Article Text

Abstract
Objective To analyse poor physical function, pain, limited exercise and smoking, assessed in a patient-friendly self-report questionnaire format that has been completed by every patient at every visit over 20–30 years in the authors’ and other usual care settings, to predict 5-year mortality in a general older population.
Methods An extended version of a Multidimensional Health Assessment Questionnaire was mailed to 2000 subjects in Finland, identified as a randomly selected control cohort for a rheumatoid arthritis cohort. The questionnaire included queries concerning baseline physical function, pain, exercise and smoking status, identical to the clinic version, as well as age and 25 medical conditions. Five-year survival was analysed according to descriptive statistics, Kaplan–Meier curves and Cox regressions.
Results The questionnaire was returned by 1523 subjects (76%). Five-year survival was 94% in all subjects, 98% in subjects with no disease or no acutely life-threatening disease, and 17% in subjects with an acutely life-threatening disease. Hazard ratios (HRs) for 5-year mortality were 3.5 for poor physical function, 2.2 for pain, 5.2 for limited exercise and 4.6 for smoking (p<0.01); 5-year survivals were 93%, 97%, 93% and 95%, respectively, compared with 91% for hypertension. Each of the four patient history variables predicted mortality at higher levels in subjects who reported no versus one or more acutely life-threatening conditions.
Conclusions Poor physical function, pain, limited exercise and smoking can be assessed systematically on a simple standard Multidimensional Health Assessment Questionnaire, to identify potentially modifiable risk factors for premature mortality in the infrastructure of usual medical care and health maintenance.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
A simple, one-page patient self-report questionnaire to assess systematically physical function, pain, limited exercise and smoking has been completed by all patients at all visits in 5–10 min in routine care in several rheumatology clinical settings for 20–30 years, including those of the authors.
Responses on this questionnaire indicating poor physical function, pain and limited exercise have been documented as significant prognostic markers for premature mortality in patients with rheumatoid arthritis, with greater significance than radiographs or laboratory tests.
Questionnaire responses in an older cohort from the general population, identified from a population register as a control cohort for a rheumatoid arthritis cohort, indicated that poor physical function, pain and limited exercise also predicted 5-year mortality significantly, in the range of smoking and hypertension.
Key messages
Poor physical function, pain and limited exercise are potentially modifiable risk factors for premature mortality in the general population, in a similar range to that of smoking and hypertension.
A systematic assessment of these patient history variables is not included at most medical visits, in contrast to blood pressure or serum cholesterol, in part as most available questionnaire formats appear to add to the burden of care for patients and doctors.
Scores in a simple format on a questionnaire completed by patient self-report in 5–10 min provide quantitative data concerning physical function, pain, exercise status and smoking as significant risk factors for mortality, with virtually no additional work on the part of a health professional, to ensure that data are available for clinical review.
Poor physical function, pain and limited exercise are more significant in prognosis of death over 5 years in individuals who do not versus do report one or more potentially acutely life-threatening diseases.
Strengths and limitations of this study
Strengths
Population-based subjects? Survey returned by 1523 of 2000 subjects (76%).
Questionnaire easily completed by patient self-report in 5–10 min in any clinical or research setting, or even at home.
Limitations
No laboratory tests were available—it would be of interest to compare medical history variables with laboratory tests, such as serum cholesterol, in the prognosis of mortality, and whether a component of the risk according to the laboratory test may be ‘explained’ in part by a patient history measure.
All subjects were from Finland, although most data suggest that mortality experience in Finland is similar to that found in most Western countries, and reports from other countries have indicated that poor physical function, pain and limited exercise are prognostic of premature mortality. Furthermore, a response rate of >75% from the general population might be unlikely in most countries, and may be unique to Finland.
Diagnoses were available only from self-report, which can be inaccurate for certain diagnoses. However, the excess risk according to poor physical function, pain and limited exercise was greater in subjects who reported no versus any acutely life-threatening diseases.
Actual survey includes more queries and is not identical to that used in clinical settings, although actual queries about four risk factors are identical in clinical and study format.
Introduction
Poor physical function,1–7 pain,3 8–10 limited exercise11 12 and smoking13 14 are each potentially modifiable significant risk factors for mortality derived from a medical history. However, these risk factors generally are not assessed systematically or even available at most patient visits in usual medical care and health-promotion settings.13 15 By contrast, blood pressure and serum cholesterol are recorded carefully at most visits in contemporary routine care settings and health maintenance, although the risk for mortality associated with the patient-history-derived variables may be in a similar range.
One reason that patient history variables are not available in most care settings may be that reported data generally have been collected in complex, non-standard formats, which add to the burden of usual care. Therefore, a simple format for systematic collection of data concerning physical function, pain, exercise status and smoking in the infrastructure of usual care, with minimal additional effort on the parts of patients and health professionals, could provide a useful advance.
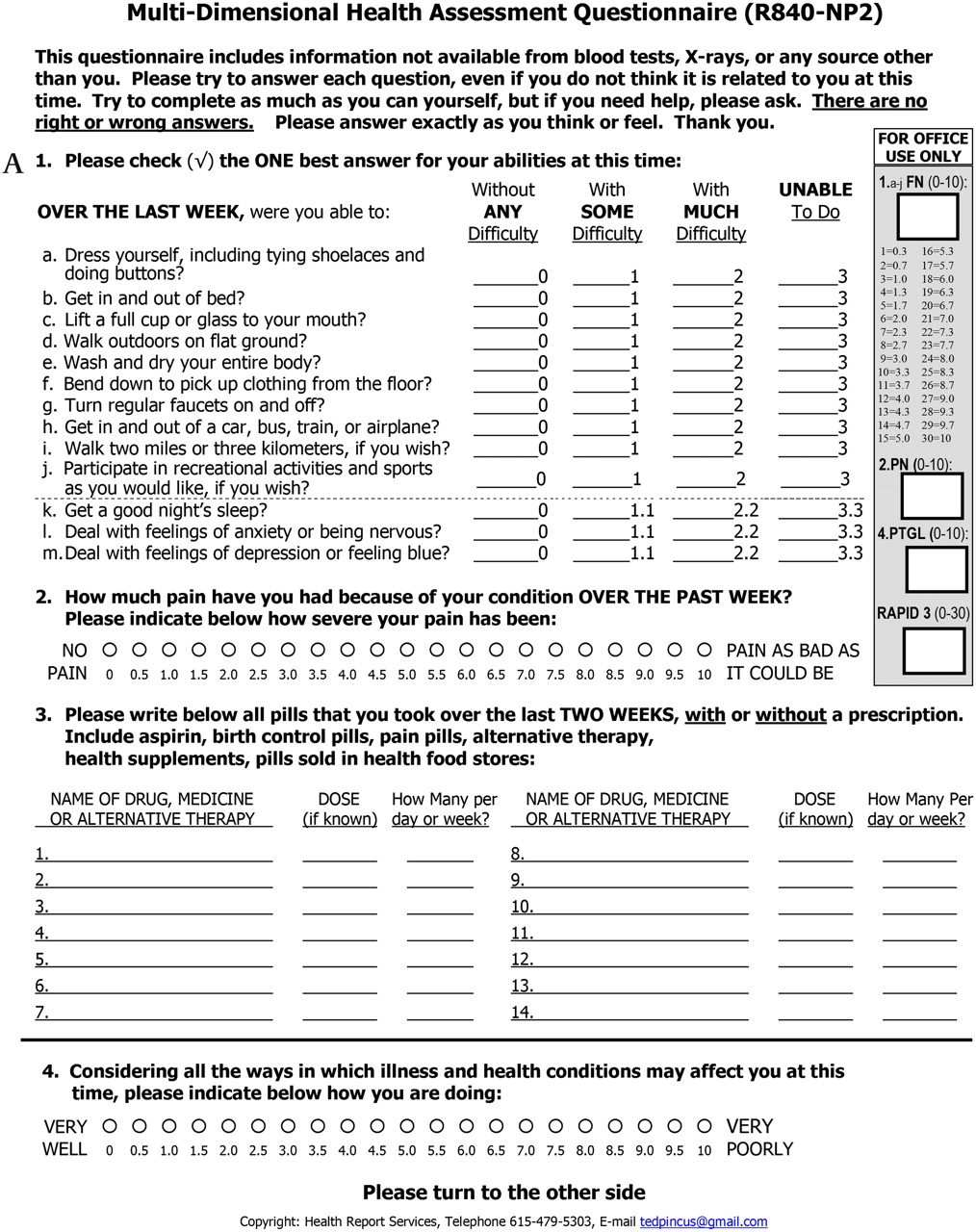
A simple, two-sided/one-page multidimensional health assessment questionnaire (MDHAQ)16 17 (figure 1) has been completed at every visit of every patient for 20–30 years in clinical settings of the authors, as well as other rheumatology clinical settings over many years.18–21 This questionnaire is readily accepted by patients, and completed in 5–10 min while waiting to see the doctor.21 Responses to MDHAQ queries concerning physical function, pain, exercise status and smoking are prognostic of premature mortality in patients with rheumatoid arthritis (RA).22 Since the MDHAQ format could facilitate availability of the information to any health professional caring for any individual patient, it appeared of interest to analyse whether responses concerning these variables on this simple questionnaire (in contrast to lengthy questionnaires used in research studies) would be prognostic of 5-year mortality in the general population.

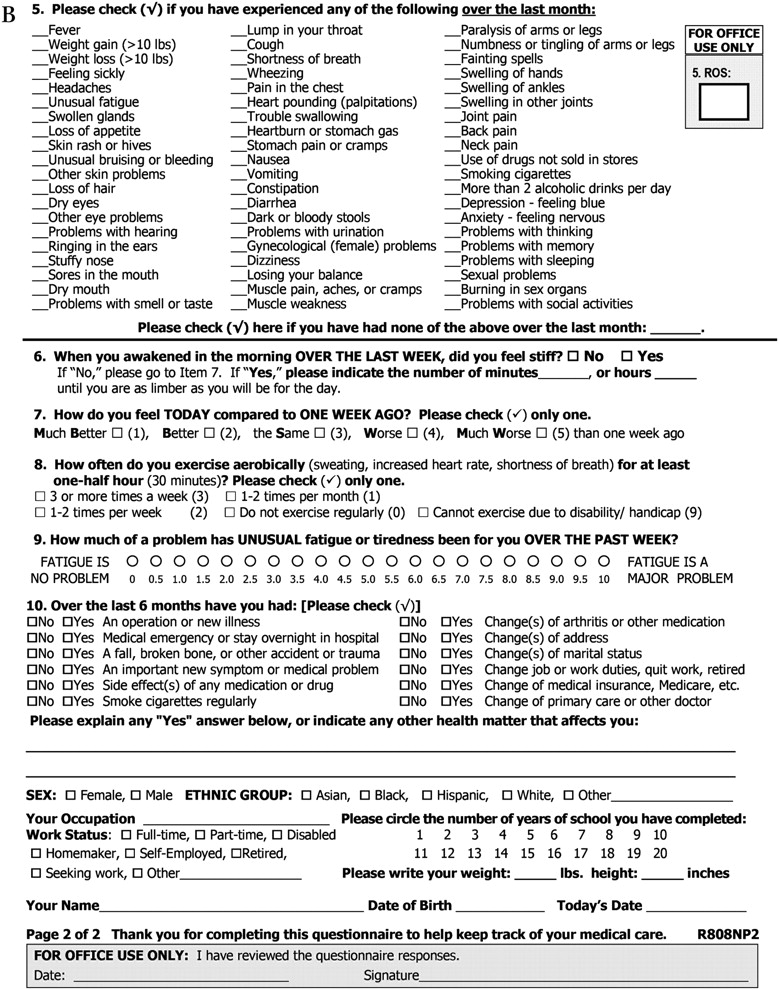
Multidimensional Health Assessment Questionnaire. The front page (A) includes 10 activities for function, two visual analogue scales for pain and patient global estimate of status, and a report of medications currently taken. Scoring templates for these measures are available on the right-hand side of the page. An index of the three patient-reported measures, routine assessment of patient index data, can be calculated from a Multidimensional Health Assessment Questionnaire in less than 10 s. The reverse side (B) includes a review of systems, fatigue visual analogue scale, recent medical history, queries about change in global status and frequency of exercise, and demographic data (not included in scoring, but providing useful data in clinical care).
A cohort of 1523 individuals from a normal older Finnish population had been assembled as a ‘control group’ to be monitored over long periods in comparison with a cohort of RA patients.7 23 24 These individuals had completed a questionnaire with MDHAQ queries (used in usual clinical care) for quantitative physical function, pain, exercise frequency and smoking. An earlier report indicated that scores for physical function, but not for pain, were prognostic for mortality 2 years later in this cohort, but the data did not include exercise status and were not adjusted for specific comorbidities, including the presence of acutely life-threatening diseases.7 In this report, we present analyses of 5-year survival according to baseline physical function, pain, exercise status, smoking and disease data collected on this questionnaire, in this randomly identified older Finnish population.
Methods
Subjects
The subjects were 1523 older individuals in the general population of the Central Finland District. Initially, in the year 2000, the Finnish Population Register Centre identified 2000 individuals from the general population as a ‘control’ population for a cohort of 1500 patients with RA who are being monitored for long-term outcomes.23 The cohort was designed to include 70% females, with a mean age of 55 years, but otherwise was identified randomly from the general population with no selection criteria other than age and sex.
A self-report questionnaire which included the items in figure 1 in an identical format, plus additional items designed for further longitudinal research, was mailed to the 2000 older individuals, identified randomly in the general population from the Finnish Population Register. The questionnaire was returned by 1523 subjects (76%). Earlier reports 2 years after baseline indicated that functional status was considerably poorer in age-matched patients with RA than in the general population23; that poor physical function not analysed according to possible diseases, but not pain, was associated with increased mortalities in both RA patients and the general population7; and that significantly higher mortalities were seen in individuals who did not return the questionnaire.24 Five years after the baseline assessment, in September 2005, the vital status of all subjects was ascertained from the Finnish Population Register. The study was approved by the Ethics Committees of Jyväskylä Central Hospital and Population Register Centre of Finland.
Self-report questionnaire
The self-report questionnaire mailed to subjects in the general population included the items on the MDHAQ in figure 1, and additional queries concerning diagnoses and demographic data for a research study. Physical function was queried on a version of the original Health Assessment Questionnaire (HAQ),25 which queries 20 activities of daily living, scored 0–3, with a mean overall physical function score of 0–3; similar results are seen with the inclusion of only 10 activities on a MDHAQ.16 17 Pain was assessed on a 10 cm pain visual analogue scale (VAS) (0=‘no pain,’ 10=‘pain as bad as it could be’) derived initially from Huskisson.26 The frequency of aerobic exercise was queried with five response options: ‘≥3 times weekly,’ ‘1–2 times weekly,’ ‘1–2 times monthly,’ ‘no exercise’ and ‘cannot exercise because of health conditions.’ Smoking status was queried as a response to ‘Do you smoke cigarettes at this time?’ with simple ‘Yes/No’ response options. A list of 25 health conditions (table 1), not included in the MDHAQ for usual clinical care, was included on the study questionnaire. Subjects were asked: ‘Which of the following conditions have you ever had at any time?’ with ‘Yes/No’ response options. The standard MDHAQ includes date of birth as well as recent medical history, list of medications, symptom checklist review of systems, and other variables in a two-sided, one-page format.27 28
Prevalence of conditions in the older general population: baseline scores for pain and functional capacity on the Health Assessment Questionnaire, according to status at 5 years
Statistical analyses
Data concerning survival of all subjects over 5 years were obtained from the Finnish Population Register Centre in 2005 and were computed according to a self-report of each individual condition, age, physical function, pain, exercise frequency and smoking. Analyses of mortality according to continuous variables were computed as median and mean values, and for dichotomous variables as percentages in each category. Statistical significance was analysed according to a t test and analysis of covariance for continuous variables and χ2 test for dichotomous variables.
Survival was analysed for subjects classified into three categories on the basis of results from the survey: no reported health condition; one or more condition(s) but no acutely life-threatening condition; and one or more acutely life-threatening condition(s), as defined by the findings described in Results. Few deaths occurred in those who reported no health condition, and further analyses were performed in two categories: no condition or no acutely life-threatening condition versus one or more acutely life-threatening condition(s).
Kaplan–Meier curves and Cox proportional hazard regression models were computed to analyse time-to-death in subjects according to: (a) physical function scores (range 0–3) of <1 versus ≥1, indicating moderate difficulty to perform activities of daily living; (b) pain VAS scores (range 0–100) of ≤40 versus >40, indicating moderate pain; (c) frequency of physical exercise of ‘1 or more times weekly’ versus ‘less than once weekly’; (d) current smoking status, analysed as yes or no. Multivariate models were analysed for physical function and pain as continuous variables, as well as according to clinical cutpoints that could highlight possible severe status, such as physical function of ≥1.0 versus <1 on a scale of 0–3, and pain of >40 versus ≤40 on a 0–100 VAS. Certain analyses were stratified according to age, and multivariate computations were adjusted for age, sex and type of health condition—acutely life-threatening versus non-acutely life-threatening or none.
Results
Overall mortality in the cohort
The mean age of the 1523 individuals in the study cohort was 55 years (range 30–91 years), and 72% were females. Among the 1523 subjects, 92 (6.0%) died over the subsequent 5 years. Eight of 25 health conditions were found to be associated with 5-year mortalities of 19% or more and were classified as ‘acutely life-threatening diseases,’ that is, coronary artery disease, other heart diseases, chronic kidney disease, chronic bronchitis, chronic leg ulcers, diabetes, cancer and stroke. The 17 other conditions with subsequent 5-year mortalities of 17% or less were classified as ‘non-acutely life-threatening diseases,’ that is, hypertension, peptic ulcer, inflammatory gut disease, asthma, thyroid disease, Parkinson's disease, epilepsy, other neurological diseases, chronic back pain, fibromyalgia, psoriasis, psychiatric diseases, alcoholism, osteoarthritis, musculoskeletal trauma, RA and ankylosing spondylitis.
The 92 deaths included eight of 429 (1.9%) who had reported no health condition, 21 of 728 (2.9%) with a non-acutely life-threatening condition, and 63 of 366 (17.2%) with one or more acutely life-threatening conditions (table 1) (some patients had two or three such conditions, so the total mortality was less than 19%). The eight subjects with no health condition and 21 with no acutely life-threatening conditions were pooled for further mortality analyses as 29 (2.5%) of 1157 subjects with no condition or no acutely life-threatening condition who died within 5 years. The mean baseline age of all patients who survived or died over the 5-year period was 54 and 75 years, respectively (p<0.001) (table 2), including 51 and 69 years in subjects with no conditions or no acutely life-threatening conditions (p<0.001), and 65 and 77 years in subjects with an acutely life-threatening condition (p<0.001).
Mean (SD) values for age, physical function and pain, and percentage of patients who exercise rarely or smoke, according to type of condition and vital status 5 years after baseline
Survival according to four medical history variables
Cumulative survival in the entire cohort differed according to physical function scores: 98% with scores <1 (on a 0–3 scale) survived versus 93% with scores ≥1 (figure 2). Survival was 99% in those with pain VAS scores ≤4 versus 97% in those with pain scores >4. Survival was >99% in those who exercised more than once weekly, 97% in those who exercised once weekly and 93% in those who did not exercise. Survival was 98% in non-smokers versus 95% in smokers (figure 2). Further analyses of survival according to each of the four variables are presented below.

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival for mortality according to (A) functional capacity (Health Assessment Questionnaire ≥1 vs <1), (B) pain (>4.0 vs ≤4.0), (C) frequency of physical exercise and (D) smoking status, over 5 years.
Physical function scores and mortality risk
The mean physical function scores were 0.27 (on a scale of 0–3) in all subjects, including 0.20 in those who survived and 1.4 in those who died over the 5-year period (p<0.001) (table 2). In the 1257 subjects with no conditions or no acutely life-threatening conditions, the mean physical function scores were 0.16, including 0.13 for those who survived and 1.1 for those who died (p<0.001) (table 2). In the 366 subjects with acutely life-threatening conditions, the mean physical function scores were 0.63, including 0.45 in those who survived and 1.5 in those who died (p<0.001) (table 2). The HR and 95% CI for mortality over 5 years for physical function scores ≥1 (on a scale of 0–3) were 3.5 (95% CI 2.1 to 5.1) for all subjects, 4.5 (95% CI 1.6 to 12.6) for those with non-acutely life-threatening conditions and 3.1 (95% CI 1.8 to 5.5) for those with acutely life-threatening conditions (table 3).
HRs (95% CI) for 5-year mortality in older general population: analyses adjusted for age and sex
Pain scores and mortality risk
The mean pain score was 20 (on a scale of 0–100) in all subjects, including a mean level of 19 in those who survived compared with 38 in those who died over the next 5 years (p<0.001) (table 2). The mean pain score in individuals with no condition or no acutely life-threatening condition was 16, including 16 in those who survived compared with 27 in those who died (p=0.020) (table 2). The mean pain score in subjects with an acutely life-threatening condition was 34, including 32 in those who survived compared with 43 in those who died over the next 5 years (p=0.008). The HRs (with 95% CI) for mortality over 5 years if pain scores were >40 compared with ≤40 (on a scale of 0–100) were 2.2 (95% CI 1.3 to 3.5) for all subjects (table 3) and 3.1 (95% CI 1.2 to 8.3) for those with non-acutely life-threatening conditions, but 1.5 (95% CI 0.9 to 2.8) for those with acutely life-threatening conditions, not meeting the p<0.05 criterion (p<0.16).
Exercise frequency and mortality risk
Among all individuals, 28% exercised less than once per week, including 26% of those who survived and 76% of those who died over the 5 years (table 2). Among subjects with no conditions or no acutely life-threatening conditions, 25% exercised less than once per week, including 24% who survived versus 63% who died (table 2). Among subjects who had an acutely life-threatening condition, 40% exercised less than once per week, including 33% who survived and 82% who died. The HRs (with 95% CI) for death over 5 years among subjects who exercised less than once per week compared with those who did exercise at least once per week were 5.2 (95% CI 3.1 to 8.9) for all subjects, 4.9 (95% CI 1.8 to 13) for those with non-acutely life-threatening conditions and 4.7 (95% CI 2.3 to 9.6) for those who had an acutely life-threatening condition (p<0.001 for all comparisons) (table 3).
Smoking and mortality risk
Current smoking was reported by 17% of subjects, including 17% who survived versus 19% who died over the 5-year period (p=0.61) (table 2). Among those with no condition or no acutely life-threatening condition, 19% were smokers, including 18% who survived versus 28% who died (p=0.27). Among those who had acutely life-threatening conditions, 13% were smokers, including 12% who survived versus 15% who died (p=0.59). Among all subjects, people who smoked at baseline had a 4.6-fold higher HR (95% CI 2.5 to 8.6) of dying within 5 years compared with non-smokers (p<0.001), including a HR of 7.4 (95% CI 2.1 to 25) among people with a condition that was not acutely life-threatening and 3.3 (95% CI 1.5 to 7.3) among those who had an acutely life-threatening condition (table 3).
Multivariate Cox regression analyses
The four variables studied are not independent, and multivariate regression analyses were performed (table 4). In the entire cohort, physical function, exercise and current smoking were each significant independent predictors of 5-year mortality, while pain was not significant, that is, explained by the other variables (table 4). In individuals younger than age 55 who had no acutely life-threatening condition, pain and smoking were significant independent predictors of mortality, and physical function and exercise were not significant; in individuals younger than age 55 who had an acutely life-threatening condition, no medical history variable was significant in multivariate analyses (data not shown). In individuals aged 55 years and older who had no acutely life-threatening condition, functional status was the only significant predictor of mortality, whereas both functional status and lack of exercise (but not pain or smoking) were independent statistically significant predictors in individuals over age 55 who had an acutely life-threatening condition (data not shown).
Multivariate model: HRs (95% CI) for 5-year mortality
Discussion
The results confirm and extend a number of reports (only some of which are cited here) that poor physical function,1–7 pain,3 8–10 limited exercise11 12 and smoking14 predict premature mortality. Smoking14 and limited exercise11 12 29 are more widely recognised as predictors of premature death than poor physical function2 7 and pain.3 9 10 Nonetheless, these four medical history variables usually are not collected in everyday medical care—even smoking status often remains unknown,30 although some evidence of improvement has been reported.31 By contrast, variables from sources other than the medical history with similar prognostic significance for premature mortality—such as blood pressure and cholesterol—are collected rigorously in most clinical care and health maintenance settings.
The new information presented here is that prognostic quantitative data concerning physical function, pain, exercise status and smoking can be collected in a format found on a one-page (two-sided) self-report MDHAQ (figure 1), which has been completed by all patients seen by the authors at all visits in the infrastructure of usual care for 20–30 years,18–21 and in many other settings. This questionnaire is given to each patient to complete upon registration for a visit and easily completed by patients in 5–10 min, so that collection of the medical history variables involves no additional effort on the part of a health professional or office staff.32 The MDHAQ can be adapted to any clinical, health maintenance or research setting, and can be completed at home.
In the reported cohort of 1523 older people from the general Finnish population, survival was 93% in subjects who reported poor physical function or limited exercise, compared with 95% in smokers, 97% in those who reported pain, and 91% in those who reported hypertension, versus 98–99% in other subjects. It could be suggested that one or more of the four patient history variables, which are correlated with one another, might not be necessary in clinical care. However, clinical care of individual patients necessarily addresses multiple variables that might be correlated significantly but may each contribute incrementally to a poor outcome—for example, blood pressure, cholesterol or glucose.33 The possible independent contribution of poor physical function, pain and limited exercise, as reported in the simple self-report MDHAQ format, to higher mortalities remains to be characterised further.
Physical function, pain, exercise status and smoking may be regarded as ‘vital signs’ from a medical history for chronic diseases and health maintenance, analogous to traditional vital signs in acute care, such as pulse and temperature. Pain34 35 and smoking status14 have been advocated as ‘vital signs’,13 introducing a concept that a vital sign may be derived from a medical history, rather than from physical examination.
Vital signs often confirm impressions of the clinician but also provide standard quantitative data, which may be regarded as a type of checklist36 37 to be monitored from one encounter to another more accurately than through narrative descriptions. Vital signs that identify risk of premature mortality may provide data to analyse whether interventions to improve variables such as physical function or pain will improve survival, as seen for exercise, smoking, blood pressure and cholesterol. It may also be desirable to include these medical history variables in research and clinical analyses of any risk factor for long-term mortality, to ascertain the extent to which they may modify biomedical, genetic and physiological risk factors in prediction of long-term mortality.
There are several limitations to this study. No laboratory tests were available—it might be of considerable interest to compare these medical history variables with laboratory tests, such as serum cholesterol, in the prognosis of mortality, and whether a component of the risk may be explained by one or more of the reported medical-history variables. All subjects were from Finland, although most data suggest that mortality experience in Finland is similar to that found in most Western countries, and reports from many countries have indicated that each of these variables is prognostic of premature mortality. Furthermore, a 76% response rate to a mailed questionnaire is unlikely in locations outside Finland. Diagnoses were available only from self-report, which can be inaccurate for certain diagnoses.38 Nonetheless, most of the excess risk according to these medical history variables was not seen in patients with acutely life-threatening diseases, which ironically may be over-reported in many situations.
In conclusion, poor physical dysfunction, pain, limited exercise, and smoking may be identified in a general population as risk factors for premature mortality in a standard systematic format on a simple patient self-report MDHAQ that has been completed at every visit of every patient to the authors for 20–30 years. This questionnaire can be completed before any visit in usual care, health maintenance or clinical research, so the information is available for clinical care. More information concerning possible modification of these risk factors through therapeutic intervention could advance the quality of life and longevity in many individuals and the general public.
References
Supplementary materials
Supplementary Data
Files in this Data Supplement:
Footnotes
To cite: Sokka T, Pincus T. Poor physical function, pain and limited exercise: risk factors for premature mortality in the range of smoking or hypertension, identified on a simple patient self-report questionnaire for usual care. BMJ Open 2011;1:e000070. doi:10.1136/bmjopen-2011-000070
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Ethics approval Ethical approval was provided by the Ethics Committees of Jyväskylä Central Hospital and Population Register Centre of Finland.
Contributors Supervision of data collection: TS; analyses: TS and TP; preparation of manuscript: TP and TS.
Provenance and Peer review Not commissioned; externally peer reviewed.
Data sharing statement De-identified data will be available to readers upon request.