Article Text

Abstract
Introduction Decision analysis is a quantitative approach to decision making that could bridge the gap between decisions based solely on evidence and the unique values and preferences of individual patients, a feature especially important when existing evidence cannot support clear recommendations and there is a close balance between harms and benefits for the treatments options under consideration. Low molecular weight heparin (LMWH) for the prevention of venous thromboembolism (VTE) during pregnancy represents one such situation. The objective of this paper is to describe the rationale and methodology of a pilot study that will explore the application of decision analysis to a shared decision-making process involving prophylactic LMWH for pregnant women or those considering pregnancy who have experienced a VTE.
Methods and analysis We will conduct an international, mixed methods, explanatory, sequential study, including quantitative data collection and analysis followed by qualitative data collection and analysis. In step I, we will ask women who are pregnant or considering pregnancy and have experienced VTE to participate in a shared decision-making intervention for prophylactic LMWH. The intervention consists of three components: a direct choice exercise, a values elicitation exercise and a personalised decision analysis. After administration of the intervention, we will ask women to make a treatment decision and measure decisional conflict, self-efficacy and satisfaction. In step II, which follows the analysis of quantitative data, we will use the results to inform the qualitative interview. Step III will be a qualitative descriptive study that explores participants’ experiences and perceptions of the intervention. In step IV, we will integrate findings from the qualitative and quantitative analyses to obtain meta-inferences.
Ethics and dissemination Site-specific ethics boards have approved the study. All participants will provide informed consent. The research team will take an integrated approach to knowledge translation.
- thromboembolism
- haematology
- health economics
- maternal medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The mixed methods approach will evaluate the application of decision analysis to shared decision making surrounding prophylactic low molecular weight heparin (LMWH) for women who are pregnant or considering pregnancy and have experienced a venous thromboembolism (VTE) for whom guidelines recommend a shared decision-making process regarding thromboprophylaxis.
Women who are pregnant or considering pregnancy and have experienced a VTE will be specifically targeted since guidelines recommend that treatment decisions regarding prophylactic LMWH be made using a shared decision-making process.
The integration of quantitative and qualitative research methods to evaluate a complex intervention will offer greater insights than either method alone.
A small sample size and the recruitment of participants from two high-income countries limits the generalisability of study findings.
The results of this pilot study will be used to inform a randomised controlled trial.
Introduction
Thromboprophylaxis during pregnancy
Venous thromboembolism (VTE) is a condition in which a blood clot forms in the deep veins of the leg, groin or arm (deep vein thrombosis (DVT)) and travels to the lungs (pulmonary embolism (PE)). Globally, VTE is a leading cause of maternal morbidity and mortality.1 2 In high-income countries, the incidence of VTE is 1.2 in 1000 pregnancies and deaths in 1.1 per 100 000 deliveries.3 Women with prior VTE are at an increased risk of thrombosis during subsequent pregnancies,4 5 although the magnitude of this risk remains uncertain given that the existing evidence base is informed by studies with major limitations.6
Because it does not traverse the placenta and is associated with a low risk of heparin-induced thrombocytopaenia and osteopaenia, low molecular weight heparin (LMWH) represents the preferred treatment option for the prevention of VTE during pregnancy over other antithrombotic therapies, such as unfractionated heparin.7–9 It is, however, expensive and requires daily subcutaneous injections.10 Prophylactic LMWH may be associated with an increased risk of major bleeding, especially around the time of delivery and may limit access to regional analgesia.7 11 There continue to be challenges in determining the appropriate pregnancy-specific dose and role of laboratory monitoring.
Due to uncertainty regarding available evidence as well as the costs associated with administration and monitoring, the American Society of Hematology recommends that the decision between prophylactic LMWH during pregnancy versus expectant management involving no LMWH be made using a shared decision-making process.9 The use of decision aids is suggested for this type of conditional recommendation (ie, recommendation based on weak evidence) as they may help individuals make decisions consistent with their risks, values and preferences. Despite this call for shared decision-making, a paucity of decision support tools exist to help patients engage in treatment decisions for VTE.12
Shared decision making and the clinical encounter
Shared decision-making is a continuum process through which patients and clinicians work together to make a treatment decision.13 Although there is no consensus regarding the definition of shared decision-making,14 three elements are considered necessary: (1) recognising a decision is required; (2) knowing and understanding the best available evidence; and (3) incorporating patient values and preferences into the decision.15 Although a key element is the incorporation of patient values and preferences into the decision,15 studies indicate they are often ignored or poorly understood by providers.16 17
A number of decision support technologies to facilitate shared decision-making exist. Decision aids are the most commonly used tool. Available in a variety of formats (eg, online, print and video), decision aids are meant to inform patients regarding treatment options and their associated potential benefits, harms and costs.18 19 These tools often entail an implicit method of values clarification, in which patients are encouraged to think about what’s important to them.20 A systematic review of 105 randomised controlled trials involving 31 043 patients found that, while decision aids helped patients make more informed decisions,21 there is uncertainty as to how these tools support the process of integrating patient values and preferences into the decision-making process.
The International Patient Decision Aid Standards Collaboration recommends that decision aids include a value elicitation exercise alongside the presentation of evidence.22 A variety of methods can help patients appraise their values regarding treatment options under consideration. For example, patients can complete a ranking exercise to express the relative importance of each outcome. Although eliciting patients’ values is important, it does not ensure that they are incorporated into the decision-making process. Furthermore, patients and providers then face the cognitive challenge of weighing the harms and benefits of each treatment option alongside their probabilities of occurring and the patient’s values and preferences.23–25
Decision analysis
Decision analysis is a decision support technology that could bridge the gap between decisions based solely on evidence and the values and preferences of individual patients. It involves structuring a decision problem using an analytical framework (eg, decision tree) that includes key clinical outcomes associated with each treatment option as well as the natural course of untreated illness along with their associated probabilities and utilities or other weighting factors based on patients’ values and preferences. Probabilities, a measure of likelihood that an event will occur,26 are obtained from published studies and may themselves be personalised based on individual patient’s clinical risk profile. Values and preferences for health outcomes, which are expressed as health utilities, can be obtained directly from patients.27 Utility assessment involves comparisons to anchor health states (ie, perfect health and death) and may involve gambles that entail a risk of undesirable outcomes, or trade-offs between quality and quantity of life. Utility scores can be elicited directly from patients using exercises such as the standard gamble, time trade-off and visual analogue scale.28 Utility scores typically are anchored 1 representing ‘perfect health’ and 0 representing the ‘dead’ state. Utility scores can be used in a personalised decision analysis to calculate the quality-adjusted life years (QALYs) for each treatment option under consideration. For example, if a treatment results in a life expectancy of 10 years, but the quality of life for the resulting health state has a utility of 0.9, the treatment would yield 9.0 QALYs. If multiple treatment options are being considered, the treatment with the highest quality-adjusted life expectancy represents the best option.27 Thus, patient-specific probabilities and utility scores can be used in a decision analysis to calculate personalised results and obtain an explicit guidance statement to facilitate decision making.29 30
Decision analysis for shared decision making
Several studies found a disagreement between the results of the decision analysis and treatment guidelines.31–33 This suggests that guidelines, despite including a range of inputs (clinical evidence and patient preferences) and potential outcomes, might not adequately respond to individual patient treatment decisions.
Current evidence, although limited, shows the potential for personalised decision analysis to improve shared decision making in clinical contexts.31–41 While decision analysis is increasingly being used to inform the management of pregnancy-related conditions,42 its use is fraught with challenges. These include competing interests of mother and fetus, the use of appropriate time horizons and challenges with using QALYs as an outcome measure for combined maternal–fetal health states.43 As a result, it is unclear how or if decision analysis should be incorporated within shared decision making surrounding VTE and pregnancy, which necessitates a robust approach to shared decision-making given the close balance between benefits and harms of LMWH and limitations of available evidence.
Objective
The objective of this study is to explore the application of decision analysis to a shared decision-making process for the decision of using prophylactic LMWH for pregnant women or those considering pregnancy who have experienced a VTE. The study will also inform the design and execution of a future randomised controlled trial that will evaluate the additional value of decision analysis in the clinical encounter for the same decision.
Methods and analysis
In this study, we will use an explanatory sequential mixed methods design, which consists of quantitative data collection and analysis followed by qualitative data collection and analysis. This type of study design will allow for a comprehensive evaluation of decision analysis within a shared decision-making encounter for VTE and pregnancy.
In a mixed methods study, separate research questions are specified for the quantitative and qualitative components of the study, as well as an overarching mixed methods question.44 The following research questions will guide the conduct of this study:
Quantitative research question
Using a shared decision-making process that incorporates decision analysis, what is the level of decision quality among women that are pregnant or considering pregnancy who have experienced VTE and must decide whether to take LMWH?
Qualitative research question
What are the experiences and perceptions related to a shared decision-making process that incorporates decision analysis among women that are pregnant or considering pregnancy who have experienced VTE and must decide whether to take LMWH?
Mixed methods research question
How do the qualitative findings provide an enhanced understanding of quantitative results on decision quality to evaluate the application of decision analysis to a shared decision-making process among women who are pregnant or considering pregnancy and have experienced a VTE and must decide whether to take LMWH?
Figure 1 presents the study flow of this multicentre, single-arm, intervention pilot study. In step I, we will administer the intervention and measure decision quality among women who are pregnant or considering pregnancy and have experienced a VTE and must decide whether to take prophylactic LMWH. Step II follows the analysis of quantitative data, whereby we will use the quantitative results to inform qualitative data collection. In step III, we will conduct a qualitative descriptive study with all participants to explore their experiences and perceptions related to the intervention. In step IV, we will integrate findings from the quantitative and quantitative analyses to obtain inferences that add insight beyond what could be understood from either dataset on their own (meta-inferences).44

Study flow diagram for the DASH-TOP study. DASH-TOP, Decision Analysis in SHared decision making for Thromboprophylaxis during Pregnancy.
Step I: administration of intervention and quantitative data collection
Study design
In step I, we will ask women who are pregnant or considering pregnancy and have experienced VTE to participate in a shared decision-making intervention for prophylactic LMWH. The intervention will use a personalised decision analysis as a complementary approach to a decision aid. Since this study aims to pilot test the use of the decision analysis tool and explore preliminary findings, a control group was not included because the study was not designed to compare effects between intervention and control groups.
Study setting
The study will recruit women from hospitals in Canada (n=2 sites) and Spain (n=4 sites). The decision to conduct an international study was made in consideration of the small size of the target population. Since it is estimated that complications due to VTE occur in approximately 1 in 1000 pregnancies,45 an international study will increase feasibility of recruitment and generalisability of results.
In a previous study conducted by the research team, we compared the use of direct choice and decision analysis among 123 women with a history of VTE who were pregnant or planning pregnancy. During this study, we observed some differences between countries, including Canada and Spain.46 Given that the research teams in these two countries have conducted similar studies together and staff at the selected study sites are already trained, these two countries were selected for the pilot sites.
Participants
The target population consists of women with a prior VTE who are pregnant or planning pregnancy and who have been referred for counselling regarding prophylactic LMWH. Women will be eligible for inclusion if they have a history of lower extremity DVT or PE, are currently pregnant or planning pregnancy and considering LMWH. Women will be excluded from the study if they are currently receiving thromboprophylaxis or therapeutic anticoagulation, are less than 18 years of age, have contraindications or intolerances to LMWH, or are unwilling and/or unable to provide informed consent. At each site, the clinician will review medical charts to identify eligible women based on their pregnancy status and presence of a previous blood clot. The clinician will contact potential participants and ask if they are willing to be approached by a member of the research. With the woman’s permission, the research team will contact the woman by telephone to explain the study, confirm eligibility and schedule the interview.
Since greater priority will be given to the qualitative component of this mixed methods study, the sample size will be determined in consideration of the amount of information required to address the qualitative research question.47 There are no formal rules for calculating a priori a sample size for qualitative studies, instead an estimate of the number of participants required is provided. We have estimated that we will need an initial purposeful sample of 30 women (n=5 per site) given that this is a fairly homogenous population of women with respect to their medical diagnoses and who are making these decisions within pregnancy. However, as data collection and analysis is concurrent in qualitative studies, if we determine towards the end of our recruitment that certain concepts are not fully saturated, then the decision will be made to continue recruitment until we reach saturation or ‘the point at which the data collection process no longer offers any new or relevant data’.48
Intervention
The intervention will explore the decision-making process comparing strategies of administering prophylactic LMWH once daily when pregnancy is confirmed and continuing until delivery7 versus expectant management without LMWH. The intervention has been designed with three components: a direct choice exercise, values elicitation exercise and personalised decision analysis. All participants in the study will receive the intervention. A member of the research team will deliver the intervention and collect data in person or online using a web-based platform. The process is expected to take between 1 and 1.5 hours. Through this interview, some women may find the additional counselling and information received helpful in making their decision about the use of LMWH. All women will participate in the study prior to meeting with their healthcare provider so that they can apply this new information to their decision and follow-up with a healthcare professional if they have any questions. We do not anticipate there is any risk associated with this interview in general nor with the length of time required to complete the interview; however, we do inform participants that they can stop participation at any point during the intervention and are free to not respond to questions they are uncomfortable with.
To start, women will be asked to consider four health states relevant to this decision: (1) use of LMWH; (2) major obstetrical bleed; (3) DVT; and (4) PE. Health state descriptions are available in online supplemental appendix 1. Women will then complete a direct choice exercise that includes the review of an interactive electronic decision aid developed using the MagicApp platform.49 The decision aid describes the harms and benefits of LMWH for prevention of pregnancy-related VTE. In line with International Patient Decision Aid Standards (IPDAS) recommendations, information is presented in numeric and graphic format.22 Figure 2 presents a screenshot of the decision aid.
Supplemental material

Screenshot of decision aid. This screenshot presents women with their estimated risk of experiencing a deep vein thrombosis (DVT). Risks are presented in both numerical and graphical format. Numerically, the risk of DVT during pregnancy is 5.5%. This means that, out of 1000 women, approximately 55 will experience a DVT if they do not take low molecular weight heparin (LMWH) and 9 will experience a DVT if they do take LMWH. Overall, 46 fewer women will experience a blood clot when taking LMWH compared with not taking LMWH. The graphic represents a room of 1000 women. The 945 figures who are coloured in grey represent those women who were not destined to experience a DVT and would take daily injections of medication for the rest of their pregnancy with no benefit. The nine black figures represent women who will take the medication regularly and still experience a DVT during pregnancy because LMWH is not 100% effective. The orange figures represent the 46 women who would have experienced a DVT in their pregnancy and will avoid the blood clot because they took LMWH. The overall certainty of the evidence informing these estimates is low due to the types of studies that were conducted and the small sample sizes.
The direct choice exercise will be followed by three value elicitation exercises (rank ordering, visual analogue scale and standard gamble)50 that will be completed using Gambler II software.51 Women will consider the four health states listed above. For the ranking exercise, women will rank the health states from most to least preferred. For the visual analogue scale, women will place each health state along a ‘feeling thermometer’ that represents their preference on a scale of 0 (dead) to 100 (perfect health). Figure 3 presents a screenshot of the visual analogue scale exercise. The standard gamble uses a poison pill analogy to describe a gamble in which the patient can accept an intermediate health state, such as a PE, or take a medication that can prevent that from occurring. The patient need only take a single pill from the bottle, but unfortunately some varying number of pills in the bottle are ‘poison’ and may result in death. If a patient is indifferent between, for instance, a 0.1 risk of getting a poison pill to avoid a PE and prophylactic LMWH, then the utility of that health state would be calculated as (1–0.1) or 0.9.35 Death will be used as the anchor for standard gambles relating to major obstetrical bleed, DVT and PE health states. In the standard gamble for the use of LMWH, DVT will be the anchor.

Screenshot of visual analogue scale. This screenshot demonstrates a visual analogue scale where participants are asked to place each health state along a ‘feeling thermometer’ that represents their preference on a scale of 0 (dead) to 100 (perfect health). In this hypothetical example, pulmonary embolism, deep vein thrombosis and major bleed are rated as 20, 30 and 50 out of 100, respectively.
The visual analogue scale and ranking tasks will serve as warm-up exercises, with the standard gamble determining the value rating inputted into the decision analytic model. The standard gamble is considered to be a gold standard in preference elicitation methods as it has demonstrated acceptability and reliability,52 53 as well as established theoretical underpinnings of expected utility theory.54 55 Unlike ranking and the visual analogue scale, it evaluates preferences under conditions of uncertainty.
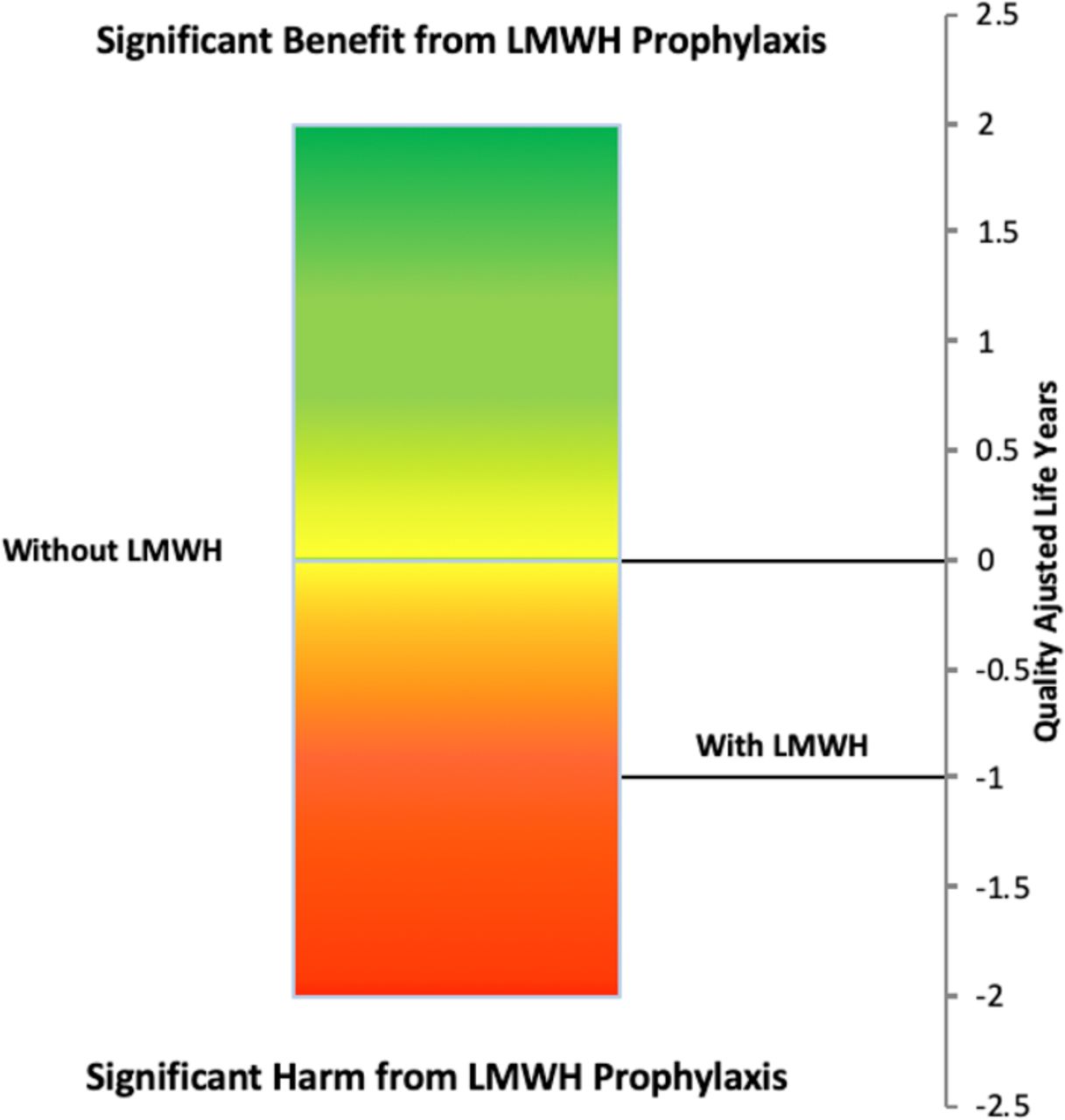
Once the utilities for a given patient have been obtained, they will be inputted into the decision analytic model along with patient-specific probabilities for VTE risk sourced from clinical guidelines.9 The decision analytical model is a Markov state transition model that examines two treatment options under consideration: prophylactic LMWH versus expectant management without LMWH.10 The model has a lifetime time horizon and a 6-week cycle length to simulate both antepartum and lifetime events. The model will be personalised according to women’s age and risk of VTE and utilities for each health state.56 57 Based on this information, the decision analytical model will estimate the QALYs for each treatment option. The treatment with the greatest expected QALYs will represent the recommended strategy. Figure 4 presents a screenshot of the decision analysis recommendation.

Screenshot of decision analysis recommendation. This screenshot shows how the personalised decision analysis results are presented to participants. In this example, the decision analytic framework calculated that the average quality-adjusted life year (QALY) expected for treatment with low molecular weight heparin (LMWH) was −1 compared with expectant management without LMWH. In this case, no LMWH would be the recommended strategy because it has the greatest expected QALYs and represents the treatment option that maximises the woman’s quality of life based on available clinical evidence and the patient’s preferences.
Data collection
At the start of the study, the research team will document women’s age, level of education, pregnancy status, pregnancy number, details regarding prior VTE (eg, type of event and presence of precipitating clinical risk factors), type and duration of treatment for prior VTE, and experience with LMWH (eg, bruising and heparin-induced thrombocytopaenia).
After completing the direct choice, values elicitation exercises and receiving the results of their personalised decision analysis, women will be asked to make a preliminary treatment decision. Women will make a final decision during the consultation with their provider. Women will complete a self-administered questionnaire to evaluate decision quality using the Modified Decisional Conflict Scale,58 Decision Self-Efficacy Scale59–61 and Satisfaction with Decision Scale.62 The Decisional Conflict Scale is a 16-item instrument that includes five subscales: informed, values, support, uncertainty and effective decision. Response options, which range from 0 for ‘strongly agree’ to 4 for ‘strongly disagree’, are combined into a summary score that ranges from 0 to 100, with 100 indicating an extremely high level of decisional conflict. The Decision Self-Efficacy Scale is an 11-item instrument that measures confidence or belief in one’s ability in decision making. Items are given a value between 0 and 4, with 0 indicating ‘not at all confident’ and 4 ‘very confident’. These values are combined into a summary score that ranges from 0 for ‘not confident’ to 100 for ‘extremely confident’. The Satisfaction with Decision Scale measures satisfaction with healthcare decisions. It is a six-item instrument that generates a summary score, ranging from 6 for ‘low level of decision satisfaction’ to 30 for ‘high level of decision satisfaction’. While it is acknowledged that these measures of decision quality have limitations,63 they are widely used and have been validated in different patient populations.58 64–68 Selecting three measures will provide a starting point for understanding different facets of the shared decision-making process. The self-administered questionnaire is available in online supplemental appendix 2.
Supplemental material
Data analysis
We will use descriptive statistics to summarise women’s age, level of education, pregnancy status, number and characteristics of previous VTE and experience with LMWH. We will assess decision quality using the scores obtained from the Decisional Conflict Scale, Self-Efficacy Scale and Satisfaction with Decision Scale. We will examine concordance between the woman’s decision regarding LMWH and recommendation from the personalised decision analysis.
Step II: integration of quantitative results and planning of qualitative data collection
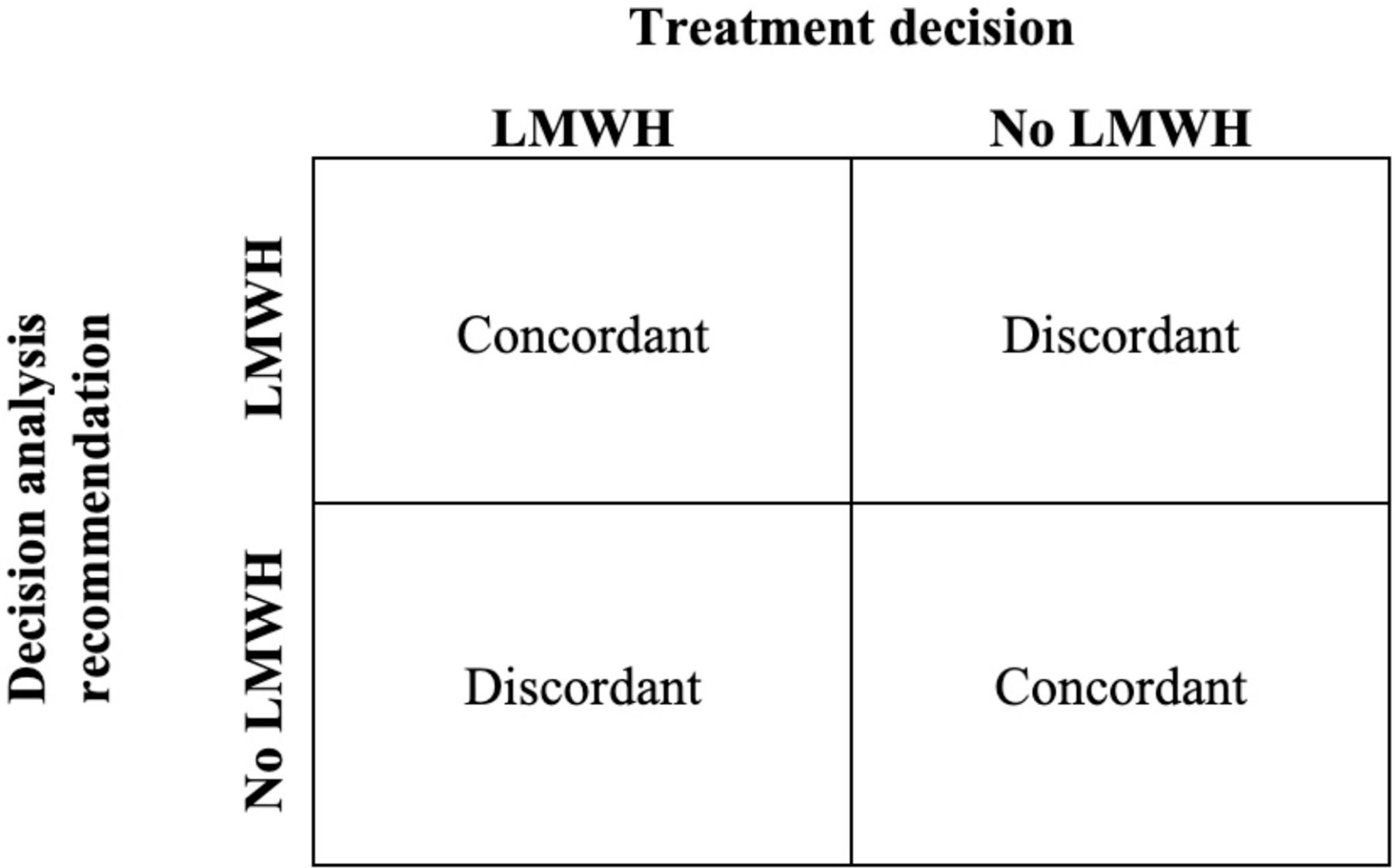
Based on the results of step I, women will be stratified into four categories according to their treatment decision (LMWH and no LMWH), decision analysis recommendation (LMWH and no LMWH) and the concordance/discordance between the two. Figure 5 presents the categorisation matrix. This is a form of integration in mixed methods research where one dataset (ie, quantitative) is analysed and used to inform subsequent data collection (ie, qualitative).69 The purpose is to identify what quantitative results need further explanation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Categorisation matrix based on quantitative results. LMWH, low molecular weight heparin.
Step III: qualitative descriptive study
Study design
Step III is a qualitative descriptive study that will occur after the quantitative component is complete. Qualitative description is a method of inquiry that explores individuals’ perceptions and experiences of a phenomenon.70 The aim is to generate rich and straightforward descriptions of an experience that is rooted in the language used by participants.71
Participants
After completion of the multicentre, single-arm, intervention study, all women will be invited to participate in the qualitative descriptive study.72 Women will be stratified into four categories according to their treatment decision, decision analysis recommendation and the concordance/discordance between the two.
Data collection
In-depth, semistructured interviews will be conducted to explore women’s experiences and perceptions as they relate to: (1) the decision-making process; (2) the direct choice exercise; (3) the personalised decision analysis; and (4) their knowledge of LMWH. Explicitly linking to the quantitative results, four versions of the interview guide have been designed to address women’s treatment decision, decision analysis recommendation and the concordance/discordance between the two. The interview guide was developed and tested by the research team, which comprised clinicians, patients and researchers with expertise in pregnancy-related VTE, shared decision making and qualitative methods. It is available in online supplemental appendix 3. A member of the research team will conduct the interviews, which will be audio-recorded and transcribed verbatim.
Supplemental material
Data analysis
Data from the interviews will be analysed using a method of thematic analysis. Thematic analysis refers to the systematic search for and identification of themes that are present in data.73 The aim is to obtain an understanding of a phenomenon by identifying themes or patterns through a process of coding.74 Given the exploratory nature of this qualitative descriptive study, there will be no predetermined coding scheme.
Two members of the research team with training in qualitative analyses will conduct the thematic analysis following the six-step approach outlined by Braun and Clarke75 (ie, familiarising with the data, generating initial codes, searching for themes, reviewing the themes, defining and naming themes and producing the final report). This process entails an iterative analysis within and across the transcripts of women from each of the four groups outlined in figure 5 to gain insight into why there is concordance/discordance between treatment decisions and decision analysis recommendations among pregnant women with a previous VTE.46
Looking for overarching themes and relations between them, the investigators will independently code a sample of the transcripts independently to generate an initial codebook and definitions. They will meet with a third study investigator to discuss emerging themes and definitions of codes until consensus on a codebook is reached. To ensure reliability, two team members will code the transcripts using this codebook. They will document and discuss any inconsistencies. NVivo software76 will facilitate this analysis. Qualitative data collection and coding will be conducted in the language of origin. Canadian and Spanish team members will work collaboratively on developing a single codebook for the Spanish and English analyses, discussing emerging themes and discrepancies as part of this process. An investigator with proficiency in English and Spanish will compare the summaries of findings and write a synthesis of themes that highlights important differences if they exist.
Step IV: integration of quantitative and qualitative findings
Once the quantitative and qualitative analyses have been analysed separately, the findings will be integrated using a joint display. A joint display is a table in which the quantitative and qualitative data are displayed alongside each other to enable an explicit comparison between datasets.44 This is a form of integration at the interpretive level, whereby each data set remains analytically separate from the other.77 The intent is to give a voice to study participants and ensure that quantitative findings are grounded in participants’ experiences.
The joint display will present each theme from the qualitative analyses according to the mean scores obtained from the Decisional Conflict Scale, Self-Efficacy Scale and Satisfaction with Decision Scale as well as the women’s risk of VTE, utility values, treatment decision and decision analysis recommendation. If there are any outliers or differences across groups, the integrated analyses will aim to explain these through qualitative data. For example, qualitative data can be used to explore any inconsistencies in utility values that are produced by the standard gamble and inputted into the decision analytic framework.
There are many reasons an inconsistency could occur. Pregnancy can be accompanied by extreme risk aversion,78 which could skew the standard gamble utility value and subsequent treatment recommendation. A qualitative evaluation of a shared decision-making intervention in atrial fibrillation reported that patients struggled to grasp the standard gamble concept,79 which could result in utility values that are not representative of patients’ preferences. By leveraging qualitative data on women’s experiences and perceptions of the intervention and decision-making process, integration will enable the research team to obtain meta-inferences and a deeper understanding of the application of decision analysis to shared decision making surrounding LMWH for pregnant women or those considering pregnancy who have experienced a VTE.
A joint display is an important tool for establishing the relationship between intervention effects and the patient experience. If the analysis identifies contradictions between quantitative and qualitative findings,80 we will verify the methodological rigour of each component of the study, the comparability of datasets and the delivery of the intervention.81 We will also consider how these contradictions can generate new research questions.82
Methodological rigour
Although an international study ensures feasibility of recruitment, it poses a challenge of maintaining consistency in data collection across sites. We have taken several steps in the planning of this study to mitigate this issue. At each site, we will have highly qualified personnel who have experience working on a shared decision-making project for VTE prophylaxis. Professional translation agencies have translated the scripts and interview guides developed in English into Spanish. Data collection materials have been tested with three to five patients at each site to ensure adequate understanding. To facilitate a standardised approach for administering the intervention, we have developed scripts based on feedback from patients, nurses and clinicians. All members of the research team will receive training on how to use required software programs.
Once recruitment starts, a range of strategies will be used to verify credibility (internal validity), dependability (reliability or consistency of findings) and confirmability (neutrality) of data. A list of these strategies is presented in table 1. Given the complexity of mixed methods research,83 the rigour of the quantitative, qualitative and mixed methods components of the study will be assessed separately.84
Checklist of strategies to ensure rigour in the conduct and reporting of the study
Patient and public involvement
Three patients (one from Spain and two from Canada) joined the study team as patient advisors. The Canadian Venous Thromboembolism Clinical Trials and Outcomes Research Network allowed our team to use their Partners Platform to recruit two Canadian patient-advisors. As part of this programme, patients receive training on how to participate in the research process. For the Spanish site, a patient who is also nurse at one of the participating hospitals was asked to participate as an advisor.
The three patient advisors matched inclusion criteria for the study. They reviewed all study materials and met with the research team to provide feedback on the study design, intervention, scripts and data collection materials. The development of the qualitative research questions and selection of quantitative outcome measures were directly informed by these patients’ priorities, experience and preferences. An additional five patients participated in preliminary testing of the intervention to provide feedback on the overall research process and ensure adequate understanding.
Patients will not be directly involved in the recruitment and conduct of the study. The results of the decision analysis will be communicated with patients participating in the study. Additional study materials (ie, print outs of decision aid and health state descriptions) and published results will be made available to participants on request.
Ethics and dissemination
Site-specific ethics boards have approved the study.
This study takes an integrated approach to knowledge translation that applies the principles of knowledge translation to the entire research process.85 Eight patients have contributed to the design and prepiloting of data collection materials. We will publish findings in peer-reviewed journals and present at key conferences, including meetings of the American Society of Hematology, International Society on Thrombosis and Haemostasis, Society of Medical Decision Making and Guidelines International Network. We will also disseminate results within the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) community.
Acknowledgments
The authors wish to acknowledge and thank the the patient advisors who contributed to the design of the study and testing of the data collection materials.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @fengxie_mac
Contributors The study concept and design were conceived by FX, PA-C, GG, SB and ME. ME developed the intervention, with support from FX, PA-C, BH, ML-G and SB. BH developed the data collection materials and plan for data analyses, with support from FX, PA-C, GG, ME, ML-G, SB, RD, NS and SJ. BH prepared the first draft of the manuscript. All authors have reviewed the manuscript for critically for important intellectual content and offer final approval.
Funding BH received a doctoral award from the Canadian Institutes for Health Research (Grant number: GSD – 152327). The study is partially funded by the Spanish Public Research Institute – Health Institute Carlos III (Grant number: PI17/01874).
Competing interests ME has received grant funding from the National Institutes of Health (Eunice Kennedy Shriver National Institute of Child Health and Human Development, and National Center for Advancing Translational Sciences) and funding for investigator-initiated research from Bristol-Myers Squibb. RD has received speaking honoraria and grant funding from Ferring Inc and an early career grant from the Canadian Institutes for Health Research for projects unrelated to this study. NS has received honoraria and an educational grant from Sanofi. ML-G receives doctoral support from the Spanish Public Research Institute – Health Institute Carlos III. SB has acted as a consultant for Leo Pharma Canada (manufacturer of low molecular weight heparin) and receives unencumbered salary support through the McMaster University Eli Lilly Canada-May Cohen Chair in Women’s Health.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.