how individuals interpret their social world structures and events determines their attitudes and behaviours.90 Additionally, causal powers in social systems lie in the social relations between the individual (reasoning and volition) and the organisational structures (leadership, culture, social groups).88 We looked specifically at the interaction between leaders and their followers, the psychological processes of individual motivation and the drivers of individual performance as situated within the interviewee’s context.
Patient and public involvement statement
There was no direct involvement of patients in this study.
Results
In this section, we present first the organisational characteristics (performance, structure and culture), followed by the leadership practices displayed by the different chief executive officers (CEOs). Finally, we will present the causal configurations underlying the linkages between leadership, motivation and performance.
The hospital and its performance
This hospital was opened in 2004. The performance of the hospital in the quality assurance programme improved significantly between 2010 and 2016: the overall performance score index increased from 42% in 2010 to 83% in 2016.
Organisational structure
The hospital has relatively small clinical units, which are supervised by a doctor and nurse-in-chief. Both interact directly with the hospital director and the provincial health officer (PHO), whose office is located within the hospital. The hierarchical line is therefore short. The managers of the clinical units interact directly with patients (Source: Researcher’s field note, 30/2/2018).
Organisational culture
The hospital is characterised by a strong clan culture. The respondents express strong feelings of belonging to the same entity (esprit de corps).
We become family. The majority of us are like brothers and sisters. We are part of “DART” (a rotating saving group). We go together to weddings, we shop together, we eat together. We love to work together. (NHMH 12, administrator)
Respondents express feeling proud to belong to this group, which facilitates openness of expression, communication and collaboration. Respondents from all cadres indicate that friendliness defines their daily interactions. This, in turn, facilitates trust among group members and their effective cooperation.
Here, we have a strong team spirit. We are open to talk about everything when we are together. Whenever I had an exam at the university, I gently asked my colleague to fill my position for a half day, and afterwards I give her back this service. We accomodate each other and I support her whenever she needs me on her shift. We are all cooperative. (…) Trust, they trust me, this is the most important thing. They know that I will not harm them. If this was not the case, we would be having conflicts and be shouting at each other. (NHMH 8, midwife, midlevel manager)
It was a pleasure to work in teams. A key characteristic of these teams is friendship: staff are considered as friends, we care for each other. I watch over their interests. We held our director in high consideration. I would not have participated to quality circles if I disliked the director. (NHMH 10, doctor)
Age is another connector. Staff tend to identify themselves as belonging to the same age category and this enhances their feeling of group cohesion.
Before, I worked in another hospital where young people were few and were unable to express their opinions to the administration. In this hospital, it is really different. We have the same age more or less, we support each other, we listen to each other. (NHMH 20, nurse anaesthesiologist)
Respondents note there are little status differences between nurses, doctors and administrators, which allows them to identify with the hospital and not just with their specific professional category or age group.
There is no status difference between nurses and doctors. Everyone is a one single corps. (NHMH 6, doctor, specialist)
Our analysis shows that this has implications for staff motivation and organisational commitment. Health workers felt committed to the hospital because they have a strong feeling of ‘being one’, of belonging to the same group with the same ‘esprit de corps’.
What motivates me in this hospital is the work ambiance, the youthfulness and the dynamism of my team members. (NHMH 20, nurse anaesthesiologist)
Another hallmark of the organisational culture in this hospital is the shared beliefs and values concerning integrity and moral conduct.
An important issue in this hospital, thank God, all staff are honest. They do not take bribes. They are not corrupt. Patients do not bribe the surgeon or nobody else here to have a cholesystectomy and they are operated in due time. (NHMH 10, doctor, specialist)
We found that this clan culture was shared by all staff categories and that it remained stable despite the high turnover of hospital directors.
Leadership practices
Since its opening in 2004, there has been a high turnover of hospital directors (table 2). Our analysis shows this had an impact on the organisational climate and on the organisational performance.
Sucessive leadership periods (leadership styles, perceived leader support, organisational culture)
From 2007 until the end of 2013, the hospital was managed by chief executive officer 1 (CEO 1). He was a physician with no formal training in management. He adopted a rather distant, transactional leadership style and emphasised compliance with rules and procedures. He retired in December 2013. During this period, the provincial health officer (PHO) continued to play an important role in the hospital. He, too, adopted a strong transactional leadership style, but he was appreciated by staff because they felt he was responsive to their needs. He showed strong consideration for individual staff members and concern for their well-being.
He, may the grace of God be upon him, was severe. He had an administrative attitude. However, he upgraded a resting room for doctors within the operating theatre. He improved our working conditions (offices, sanitary), whereas the former two PHOs did not respond to our needs, even though we relentlessly asked them to. (NHMH 25, doctor)
When there was a farewell, he brought me himself my share of sweets and juices. (NHMH 12, administrator, close collaborator)
He displayed altruistic behaviour and encouraged the continued education of staff. He upheld high ethical standards. Respondents noted that he was a role model and a source of inspiration to hospital staff.
He [The PHO] initiated the quality culture at the hospital. He appointed project managers, he was visionary. Five of the project managers who remained were commited to the quality culture. Although he passed away in 2014, it was him who made who they were. (NHMH 30, senior manager, nurse)
From 2014 to 2016, NHMH was managed by CEO 2. During this period, the hospital achieved the second position in the national quality contest. Our analysis showed that CEO 2 displayed distributed leadership. He fostered the creation of networks and experimented with interdisciplinary committees, which carried out quality circles called ‘Kind heart actions’.
I said, why would not we experiment something. Let’s create committees - it was the first time - to monitor stock management of medical fluids, catering waste or patient catering. We created teams that supervised each activity. We agreed that we would do an experiment with these committees. If it wouldn’t work, auditors would come and tell us what did not work. (NHMH 32, CEO 2)
These interdisciplinary committees included a quality manager, physicians, nurses and pharmacists and this enabled sharing of ideas and creative problem solving. CEO 2 stimulated line managers and members of ‘kind heart action’ committees to adopt a distributed leadership style themselves. This was successful in that a number of staff took up such a leadership style:
I am close to the personnel. I have a nearby management style. I try to be close to physicians. I try not to create tensions and they listen to me a bit. I try to understand their specific needs. (NHMH 11, surgeon, intermediate manager)
The quality circles created conditions that were favourable to close interaction between different staff members across hospital units and departments. As a result, innovative solutions emerged in response to problems.
The former director catalysed teams, he gave us energy. We loved to work with him. We stayed till 8 pm in the evening. We worked during weekends. We worked hard. We were motived to work and perform. Actually, we feel the difference with other leaders. (NHMH 08, midwife)
Our analysis shows that CEO 2 had a clear vision on management and that he was able to communicate that vision, clarifying goals and increasing the mission valence (eg, quality of care, organisational citizenship). It emerges from our data that CEO 2 also displayed nearby leadership: he was responsive to individual staff needs, showed individual consideration and supported them in doing their tasks. CEO 2 enabled dialogue and accepted divergent opinions. This was highly appreciated by staff; it enhanced their self-esteem and perceived supervisor support. This, in turn, increased staff commitment and respect. Staff considered him to be a role model.
The former CEO did not have a distant attitude. When I met him in the hallway, he communicated with me respectfully. He asked me about my personal health: “Is everything ok?”. He greeted everyone. Then when he needed an anaesthesiologist to fill an unplanned shift position outside working hours, I accepted the job because that day he showed consideration for me. (NHMH 02, nurse anaesthesiologist)
The former Hospital director was often close to the field. He was a guy who rolls up his sleeves and organizes himself the emergency cart. He empathized with a nurse who had night shift, wear his pyjama, organized himself the emergency cart. He organizes the medicine cabinet. (NHMH 01, senior manager)
CEO 2 was very dynamic, he was very good as a role model. He involved all personnel. We had several meetings to discuss our concerns and service fonctioning issues. We engaged toward quality objectives. This was a true example for staff motivation (…) The objectives were to improve working conditions, and to understand staff needs, valuing teamwork and participative decision making. (NHMH 31, doctor)
Our data show that the distributed leadership and the quality circle interventions were congruent with the organisational culture described above. CEO 2 provided room for staff discretion (micro-emancipation), for instance, by allowing them to arrange their own shift schedules and working practices, while setting simple rules to guide the overall performance (eg, focus on quality and patient satisfaction). This promoted staff autonomy and thus enhanced employee self-esteem, while addressing staff’s needs for discretion in decision-making.
The former director said: ‘You manage your unit as a team. Do whatever you like in the service. The operating theatre is your kingdom. Then do whatever you like, but what I care for is that patients do not come complaining to me about the quality of service. (NHMH 02, nurse, anaesthesiologist)
Responsiveness to staff needs for discretion through participative decision-making enhanced their organisational commitment.
When leaders involve staff in decision making, staff are committed. Work flows smoothly. (NHMH 23, nurse)
“I told them (the staff) to make the hospital plan they see appropriate. What is your vision of your hospital? I am just a passerby in this hospital. I will stay 2 or 3 more year and quit. It is you who will stay at the hospital. How many hospital directors have you seen? How many provincial health officer have you encountered. You will remain at the hospital. This is why give me your vision about the hospital!]. It is important to involve people in decision making. It is necessary to use what we call in our jargon the participative management. You need to involve them all. This way, you increase their self-esteem, when you ask them how do you prefer this mug (a metaphor) this way or that way. I will bring you the glass you chose. (…) Involving staff in decision making in hospital development plans enhances their sense of belonging. (NHMH 32, CEO 2)
Our analysis shows that during the time of CEO 2, a positive organisational climate emerged within the hospital.
The former CEO was animated. He was open to discussion. He changed the organisational climate. He acquired necessary material, but his stay was short. He did not last long enough, but the hospital was catalysed. (NHMH 25, doctor and operational manager)
CEO 2 left in June 2016 and he was replaced by CEO 3, who had a more distant, laissez-faire leadership style. The staff found his communication style to be poor. Respondents indicated that this led to mistrust between the management team and staff. They mentioned that CEO 3 was not responsive to staff needs (for instance, not addressing problems of shortage of consumables and of maintenance of equipment). This led to increased job pressure and demotivation of staff.
CEO 3 was reluctant to solve problems. He did not want to be bothered. At that time, we had issues with medical waste. We suffered from shortages of bed sheets. An electrocardiograph and tensiometers were not available at the emergency room! (…) Once, he aggressively blamed me for refusing to use non-sterilized instruments due to a broken autoclave . (…) He even passed by me without greeting me at all. Consequently, I stopped complaining about material shortages and tried just to do my night shift with the minimum available material. (NHMH 4, nurse)
The organisational climate was rapidly characterised by perceived organisational politics, which led to tensions within the hospital between union representatives and contributed to strikes. The laissez-faire leadership led to a breach of trust between the staff and the administration and reduced their organisational commitment of the former.
There was not a good organisational climate. This was due to the hospital direction. (…) There were many problems, conflicts, an instable climate. But the CEO did not intervene, he did not make promises, there was no improvement, no initiatives. Even when we asked, we were told there is no budget. (NHMH 31, doctor-in-chief of a clinical department)
We found that CEO 3 managed the hospital on a day-to-day basis: he did not present a vision, organisational objectives nor an action plan. His poor communication with close collaborators and staff contributed to a climate of ambiguity.
Staff were no longer motivated. He made promises he did not keep, they were just promises. There were no means, no defined objective, no engagement to quality or whatsoever, nothing at all. The working conditions were deteriorating! (NHMH 31, doctor)
Low participation in decision-making induced decreased perceived supervisor support and staff resistance. Front-line workers were resisting the directive attitude of CEO 3. They expressed how they appreciate being consulted and involved in decisions that concern them.
CEO 3 was a colleague, a friend. But CEO 3’s leadership was not effective. Why? Because he overrelied on administrative correspondence. He was confronted with staff resistance. (NHMH 25, doctor, intermediate manager)
A good leader is the one who involves his staff in decision making. Obtaining consent from staff is very important. We are committed to decisions taken on the basis of constructive dialogue with staff. For instance, in my specific case, when mobilising a nurse from a service to cover a vacant position in an another service. I did not accept because this decision was forced on me without concertation. This is important even for temporary mutation to cover personal shortage in the intensive emergency units. I do not accept that the director asserts his power on me. I have also the power to say NO !. (NHMH 24, nurse anaesthesiologist)
Trust in CEO 3 was breached when staff perceived him as working behind closed doors and inducing clientelism and nepotism. This was not accepted by staff because it was perceived as incongruent with their shared beliefs about integrity an moral conduct. This perceived organisational politics impacted negatively on their organisational commitment.
With the previous CEO 3, procurement processes were not transparent. Deals with suppliers were shady. He may had sought personal gain…!!. This is his business and he will be sanctioned by God. Our concerns is the patients. We behave in accordance to God’s norms. (…) Nursing staff are committed to the hospital only when the CEO is honest and working correctly! (NHMH 23, nurse)
In October 2017, yet again, a new hospital director was appointed. CEO 4 was the director at the time of data collection. This leader had a formal training in management and he emphasised re-establishing trust between staff and administration by engaging the former in decision-making.
Participative decision making increased the transparency and increased the level of trust. We presented the budget plan to the staff. We worked in a climate of transparency, we had nothing to hide. The result of this meeting was great. This way we gained the trust of the team. (NHMH 07, CEO 4)
Besides, CEO 4 focused on building alliances and gaining trust of informal leaders.
In this hospital, there is a strong level of unionisation. There are many influential people. I worked to gain their trust and included them in the team. I involved them in decision making, besides improving working conditions. We won a lot doing this (NHMH 07, CEO 4)
However, operational staff perceived him as distant transactional leader. CEO 4 reinforced the hierarchical line that was not respected by his predecessor. The information flow was again regulated through the formal hierarchical line. This was perceived by staff as ineffective in dealing with urgent issues and reducing their perceived autonomy support, and consequently reduced their internal perceived locus of control.
Before we did not have a chief medical officer; we had a chief nursing officer and an administrator. Everything worked smoothly. Now, progressively a distant management style is implemented. Tasks are regulated within supervisors’ spans of control. Administrative correpondance has to follow the formal flow of information. The chief nursing officer is distant, as if you talk to a corpse. A group of employees is favoured over others. A minority group is kept apart. Now, it is politics that prevail! (NHMH 12, administrator)
This approach, too, enhanced staff’s perception of increased organisational politics. Staff perceived negatively the hierarchical structure implemented by CEO 4 as reducing their ability to participate to decision-making and problem resolution and this reduced the dynamics of interaction between health units.
With the actual CEO 4, we now have a chief nursing officer, a chief medical officer; no more committees were created. We need to wait long for things that are simple and practical. We are told to respect the hierarchical line. We are not well received. Some objectives are now decided without concertation with the operational staff. (NHMH 31, doctor-in-chief of clinical department)
The Chief Nursing Officer reduces my interaction with the direction, stipulating that I am under his direct supervision and not under the hospital director’s supervision. (NHMH 08, nurse, intermediate manager)
By providing resources and improving work conditions, however, job pressure was reduced and the work climate progressively improved.
The service is running, we have good activity statistics. What is lacking is quality of care. Staff need more efforts from managers to provide adequate resources to improve working conditions (standardisation of patient flows, providing tools) in order to maintain the staff’s motivation and performance. (NHMH 31, doctor)
Summary of the findings
Our initial programme theory stated that “public-oriented health care organizations that are well performing are likely to be characterized by a high congruence between leadership styles and practices, organisational characteristics and individual staff attributes. More specifically, managers adopt an appropriate mix of transactional, transformational and distributed leadership styles that fits the mission, goals, organisational culture, and nature of tasks of the organisation as well as the individual characteristics of the personnel in terms of age, gender, professional profile and motivation.”
Our findings confirm the second part of our initial programme theory. Given the nature of hospitals as hybrid professional and mechanical bureaucracies, in which staff with different professional backgrounds need to collaborate in order to be effective, effective leaders adapt their leadership style to the different cadres and individuals as needed. We found that this adaptation of leadership style enhances staff PSS and POS and this contributes to the satisfaction of their basic psychological needs.
We found that laissez-faire leadership decreased the levels of POS and staff motivation by being less responsive to their basic psychological needs. Lack of vision and goal setting created a climate of ambiguity and conflict of roles. The inadequate enforcement of the hierarchical structure and high job pressure, which staff could not cope with, contributed further to a general malaise during some periods. This led to further mistrust between administration and staff and demotivation of staff.
We confirmed that transactional leaders are effective if they offer the employee the necessary support and ensure adequate working conditions. By improving the latter, transactional leaders reduce job pressure, and by implementing a clear hierarchical line, they reduce role conflicts. This explained why under the directorship of CEO 1, doctors were motivated, although they perceived that their leader was effectively asserting his power and control. However, if transactional leaders are felt to be distant, this tends to reduce the perceived autonomy support and the satisfaction of the need for mutual respect (relatedness), leading in turn to reduced motivation.
Our study showed that transformational leadership enhanced staff self-esteem and perceived autonomy support. Our findings indicate this contributed to expressed mutual trust between the director and the staff.
We found that under CEO 2, distributed leadership contributed to better interaction between staff from different health units and to improved communication flows, creative problem solving and a reinforced clan culture. Distributing leadership and embedding it throughout the organisation, combined with engaging staff in decision-making, led staff to perceive their activities as depending on their own volition (eg, planning the shift schedule). This increased their perceived autonomy support, and as a consequence, staff felt more committed to the organisational goals. This stimulated them to adopt extra-role activities (such as working off duty hours).
In short, our results show that leaders can contribute to better staff motivation if their leadership style matches the expectations of the different cadres. For professional cadres, this means effectively enabling and supporting them, as well as unit managers to take up their professional responsibilities. Other cadres may expect a more directive approach that is structuring and clearly indicating the task distribution, combined with close supervision. Leaders should adapt their practices accordingly—one size does not fit all.
We summarised our findings using the ICAMO heuristic tool in four plausible causal configurations presented below and summarised in table 3. It presents causal configurations confirmed by our empirical data.
ICAMO plausible causal configurations
Configuration 1
(I) Laissez-faire leadership decreases the levels of perceived organisational support (O) and staff motivation (O) by being less responsive to their basic psychological needs of autonomy, competence and relatedness (M). (I) Lack of vision and goal setting contributes to a climate of ambiguity and role conflict [C]. (I) The inadequate enforcement of the hierarchical structure and [C] high job pressure can contribute to mistrust between administration and staff (O).
Configuration 2
Transactional leaders (I) can improve extrinsic motivation (O) of administrative staff [A] if they offer the necessary support (I) and ensure adequate working conditions (I). By improving the latter, transactional leaders reduce job pressure (O) and by implementing a clear hierarchical line (I), they can reduce role conflicts (O) for administrators [A].
Configuration 3
By showing individual consideration (I) and communicating clearly about mission valence (I), transformational leaders enhance self-esteem of staff (M), perceived supervisor support (M), and satisfaction of their autonomy needs (M). This, in turn, contributes to staff commitment (O), mutual trust (O) and respect between the management team and staff (O).
Configuration 4
Distributed leadership (I) can contribute to improved communication and interaction between staff from different units (O), to problem solving (O) and a reinforced clan culture [C]. Distributing leadership roles and embedding them throughout the organisation (I), combined with engaging staff in decision-making (I), contributes to staff’s perceived autonomy (M), which in turn leads to organisational commitment (O), which contributes to extra-role activities (O).
Discussion
Our study aimed at exploring the underlying mechanisms that underlie the relationship between leadership and motivation, and framing these against the organisational characteristics and the context. Our analysis points to the key role of POS and PSS, and of satisfying the basic psychological needs of staff.
In the following section, we frame our findings against the literature.
Leadership styles and consequences
In line with other leadership studies,91–93 our findings indicate that laissez-faire leadership decreases the level of POS and staff motivation by being unresponsive to staff needs of autonomy, competency and relatedness. Our study has also indicated, similar to other studies,94 95 that lack of vision, poor leadership and lack of reinforcement of the hierarchical line may lead to high job pressure, mistrust between staff and administration, and turnover.
Our study showed that the over-reliance on transactional leadership in the leadership practices of CEO 1, 3 and 4 seemed to have had negative effects on staff motivation and levels of trust in the organisation, in line with other studies.94 96–100 An unexpected finding was the role of perceived organisational politics as a key contextual condition hampering leaders’ effectiveness. Perceived organisational politics understood as the perception of nepotism and lack of fairness and procedural justice in organisations seems to negatively influence the effect of leadership on staff and organisational performance.101 102
Our study, similar to other studies,103–105 indicated that transformational leaders who show individual consideration and clearly communicate their vision increase self-esteem of staff and perceived supervisor support, and satisfy their relatedness and autonomy needs. This may contribute to staff commitment, mutual trust and extra-role performance.
Our findings support the notion that complex leaders inspire followers by clearly communicating the organisational vision and articulating it with the interests of individual staff. They work on increasing the valence of staff’s efforts. They do so by adapting their style to the needs of cadres and staff. As a consequence of this fine-tuning of their leadership practices, they influence followers’ autonomous motivation by enhancing POS.106–112 This contributes to better performance in the sense of extra-role performance106 113–115 and increases mutual trust between leaders and staff.96 116–119
By distributing leadership across organisational levels, CEO 2 may have created the conditions for the formation of a shared identity and a high sense of collective efficacy, similar to what other authors have found.120 121 This was obtained by involving staff in decision-making and by creating committees and networks. It helped to create a sense of belonging to a group and respondents expressed high levels of organisational commitment. Distributing leadership and involving professional staff in decision-making responds to their autonomy and social relatedness needs.122 123 This is consistent with findings from other leadership research that emphasised the role of complex leaders in stimulating open communication, network construction and non-linear process that enable collaborative learning, innovation and perceived team performance.39 48 124–130
In summary, complex leadership understood as balancing transactional, transformational and distributed leadership fostered innovative problem solving and enabled staff interactions. This leadership effectiveness seems to be conditioned by the value congruence, responsiveness to staff needs and the absence of perceived organisational politics. In such situations, staff are likely to be autonomously motivated and to internalise public services values. Our findings suggest that this contributed in turn to higher organisational commitment and staff extra-role performance.
Our study indicates that POS and PSS may be triggered by leadership practices in certain conditions and that this may lead to higher organisational commitment, reduced staff turnover and reduced absenteeism.54–56
Our scoping review showed that complex leaders (CLs) balance between transactional, transformational and distributed leadership in function of the situation and needs.39 They address staff’s basic psychological needs and more specifically the need for competence by providing them with training opportunities, supplies and good working conditions. Distributed leadership responds to staff’s autonomy needs and triggers a perception of autonomy support, PSS and POS. The need for relatedness is addressed by creating supportive and open climates, good relations between people, and among others. All combined, such leadership practices sustain the autonomous motivation, which has been shown to be associated with effective functioning, better psychological health, well-being and persistent motivation.60 Our study seems to confirm these effects.
Refined programme theory
Figure 4 depicts the refined programme theory, indicating in blue the mechanisms we found to be triggered in this hospital. This suggests that health workers’ motivation seems to be explained by plausible causal mechanisms situated at different levels (individual, leadership practices, organisational context and external context). The empirical data provided support to the initial programme theory (figure 2) that has been specified as follows: “Leaders able to adapt their leadership practices to staff needs (autonomy, competence, relatedness) and the nature of their tasks increase their intrinsic and public service motivation by increasing the perceived supervisor support and perceived organisational support, when the organisational culture is conducive (absence of perceived organisational politics).”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Refined programme theory. Mechanisms appear in blue text. Arrow with “-” sign: negative effect; arrow with “+” sign: positive effect.
Study contributions and limitations
This study provides evidence that may contribute to fill a gap in complex leadership studies by addressing the underlying psychological processes, mechanisms and conditions through which leaders motivate followers, an issue which has received little attention in general131–133 and specifically in the field of healthcare.39 130 It may also contribute to fill the gap in leadership research in Muslim countries, under-respresented in the leadership research field.134 Another contribution is the application of the RE approach to unravel the relationship between leadership, staff motivation and performance in healthcare.
There are some limitations to our study. In the ‘Concours Qualité’ (CQ), scales psychometric properties were not tested for their internal validity.23 135 However, the rigorous annual implementation process of CQ at all Moroccan hospitals from 2010 to 2016 provides us with reliable data on comparative historical trends of organisational performance across all Moroccan hospitals.23 135
Furthermore, we did not quantitatively assess PSS or POS, nor use the Cameron and Quinn Organisational Culture Assessment Instrument to assess organisational culture types. The first reason is that the overall objective of this study is to explore the links between leadership and motivation. Second, given time and resource-constraints, we were not able to validate the existing scales, measures and tools used to identify, for instance, the type of organisational culture.
We acknowledge that our study findings might be affected by recall bias and temporality, commonly encountered in retrospective REs,136 and in any retrospective study in general. However, validation during FGD and the analysis of HR archives helped us improve the accuracy of information collected.
We are also aware that at one point in time, data collection has its limits when exploring the dynamic nature of leadership processes.49 137
Conclusion
In this study, we found that the leadership at a well-performing hospital was characterised by a good fit between the leadership styles, the organisational characteristics and the individual staff attributes. Leaders who display complex leadership behaviours respond better to the nature of the hospital and its mission, the nature of the task and the individual staff characteristics (age, professional profile and motivation). This study opens the door for more explanatory research on the relationship between leadership, motivation and staff performance, which can validate or falsify the ICAMO configurations presented here. Future researchers could seek to empirically test the role of responsiveness to basic psychological needs, trust, POS and PSS in explaining the motivation of staff and effectiveness of leadership in healthcare settings.
Acknowledgments
We would like to thank the NHMH hospital director, provincial health officer and staff who participated willingly to the study. We would kindly like to thank the reviewers Rohan Jayasuriya and Thu Nguyen for their insightful comments and suggestions that improved the quality of our manuscript.
References
Footnotes
Twitter @drbelrhiti
Contributors All the four authors (ZB, BM, WVD, AB) contributed significantly to the original design, analysis and interpretation of data, and writing of the manuscript. ZB carried out the data collection. AB and BM cross-checked the transcripts. Initial coding was done by ZB and discussed between the research team members (ZB, AB, BM, WVD). ZB and BM edited the final draft. All authors read and approved the final manuscript
Funding This work was funded through a PhD framework agreement between the Belgian Directorate-General for Development Cooperation and the Institute of Tropical Medicine, Antwerp.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The research protocol was approved by the Moroccan Institutional Review Board (No. 90/16) and the Institutional Review Board of the Institute of Tropical Medicine, Antwerp (No. 1204/17). All research participants were informed before the start of the data collection about the study’s objectives, the topics and type of questions, and their right to refuse being interviewed, to interrupt the interview at any time and to withdraw any given information during or after the interview. This information was provided through an information sheet and was explained before the start of the interview and focus group discussion. All respondents were presented an informed consent form, which was signed by them and countersigned by the first author. Respondents had the possibility to opt out at any time during the whole process and were given a copy of the signed informed consent form.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study.
Linked Articles
- Health services research