Article Text

Abstract
Introduction A new health state classification system has been developed for dental caries - Dental Caries Utility Index (DCUI) to facilitate the assessment of oral health interventions in the cost-utility analysis (CUA). This paper reports the protocol for a valuation study, which aims to generate a preference-based algorithm for the classification system for the DCUI.
Methods and analysis Discrete choice experiments (DCEs) will be conducted to value health states generated by the DCUI classification system and preferences for these health states will be modelled to develop a utility algorithm. DCEs produce utility values on a latent scale and these values will be anchored into the full health-dead scale to calculate the quality-adjusted life years in CUA. There is no previous evidence for the most suitable anchoring method for dental caries health state valuation. Hence, we will first conduct pilot studies with two anchoring approaches; DCE including duration attribute and DCE anchoring to worst heath state in Visual Analogue Scale. Based on the pilot studies, the most suitable anchoring method among two approaches will be used in the main valuation survey, which will be conducted as an online survey among a representative sample of 2000 adults from the Australian general population. Participants will be asked to complete a set of DCE choice tasks along with anchoring tasks, basic social-demographic questions, DCUI, a generic preference-based measure and oral health quality of life instrument.
Ethics and dissemination Ethical approval for this study was obtained from the Human Research Ethics Committee, Griffith University (reference number HREC/2019/550). The generated algorithm will facilitate the use of the new dental caries preference-based measure in economic evaluations of oral health interventions. The results will be disseminated through journal articles and professional conferences.
- health economics
- oral medicine
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The protocol has been developed for a valuation study, which aims to generate a preference-based utility algorithm for a new health state classification system for dental caries.
Since there is no previous evidence for the most suitable anchoring method for dental caries health state valuation, pilot studies with two anchoring approaches (DCE including duration attribute and DCE anchoring with Visual Analogue Scale) have been planned prior to the main valuation survey.
The most suitable valuation approach identified based on the pilot studies will be applied as the main valuation survey to generate the utility algorithm.
The generated algorithm will facilitate the use of the new dental caries preference-based measure in economic evaluations of dental caries interventions.
Health states defined by the classification system will be valued by the adult general population sample. The methodological constraints associated with conducting health state valuation studies among the paediatric population, limit the ability to value health states with an adolescents sample.
Introduction
Health economic evaluations play a vital role in assessing healthcare interventions by providing information on which interventions provides the best value for money.1 2 Cost-utility analysis (CUA) is a preferred type of health economic evaluation by many Health Technology Assessment authorities across the world.3 4 The CUA compares interventions in terms of their incremental cost per unit of outcome5 and quality-adjusted life years (QALYs) is the most common form of outcome measure in CUA.5 The QALY incorporates both quantity and quality of life as a single summary outcome measure. The use of QALY as a summary outcome measure allows CUA to compare health interventions across different diseases.5
The calculation of QALYs relies on health state utility values (preference weights) assigned to the health states in the condition of interest.6 Preference-based quality of life measures (PBMs) are used to calculate utility values for QALYs in economic evaluations. PBMs are patient-reported outcome measures that consist of a health state classification system and a set of health state utility values corresponding to each of the health states defined by the classification system.7 8 They are pre-scored, readily available and easy to use rather than the directly eliciting preferences from patients.9 There are two types of PBMs. Generic PBMs can be used for any health condition whereas condition-specific PBMs (CSPBMs) are tailored for use among patients with a particular disease or condition of interest.10 Generic PBMs such as the EQ-5D11 are widely used; however, they may not be sensitive to the changes in some disease conditions since they do not include all relevant dimensions for each disease.10 Condition-specific PBMs typically include the dimensions more relevant to a particular disease or condition, thus they may be more responsive to the changes of the disease/condition over time.8
Several oral health-related quality of life (OHRQoL) instruments have been developed and validated to date.12 13 However, none of them are preference-based, thus cannot be used to calculate utility weights for use in health economic evaluations.12 Due to the absence of a condition-specific PBM for oral health, researchers are limited to either elicit oral health utility scores via direct valuation methods14 and/or use a generic PBM measure15 in oral health interventions.16 Moreover, children and adolescents are the main focus of publicly funded oral healthcare services in many countries.17 They have a different perception about the impact of oral disease on their quality of life compared with adults. Therefore, the availability of paediatric condition-specific PBM for oral health will provide better information on how the disease and the oral health interventions affect the target group children and adolescents18 and will facilitate the use of CUA in assessing oral healthcare interventions more effectively. Furthermore, the majority of oral healthcare interventions among children and adolescents focus on dental caries since it is the most common chronic childhood oral disease.1 The development of a paediatric condition-specific PBM for dental caries is an important area of research in oral health.
Hence, in the first phase of this study (Hettiarachchi et al, submitted), we developed a classification system for dental caries - Dental Caries Utility Index (DCUI) based on a review of the literature, a series of qualitative interviews with adolescents and with expert opinion; these are accepted methodologies to develop a classification system for a CSPBM.7 10 The DCUI consisted of five items; pain/discomfort, difficulty eating food/drinking, worried, able to join in activities and appearance, with each item consisted of four levels (table 1). Considering that the mixed dentition period is over by the age of 12 years and those under the age of 12 years have less cognitive ability to understand the concepts and terms, we included adolescents above 12 years of age during the development of the classification system. Further, the Flesch-Kincaid Reading scores of the finalised instrument was 64.6, indicating that adolescents aged 12 to 13 years can easily understand the classification system. Thus, the target group of this instrument is adolescents above 12 years of age. This paper reports the protocol for a valuation study, which aims to generate a preference-based algorithm for the classification system for the DCUI. To do this, preferences for sets of selected heath states will be elicited that are then modelled to estimate weights for each attribute’s level to develop a utility algorithm. The algorithm will facilitate the use of DCUI in health economic evaluation of dental caries interventions among children and adolescents.
Dental Caries Utility Index (DCUI) classification system*
Methods and analysis
Preference elicitation technique
Different preference elicitation techniques have been adopted to elicit preference weights. The cardinal preference techniques such as standard gamble (SG) and time trade-off (TTO) produce utility values anchored by full health and death.19 However, over the recent past, ordinal preference elicitation methods such as discrete choice experiments (DCEs) and ranking orders have become widely used in health state valuations.19 A recent systematic review identified 63 health state valuation studies using DCEs and of them, 36 were published during 2016 to 2018.20 In a DCE study, participants are requested to state their preference for the series of choices between two or more alternative scenarios describing health problems.21 Best-worst scaling (BWS) is a ranking approach, in which participants are asked to state the best and worst from typically three or more sets of items or profiles.22 Compared with the traditional valuation methods such as SG and TTO,19 DCEs and BWS are typically conducted without an interviewer and compatible with the online surveys that expedites the data collection process.23 BWS provides additional information related to worst preferences compared with DCEs; however, previous studies demonstrated that DCEs performed better compared with BWS in health state valuations.24 Ordinal preference elicitation methods such as DCE and BWS produce utility values in a latent scale, thus it is important to anchor the utilities generated from these onto the full health to dead scale to calculate the QALY.25 Thus, health state valuations studies using DCE or BWS need to include anchoring tasks. In DCE approach, options such as DCE with duration (DCETTO) are available that can be used as a standalone valuation approach to test anchoring within the task. Considering all these facts, DCE approach will be used as the preference elicitation technique for the present study.
Anchoring methods
Different methods such as including duration as an additional attribute (DCETTO),23 mapping DCE into TTO, using hybrid models for DCE and TTO, anchoring the worst state using TTO,25 including immediate death in pairwise comparisons25 and anchoring with Visual Analogue Scale (VAS) have been considered for anchoring DCE values onto the full health to dead scale. The anchoring approaches that need data from separate TTO interviews among participants requires greater time and resources. Dental caries is generally not a life-threatening condition or associated with serious disabilities. Therefore, pairwise comparisons with death would also not be appropriate since dental caries health state would be predominantly the dominant choice over death or living in full dental health for a considerably shorter duration. DCETTO method is able to convert the latent utility values obtained from DCE to QALY scale while minimising the drawbacks with conventional TTO. The DCETTO method has been used for valuation studies26 27 and the methodology has been tested widely.27 28 Therefore, the DCETTO approach will be used as an anchoring approach for the valuation of DCUI. The VAS has been used in recent health state valuation studies29 to generate utility value sets. VAS includes a scale of a single line in which the top of the scale indicates the ‘best imaginable health’ and the bottom of the scale indicates ‘the worst imaginable health’. Individuals are asked to place the health state of interest on this scale.9 VAS is simple and easy to understand compared with the SG and TTO methods30 and does not attach any trade-off between life years. As mentioned earlier, dental caries is neither life-threatening nor associated with serious disabilities under normal circumstances. Therefore, anchoring with VAS would be an option for a disease condition in which participants will be reluctant to sacrifice life years for the quality of life.
Since there is no previous evidence to identify the most suitable anchoring methods for health state valuations in dental caries, it is worth exploring the two possible options; DCETTO and anchoring the worst health state with VAS. Therefore, we will first conduct two pilot studies with two DCE designs; DCETTO (valuation approach 1) and DCE with VAS (valuation approach 2) in order to identify the most suitable method among these two approaches, and this will then be used to generate the utility algorithm in the main valuation survey.
DCE experimental design and construction of choice sets
The DCUI instrument consisted of five items, each with four levels. Therefore, there are 1024 (45) possible health states for a full factorial design. As it will not be practical to value all possible combinations, a D-efficient design31 will be applied to select a subset of these health states while maximising the efficiency of the survey design. Two separate D-efficient designs with the model specification as multinomial model for valuation approach 1 and 2 (to be explained below) will be generated using Ngene software.32 As no previous studies valued dental caries health states derived from a classification system to determine the priors, zero priors will be assumed for all variables to generate the D-efficient designs. The number of choice tasks used in the previous health state valuations using DCE were ranged from 12 to 3160 and the majority of studies included more than 151 choice tasks.20 The number of choice tasks per respondent were ranged from 2 to 10820 to value health states derived from a classification system. For this study, eight choice sets per respondent are chosen and block design will be used with eight choice sets in 25 blocks to value 200 pairwise health states. The block design will ensure an equal number of respondents per block. In addition to these eight choice tasks per respondent, the DCE survey will be started, with a practice DCE choice task and a dominant choice question at the beginning of each block as an warm up task and to to allow respondents to be familiar with the DCE tasks.
Pilot study - DCETTO(valuation approach 1)
For the valuation approach 1, DCE choice tasks will include duration as an additional attribute (DCETTO choice tasks). Previous DCE studies in dental caries confined to the evaluation of treatment preferences or health services21 33 rather than the valuation of dental caries health states defined by a classification system. Therefore, no previous literature is available to determine the best levels for the duration attribute in the DCETTO for dental caries.
Dental caries is a chronic disease. Progression of dental caries depends on the balance between pathological factors, such as dietary sugars and bacterial count, and protective factors, such as fluoride and good oral hygiene.34 Thus, an assumption was made that the oral health status is constant over time and participants will be in the same caries state in the given duration when including the duration attribute to the choice tasks. Survival duration in the DCETTO could be interpreted as an equivalent to ‘marginal willingness to trade life years for an improvement in health status’.23 Therefore, it was decided to include 6 months, 1 year, 4 years, 7 years and 10 years as duration levels. Six months is included as it is recommended to visit the dentist every 6 months. 1 year, 4 years, 7 years and 10 years are included as these are the commonly used duration levels in conventional TTO tasks to calculate QALY.35 An example DCETTO choice task is given in table 2.
An example of a discrete choice experiment task including duration attribute for the valuation approach 1
Pilot study - DCE with VAS (valuation approach 2)
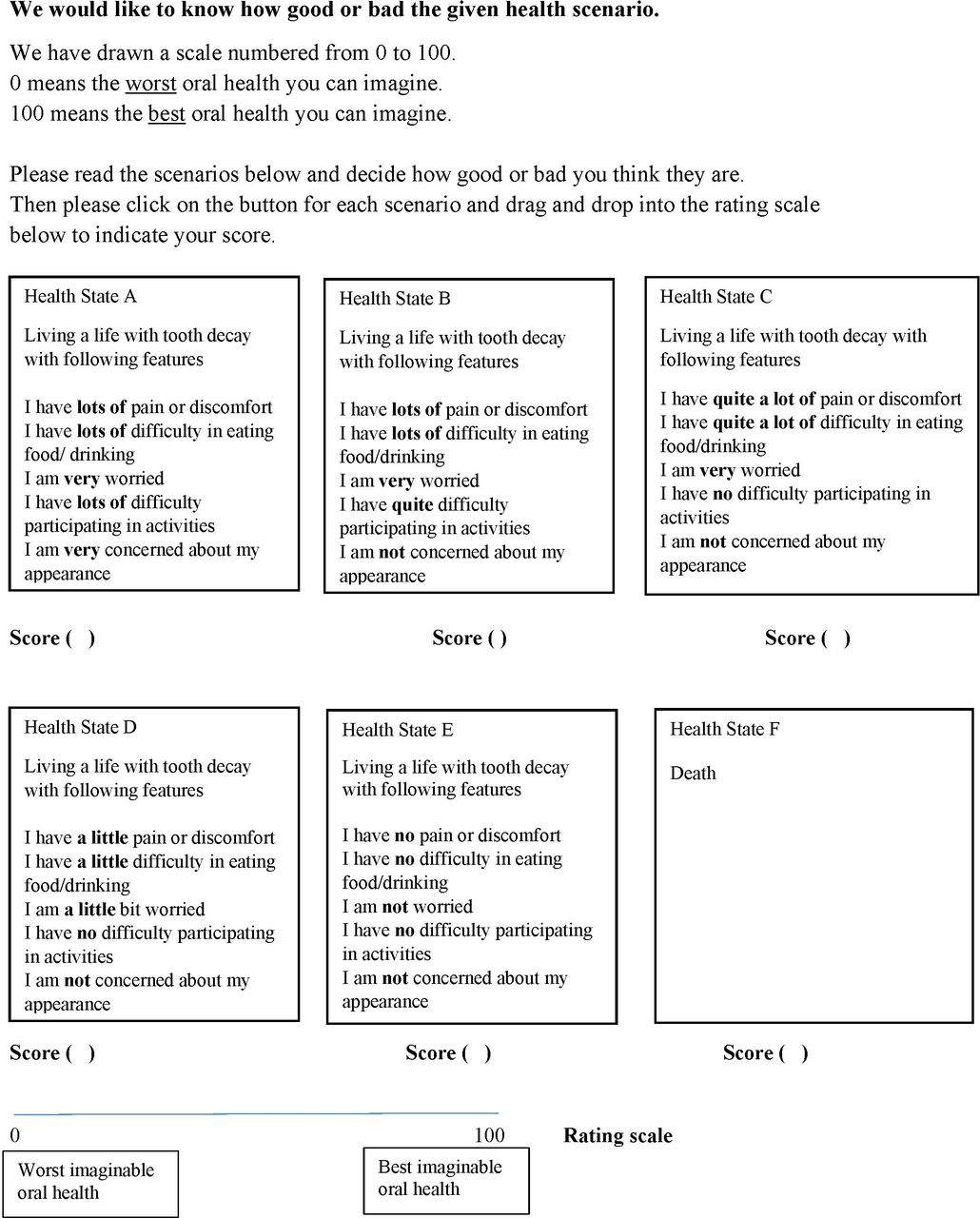
The valuation approach 2 will include DCE tasks without the duration attribute. An example of DCE choice task without the duration attribute is given in table 3. In addition to this, VAS tasks will also be included for anchoring. After DCE paired tasks, a VAS task will be included to value the best health state (11111), the worst heath state of the DCUI (44444), a mild health state, a moderate health state, a severe health state and death in a single VAS scale. The two extreme endpoints of the VAS scale indicate ‘best imaginable oral health’ (score 100) and ‘worst imaginable oral health’ (score 0). An outline of this task is given in figure 1.

{kind=link}
Visual Analogue Scale (VAS) task for the valuation approach 2.
An example of a discrete choice experiment task for the valuation approach 2
Further, for both pilot studies, questions will be added at the end of the DCE choice tasks to assess the difficulty in understanding the questions and difficulty in completing the tasks on a response scale of 1 to 4 (not difficult at all to extremely difficult). Time taken to complete the whole survey and each task based on the start time and end time will be assessed to check the feasibility and participant burden.
Main valuation survey
Based on the pilot studies, the more suitable anchoring method among these two approaches will be chosen and it will be used to generate a utility algorithm in the main survey conducted in the next phase of the study. In addition, these pilot studies will be used to assess whether the survey is launching in the way it is designed, to identify any practical issues or to identify changes required for the main valuation survey.
Study sample
There are arguments that continue to be held among researchers regarding ‘whose preference should be valued’36 for health state valuations of paediatric PBMs. Researchers have argued that the preferences of children and adolescents should be sought, since they have different preferences than adults, and it is them who are receiving the care.37 38 However, health state valuation among children is associated with methodological constraints, especially with anchoring tasks.36 These tasks would not only be a cognitive burden for children but there are also ethical issues associated with presenting ‘death’ to children. Thus, previous studies conducted to develop adolescent-specific algorithm followed different approaches. Child Health Utility-9D adolescent-specific algorithms39 were developed using two-steps; valuation tasks among adolescents and a separate TTO study with young adults group for anchoring. TTO tasks with adolescent-friendly wordings in face-to-face interviews were used to develop adolescent-specific algorithm for Assessment of Quality of Life (AQoL)-6D.40 However, it is common for child and adolescent health state values to be based on an adult general population sample or use proxy responses from parents/guardian.3 Most of the existing generic paediatric PBM valuation studies conducted with an adult general population26 36 41 as it is often public money that will be allocated to fund treatment and therefore it is the preferences of the public that matters. The present study is also planned to elicit preferences for health states from an adult general population sample; this is a highly feasible approach for generating health state values using an online sample.36
Sample size and recruitment
The calculation of sample size for DCE studies is often complex42 and researchers suggest different formulae based on several factors.43 Johnson and Orme44 suggest that the sample size (n) required for the main effects model is based on the number of choice tasks (t), the number of alternatives (a) and the number of analysis cells (c), which is equal to the largest number of levels for any of the attributes. Further, Johnson and Orme44 recommended a sample size of 300 as a rule of thumb for a quantitative study where there is no intention to compare subgroups and a minimum of about 200 per group for studies that plan to compare groups of respondents to be able to detect significant differences. Further, Lancsar and Louviere45 stated that 20 respondents per choice set would be sufficient to estimate a reliable model and a sample size of 1000 to 2000 will be able to produce small CIs.
Pilot study
Two pilot designs will be tested with an online sample of 400 representative adults (200 representative samples for each design) in Australia.
Main valuation survey
Based on the literature reviews and similar online surveys,39 42 our target is to include a sample size of 2000 representative respondents, which will be compatible with the above requirements for the main survey.
Administration of the survey
A representative sample of the Australian population in relation to gender and geographical area will be recruited from March 2020. Study participants will be recruited from an existing Australian online panel with the help of online research company SurveyEngine (http://trial.surveyengine.com/about.html). Around 86% of all households in Australia had access to the Internet at home in 2014 to 201546 indicating that online study has a good chance of reaching the target population. Potential participants (adults over 18 years old) who have registered in the online survey panel will receive the invitation for the study and interested participants will be provided the link to the survey. They will be guided through the online survey by screen prompts. The first section of the online survey will be the introduction page where participants will be given all the necessary details about the research project and contact details of the investigator if they need further clarification. Participants will be informed that the participation in this survey will be voluntary and the survey data will be anonymous and confidential. At the end of the introduction page, participants will be requested to provide their consent. Once the participant gives their consent, they will move to the next section and continue the rest of the survey. Consenting participants will be guided through the online survey by screen prompts and this will enable them to complete the tasks at their convenience. The next section of the survey will include screening questions (age, sex and which state they live in) followed by DCUI and a set of DCE choice tasks and anchoring tasks. Then the participants will be asked to complete a generic preference-based QoL instrument (the EuroQoL 5D 5L questionnaire - EQ-5D-5L),47 an OHRQoL instrument (Oral health impact profile-14 - OHIP-14)48 and questions regarding basic social-demographic characteristics, oral health status and frequency of dental visits. EQ-5D-5L and OHIP-14 are generic and OHRQoL instruments commonly used among Australian general population49 to assess generic and OHRQoL, respectively. The OHIP-14 has been shown adequate psychometric properties and validated extensively among both adults50 and adolescents population.51
Patient and public involvement
No patient involved.
Analytical plan
All data will be cleaned prior to the analysis and data will be analysed using Stata V.15.1.52 DCE data will be analysed using a conditional logit model under a random utility framework, which assumes that respondents choose the alternative that maximises their utility.53 The utility function consists of a vector of observable attributes as well as a random error term.19 Both the main effects and the interactions among attributes will be considered.
Pilot study - DCETTO(valuation approach 1)
The observable component (μij) of the utility function will be estimated using a conditional logit model as in Equation 1. The life years t will be included as a continuous variable.
 (1)
(1)
Uisj=Utility of the option j in choice set s for survey respondent i x=a vector contains five DCUI dimensions while each dimension is estimated using three dummy variables (with ‘no problems’ served as the reference level within each attribute).
t=life years
Anchoring results to a health utility scale will be performed based on the methodology described by Bansback et al.23 The objective is to derive the mean utility value of the state xij in DCE that correspond to a 10-year TTO value.
 (2)
(2)
 = value of the health state hj anchored on the health utility scale
= value of the health state hj anchored on the health utility scale
 = disutility of living with the health state hj for 1 year
= disutility of living with the health state hj for 1 year
 = coefficient represents the value of living in full health for 1 year
= coefficient represents the value of living in full health for 1 year
 = value for each health state
= value for each health state
Based on this formula, the sample mean DCETTO for the health state hj can be calculated from the coefficients of the conditional logit model.
Pilot study - DCE with VAS (valuation approach 2)
To obtain the coefficients in DCE latent scale, data from the DCE choice tasks in valuation approach 2 will be modelled with an appropriate regression model with the following specification. The best-fitted model will be selected based on the statistical significance of coefficients, the amount of explained variance and mean absolute error (absolute difference between the observed value and estimated value in each health state).
 (3)
(3)
μij = observable component of the utility function
x = vector contains five DCUI dimensions while each dimension is estimated using three dummy variables (with ‘no problems’ served as the reference level within each attribute)
β = coefficient for each dimension
Anchoring to the full health-dead scale of the VAS anchoring task will be performed based on the methodology proposed by Brazier et al30 and Rowen et al.25 Brazier et al30 proposed a formula (Equation 4) to convert the health state values in to full health-dead scale based on the value obtained for best health state and death from VAS health state valuation tasks and this has been used in previous studies.29 Raw VAS scores for worst heath state of the DCUI (44444), a mild health state, a moderate health state and a severe health state will be converted to full health-dead scale using Equation 4.
 (4)
(4)
Vh = adjusted VAS rating for health state h
Sh = respondent’s unadjusted VAS score for state h
Sdead = respondent’s assigned VAS score for the health state ‘death’
S11111 = respondent’s assigned VAS score for a state 11111 (best state)
Then the value of the worst state in the DCE model will be anchored based on anchoring with worst health states and with mapping DCE onto VAS. Rowen et al25 converted the coefficients on a latent utility scale estimated in DCE data onto the full health-dead scale using the estimated TTO value of the worst state. The same methodology would be followed here and based on the adopted formula (Equation 5) from Rowen et al,25 DCE data will be anchored to the worst state value obtained in VAS.
 (5)
(5)
βλӘ = rescaled coefficient for level λ of dimension Ә
wVAS = estimated VAS value for the worst state generated using equation 4 and 5
wDCE = DCE value for the worst state estimated using the DCE model
For the anchoring with mapping DCE onto VAS, mean VAS values obtained for the worst health state of the DCUI (44444), a mild health state, a moderate health state and a severe health state will be used as in Equation 6.


 (6)
(6)
VASj = mean VAS value of health state j
DCEj = modelled latent utility value of health state j
dVASj = disutility of the mean VAS value of health state j
dDCEj = disutility of the modelled latent utility value of health state j
ɛ = error term
Comparison of valuation approach 1 and 2 to assess the most suitable anchoring method for dental caries health state valuation
As these two DCE designs are different, they are not directly comparable. However, the pilot studies aim to identify the most suitable method for anchoring among these two approaches. Therefore, data from the two valuation approaches will be compared concerning the respondents’ self-reported difficulty of the tasks (based on the answers provided for the two questions - how difficult to understand the questions and how difficult to complete the tasks), dropout rate, time taken by each individual on the whole survey and for each DCE task.
Further anchored coefficients obtained from the valuation approach 1 and 2, as outlined in the analytical plan, will be examined for the sign and order of the coefficients; that is, the sign of the duration coefficient should be positive (since utility increase with the time living in full health) and levels in each domain should follow a logical order in which more severe should have larger utility decrement.
Main valuation survey
Once the most suitable valuation approach is decided based on the pilot surveys, that approach will continue as the main valuation survey to generate the utility algorithm. For the main survey, participants’ characteristics will be assessed and a χ2 test will be used to assess sample representativeness of the Australian general population. The EQ-5D-5L, OHIP-14, DCUI and self-reported oral health variables data will be analysed to assess the respondents’ QoL and oral health status. DCE tasks data of the main survey will be modelled based on the selected approach from the pilot study, as outlined in the analytical plan. The utility values generated from the main survey can then be used to calculate QALY in economic evaluation in dental caries interventions.
Ethics and dissemination
Ethical approval for this study was obtained from the Human Research Ethics Committee, Griffith University (HREC/2019/550). Informed consent will be obtained from the participants prior to starting the survey. Participants are only required to complete the survey; therefore, there is negligible or low risk for the participants. There are no potential adverse events/side effects. The research team will receive only de-identified anonymous data. The data obtained by this research project will be stored securely with a password-protected computer, and secure server in Griffith University until data will be destroyed after the 5 years minimum period of retention in accordance with University policy. Any personal details that will lead to the identification of individual participants will not be included in any report or publication arising from this research project. Dissemination of the study results will be through the publication of manuscripts in academic journals and conference presentations.
References
Footnotes
Twitter @ruvinihettiara
Contributors RH contributed to designing the study and draft of the article. SK, JB, BM, GC and PS contributed to the design of the study, editing and revising the article. All co-authors read and agreed the final version of the article to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.