Article Text

Abstract
Introduction Atherosclerotic intracranial artery stenosis (ICAS) is one of most common causes of stroke, which is the second-leading cause of death worldwide. Medical, surgical and endovascular therapy are three major treatments for ICAS. Currently, medical therapy is considered as the standard of care for most patients with ICAS, while extracranial to intracranial bypass is only used in rare situations. Balloon angioplasty alone, balloon-mounted stent and self-expanding stent, collectively called endovascular treatment, have shown promising potentials in treating specific subgroups of patients with symptomatic ICAS; however, their comparative safety and efficacy is still unclear. Therefore, a systematic review with network meta-analysis is needed to establish a hierarchy of these endovascular treatments.
Methods and analysis The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols was followed to establish this protocol. The search will be limited to studies published from 1 January 2000 to the formal search date. Major databases including Cochrane Library, MEDLINE, EMBASE, Chinese Biomedical Literature Database, conference proceedings and grey literature database will be searched for clinical studies comparing at least two interventions for patients with symptomatic ICAS. Primary outcomes include short-term and long-term mortality or stroke rate. Random effects pairwise and network meta-analyses of included studies will be performed on STATA (V.14, StataCorp, 2015). The surface under the cumulative ranking curve and mean rank will be calculated in order to establish a hierarchy of the endovascular treatments. Evaluation of the risk of bias, heterogeneity, consistency, transitivity and quality of evidence will follow the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions.
Ethics and dissemination Ethics approval is not needed as systematic review is based on published studies. Study findings will be presented at international conferences and published on a peer-reviewed journal.
PROSPERO registration number CRD42018084055; Pre-results.
- endovascular treatment
- balloon angioplasty
- balloon-mounted stent
- self-expanding stent
- intracranial artery stenosis
- network meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See:©http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- endovascular treatment
- balloon angioplasty
- balloon-mounted stent
- self-expanding stent
- intracranial artery stenosis
- network meta-analysis
Strengths and limitations of this study
To the best of our knowledge, this study will be the first systematic review and network meta-analysis of safety and efficacy of three subtypes of endovascular treatment for patients with symptomatic intracranial stenosis.
Besides randomised controlled studies, observational studies will also be included in order to obtain sufficient data for the network meta-analysis and improve the precision of estimates of adverse events.
The present study has a clearly established aim, state of the art methods for data collection, quality evaluation and quantitative synthesis.
The major challenge may come from unexpected heterogeneity from observational study designs. Stringent evaluation of transitivity will be conducted before data pooling for network meta-analysis.
Background
Description of the condition
Stroke is currently the second-leading cause of death just behind ischaemic heart disease, causing 6.2 million deaths in 2015 worldwide.1 2 Atherosclerotic intracranial artery stenosis (ICAS), one of most common causes of stroke, accounted for 10%–54% of all ischaemic strokes. Stroke mortality presented with regional variation, with a disproportionately high mortality in Asian countries, which might be partially attributable to higher prevalence of intracranial atherosclerosis in these regions.3 Great economic and family burden have been caused by stroke globally, especially in low/middle-income countries.4
Description of the intervention
Contemporary treatments for ICAS can be broadly categorised into medical, surgical and endovascular therapy. Currently, medical treatment remains the standard of care for patients with ICAS.5 Aggressive medical management (ie, dual antiplatelet therapy along with intensive modifiable risk factor management) is supported by the latest studies6–8 and recommended as the first-line therapy for symptomatic ICAS by the American Heart Association stroke prevention guidelines.9 Extracranial to intracranial bypass surgery (EC–IC bypass) has been used as treatment for ICAS since the 1980s, but it was proven to be associated with a worse prognosis versus medical treatment for patients with ICAS in a randomised controlled trial (RCT) published in 1985.10 Ever since, EC–IC bypass is used in very few situations, such as stenoses progressing to occlusions with major haemodynamic impairment or in non-atherosclerotic lesions like moyamoya disease.11 Endovascular therapy, also called percutaneous transluminal angioplasty and stenting (PTAS), was adopted from management of coronary heart disease and the first cases of its use in ICAS were reported in the 1980s.12 It was considered as a minimally invasive approach to treat patients with symptomatic ICAS and was found to have an acceptable periprocedural complication rate and potential benefit in initial studies.8 13 14 Although results of the Stenting versus Aggressive Medical Therapy for Intracranial Arterial Stenosis (SAMMPRIS) and the Vitesse Intracranial Stent Study for Ischemic Stroke Therapy (VISSIT) trials did not favour the use of PTAS in patients with ICAS, many neurovascular practitioners and academics still believe that there is a role for endovascular treatment of ICAS.15 Specific subgroups of patients, for example, African-American, Asian and Hispanic patients,16–19 are high-risk subgroup of patients who do not respond well to intensive medical treatment20 21 and patients with hypoperfusion symptoms,21 which still needs to be confirmed by future studies.
Rationale for the current systematic review
Endovascular therapy can be generally divided into three subtypes: balloon angioplasty alone (BA), balloon-mounted stent (BMS) or self-expanding stent (SES).22 So far, none of them have been established to be the primary option of endovascular therapy for specific subgroups of patients with ICAS. Early studies comparing BA with stent placement showed comparable recurrent stroke or mortality rate, but stent treatment showed a lower rate of postoperative residual stenosis.23 24 Comparable immediate procedural outcomes were reported by another study.25 A recent study, however, reported a significantly higher mortality (17.6% vs 8.4%, p<0.001) but no difference of iatrogenic stroke rate (3.4% vs 3.6%, p=0.826) in the BA group, compared with the stent group.26 Therefore, the safety and efficacy of BA versus stent placement is still unclear. As for the efficacy of BMS versus SES, the restenosis rate was showed to be higher in the SES than the BMS group.27–29 However, whether the other major complication rates are different between them still needs to be clarified. In summary, a systematic review with network meta-analysis that allows for both direct and indirect comparisons of multiple interventions is needed to decide the comparative effects of the three subtypes of endovascular therapy. To our knowledge, this kind of systematic review has not been previously completed.
Objective
The primary objectives of this study are to (1) determine both the safety and efficacy of different endovascular treatments (ie, BA, BMS or SES) on patients with symptomatic ICAS, and (2) establish a hierarchy of endovascular treatments for treating symptomatic ICAS, through a systematic review with network meta-analysis of randomised trials and observational studies.
Methods
This protocol was developed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) (see online supplement 1, PRISMA-P Checklist).30 This systematic review has been perspectively registered on the PROSPERO database (CRD42018084055, available at http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018084055). Any revision of this protocol and the whole review process will be updated timely on the PROSPERO registration. The conducting and reporting of this systematic review will follow the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions and the PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of healthcare interventions.31 32
Supplemental material
Criteria for considering studies for this review
Types of studies
RCTs and quasi-RCTs (non-blinded, interrupted time series) will be included. Observational cohort, case–control and registry studies will be included to obtain adequate statistical power, because rare outcomes will be included in our review and identifying these rare adverse events are important to assess the intervention safety, and RCTs lack adequate statistical power to evaluate these uncommon/rare safety outcomes due to type II (ie, false negative) error.33 Other types of studies including case series and case reports will be excluded. Studies published in Chinese journals will not be considered due to inappropriate randomisation procedures that have been reported in many of these studies.34
Types of participants
Patients with symptomatic ICAS and degree of stenosis more than 50% (verified by angiography) will be included. The stenosis is located in at least one major intracranial artery (intracranial internal carotid artery, vertebral artery or basilar artery and their major branches). Patients with ICAS with a transient ischaemic attack (TIA) or stroke are defined as symptomatic. A TIA was defined as a transient episode of neurological dysfunction (focal weakness or language disturbance, transient monocular blindness or required assistance in walking) caused by focal brain or retinal ischaemia that lasts for at least 10 min but resolves within 24 hours.35 ICAS related to the following factors will be excluded: arterial dissection, moyamoya disease, vasculitic disease, radiation-induced vasculopathy, fibromuscular dysplasia, sickle-cell disease, neurofibromatosis, suspected vasospastic process and suspected recanalised embolus.
Types of interventions
All competing interventions including any endovascular treatment as well as non-endovascular treatment strategy that can be administered for symptomatic ICAS are eligible for the analysis. Studies comparing at least two of the following eligible interventions will be considered in the analysis. We assume that any of the eligible interventions are, in principle, jointly randomisable among any patient that meets the inclusion criteria. If we identify any interventions that we are not aware of, we will consider them as eligible and include them in the network after assessing their comparability with those named below.
Interventions of direct interest
Studies that evaluated one or more of the following endovascular therapies namely BA, SES and BMS will be included. We will estimate the relative ranking of these interventions in the network meta-analysis according to primary outcomes.
Inclusion of additional interventions to supplement the analysis
Studies that evaluated non-endovascular treatment, namely medical treatment alone, and EC–IC bypass, will also be included to increase the amount of available (indirect) information in the analysis.
Types of outcome measures
Studies that reported at least one of the following outcomes will be included.
Primary outcomes
Short-term mortality or stroke rate (periprocedural or mean follow-up ≤ 3 months).
Long-term mortality or stroke rate (mean follow-up ≥ 6 months).
Secondary outcomes
Long-term restenosis (≥50% stenosis verified by angiography, mean follow-up ≥6 months).
TIA rate (short-term or long-term).
Other major complications.
Search methods for identification of studies
Literature search will mainly be executed in three databases: MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials. Search strategy has been drafted by an experienced librarian and revised by another librarian according to the Peer Review of Electronic Search Strategies checklist (see online supplement 2, Search strategy).36 The search will be limited to studies published from 1 January 2000 to the formal search date. In addition, we will also search other databases such as Chinese Biomedical Literature Database (CBM), Web of Science and Open Grey, and conference proceedings for relevant abstracts, the ISRCTN registry (http://www.isrctn.com), government registries (http://www.clinicaltrials.gov) and WHO registries (http://www.who.int/trialsearch/) for ongoing and recently completed studies. There will be no restrictions on study type, language or publication type. We will search the bibliography of all included studies and request original data from the primary authors when necessary.
Supplemental material
Data collection and analysis
Selection of studies
Two reviewers will independently complete the two levels of study screening and selection. In level one screening, reviewers will determine if a study is eligible for inclusion by screening the title and abstract of articles retrieved from the literature search. In level two screening, the full text of articles retained from level one screening will then be obtained and those that meet the eligible criteria will be included. When multiple studies report data from the same study population or multiple articles of the same study series are published in chronological order the study with the interventions of direct interest or the largest sample size will be retained. Before each level of screening, a pilot test, based on the predesigned test forms (see online supplement 3, Screening pilot-test form; adapted from Tricco et al 37), will be conducted to calculate inter-rater reliability and high agreement (≥80%) is required to launch the formal screening. Discrepancies between the two reviewers will be resolved by discussion or, otherwise, a third reviewer. In cases of any ambiguity or insufficient data, study authors will be contacted for further information.
Supplemental material
Data extraction and management
Similar with the screening process, data extraction will also be conducted by two reviewers, independently. A data abstraction form will be created in Excel and include two types of data:
Outcome data
Number of primary and secondary outcome events, total number of patients, the interventions being compared and follow-up duration will be extracted from included studies. Arm-level data will be extracted.
Data on potential effect modifiers
Data that may act as effect modifiers will be extracted from included studies, including: (1) study characteristics (eg, study design, volume of study centre, date of publication, journal of publication, study location(s), study funding); (2) population characteristics (eg, mean or median age, proportion of male patients, degree of preprocedural stenosis, functional status at presentation, medical history, drinking and smoking status, stenosis site of the intracranial artery); (3) intervention characteristics (eg, placement success rate, residual stenosis).
Also, a similar pilot test to calculate inter-rater reliability is required to confirm high agreement (≥80%) between two reviewers. Similarly, two reviewers will be resolve disagreements by discussion or, otherwise, a third reviewer. And we will contact study authors for further information in case of any ambiguity or insufficient data.
Assessment of risk of bias in included studies
Similarly, two reviewers will independently assess risk of bias, and conflicts will be resolved through discussion or, otherwise, a third reviewer. The risk of bias of RCTs and quasi-RCTs will be assessed with items in the Cochrane Collaboration’s tool,31 while that of non-RCTs (observational cohort and case-control studies) will be assessed with the Newcastle-Ottawa Scale (see online supplement 4, Newcastle-Ottawa Scale).38
Supplemental material
Measures of treatment effect
As primary and secondary outcomes are all dichotomous data, ORs will be used as the measure of treatment effect. Relative treatment effects will be presented as the summary relative effect sizes (ORs) and associated 95% credible intervals (CIs) for each possible pairwise comparison. Relative treatment ranking will also be estimated using the surface under the cumulative ranking curve (SUCRA) and mean ranks.39
Dealing with missing data
Some of the outcomes are assumed to be rare. Thus, zero events in one arm might be reported. In this case, 0.5 will be added to the numerator and one will be added to the denominator. Studies reporting zero events in all arms for primary outcomes will be excluded.40 41 When encountering missing data in the included studies, we will contact the study authors for these data first. If the data are still unavailable on requests, we will impute missing data using established methods, including informative missing ORs for dichotomous outcomes and informative missingness difference of means for continuous outcomes.42 43 Furthermore, a sensitivity analysis will be conducted to ensure that our imputations do not bias the final results.44
Assessment of clinical and methodological heterogeneity and transitivity
Across all eligible trials that compare each pair of interventions, descriptive statistics for potential effect modifiers described above (ie, study, population and intervention characteristics) will be generated. We will assess the presence of clinical and methodological heterogeneity both within and across treatment comparisons by calculating the I2 within each pairwise comparison.45 We will assess the assumption of transitivity across treatment comparisons by comparing the distribution of the potential effect modifiers across the different pairwise comparisons using boxplots or percentages.46 47 The above factors are ensured prior to conducting the following pairwise and network meta-analyses.
Data synthesis
As described above, if quantitative synthesis is not appropriate or the data are insufficient, the findings of our systematic review will be narratively reported. When quantitative analysis is plausible, the following pairwise and network meta-analyses will be conducted in STATA (V.14, StataCorp, 2015). We will first restrict our analysis to RCTs, then include data from quasi-RCTs and, finally, data from observational studies. This sequential approach of analyses will provide an understanding of the contribution of each type of study design to our summary estimates.
Methods for direct treatment comparisons
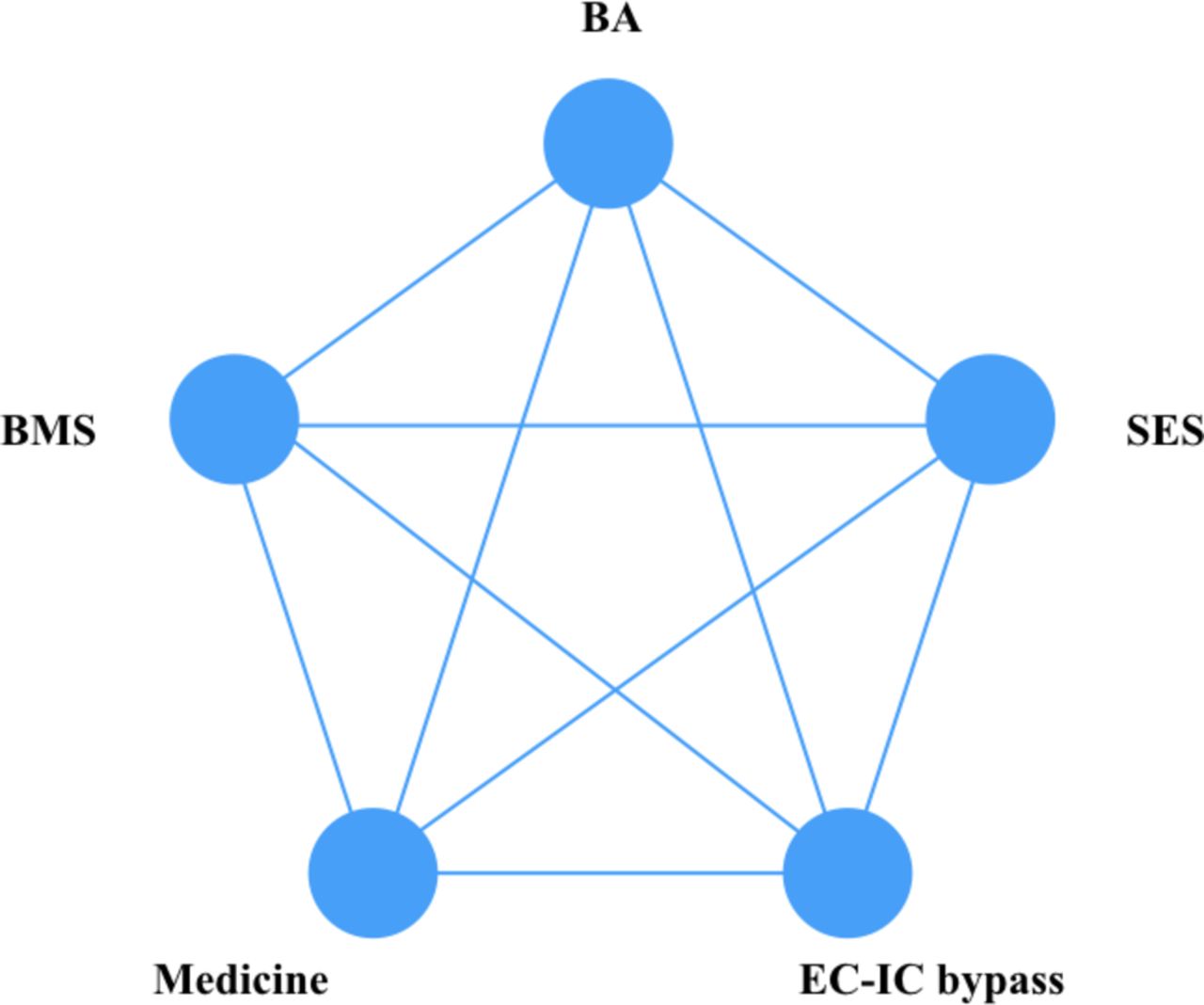
Initially, we will perform standard pairwise meta-analyses for every direct treatment comparison with at least two studies (see figure 1). We will use the Bayesian random-effects models to derive summary effect measures with associated 95% CIs.48 The normal distribution will be used in the vague priors for all trial baselines, treatment effects and between-study SD.

{kind=link}
Network of all possible pairwise comparisons between the eligible interventions. BA, balloon angioplasty; BMS, balloon mounted stent; EC–IC bypass, extracranial to intracranial bypass; SES, self-expanding stent.
Methods for indirect and mixed comparisons
We will perform network meta-analysis using the three-level hierarchical, random-effects model as described in Schmitz et al.49 The normal distribution will also be used as the vague priors. We will rank relative treatment effects using mean ranks and the SUCRA.39 Rank-heat plots will be used to display the treatment rankings across multiple outcomes.50
Assessment of statistical inconsistency
We will evaluate the inconsistency between direct and indirect data locally by using the loop-specific method51 52 and the node-splitting method,53 and globally by using the design-by-treatment interaction model.54
Investigation of heterogeneity and inconsistency and sensitivity analyses
Subgroup analyses will be conducted to explore if sufficient data are available. The following effect modifiers will be included in subgroup analyses: age, sex, degree of preprocedural stenosis, functional status at presentation and stenosis site of the intracranial artery. Network metaregression will be used to explore the effect of study year and study country if more than 10 studies are available. Sensitivity analyses will be conducted to test the robustness of our study findings by incorporating only data from the following studies when adequate studies are available: RCTs, quasi-RCTs and cohort studies reporting effect measures that are adjusted for important confounders.
Patient and public involvement
As the present study is a systematic review based on published data, patient and the public are not involved in the study design, conduct, data analysis and result dissemination.
Discussion
The main anticipated challenge for the present systematic review and network meta-analysis is incorporating both randomised and observational studies. The rationale for including non-randomised studies is to obtain adequate statistical power to evaluate the outcomes, especially for the rare complications, because only a small amount of randomised studies were identified through an experimental search for eligible studies. Given that observational studies have inherited methodological limitations compared with randomised studies, another challenge is ensuring the treatment comparisons in our study maintain transitivity in our network meta-analyses while also remaining clinically meaningful to knowledge users.
It is expected that the study findings will address important questions about the relative safety and efficacy of different endovascular treatments for patients with symptomatic ICAS, allow patients and care providers to make informed decisions and provide comprehensive information for future study designs.
Ethics and dissemination
Ethics approval is not needed as systematic review is based on published studies. Study findings will be presented at international conferences and published on a peer-reviewed journal.
References
Footnotes
TW and XW contributed equally.
Contributors LJ, FL and YM developed the initial idea for this study. XW, TW and KY developed and revised the search strategy. TW, JZ and PG finished the study design. LJ, FL and YM were consulted about clinical issues. TW, JL and KY contributed to the original draft. PG, JZ and XW were responsible for the revision of the draft. TW and XW contributed equally to this article. All of the authors approved the final work prior to submission.
Funding This work was supported by the Ministry of Science and Technology of the People’s Republic of China (2016YFC1301700).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data from the study are available upon request to corresponding authors via e-mails.