Article Text

Abstract
Objective To identify adequate criteria to determine the success or failure of mandibular advancement device (MAD) treatment for obstructive sleep apnoea (OSA) based on long-term symptoms and new-onset hypertension.
Design Observational cohort study.
Setting A tertiary care hospital setting in South Korea.
Participants Patients (age >18 years) who were diagnosed with OSA by a polysomnography (PSG) or Watch peripheral arterial tonometry (PAT), and who had been treated with MAD between January 2007 and December 2014 were enrolled.
Primary and secondary outcome measures Patients underwent PSG or Watch PAT twice; before and 3 months after the application of MAD. The patients were categorised into success and failure groups using seven different criteria. MAD compliance, witnessed apnoea and snoring, Epworth Sleepiness Scale score and occurrence of new-onset hypertension were surveyed via telephonic interview to determine the criteria that could identify success and failure of MAD.
Results A total of 97 patients were included. The mean follow-up duration was 60.5 months, and the mean apnoea–hypopnoea index (AHI) was 35.5/hour. Two of the seven criteria could significantly differentiate the success and failure groups based on long-term symptoms, including (1) AHI<10/hour with MAD and (2) AHI<10/hour and AHI reduction of >50% with MAD. Kaplan-Meier survival analysis showed that one criterion of AHI<15/hour with MAD could differentiate the success and failure groups based on new-onset hypertension (p=0.035). The receiver operating characteristic curve analysis indicated that the cut-off AHI for new-onset hypertension was 16.8/hour (71.4% sensitivity and 75.0% specificity).
Conclusion Our long-term follow-up survey for symptoms and new-onset hypertension suggested that some of the polysomnographic success criteria, that is, AHI<10/hour with MAD, AHI<10/hour and AHI reduction of >50% with MAD and AHI<15/hour with MAD may be useful in distinguishing the success group from failure one. Further prospective longitudinal studies are warranted to validate these criteria.
- Obstructive sleep apnea
- Mandibular advancement
- Hypertension
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Strength of this study is that this is an observational cohort study to identify the optimal polysomnographic success criteria for mandibular advancement device treatment based on long-term subjective symptom changes or occurrence of new-onset hypertension.
This study was limited in its telephonic interview-based study design.
Diagnosis of hypertension was estimated based on a physician-diagnosed disease.
Potential interviewer bias and respondent’s recall bias may exist.
Introduction
Obstructive sleep apnoea (OSA) is associated with many chronic diseases1 such as cardiovascular diseases,2 cerebrovascular diseases,3 metabolic syndrome4 and neurocognitive dysfunction.5 Furthermore, it may be a risk factor for the future development of hypertension.6 7 A short-term randomised controlled trial showed that continuous positive airway pressure (CPAP) treatment for OSA reduces cardiovascular morbidity.8 Therefore, it is important to focus on effective treatments for OSA to reduce its associated comorbidities.
The mandibular advancement device (MAD) is generally indicated for use in patients with mild-to-moderate OSA.9 However, MAD treatment is not always inferior to CPAP therapy and has been reported to show better compliance than CPAP.10 11 MAD treatment has shown beneficial effects on the number of obstructive breathing events, arterial oxygen saturation levels and arousal frequency.12 Furthermore, meta-analysis of several observational and randomised controlled trials showed that MAD reduces blood pressure in patients with OSA.13 14 Although MAD is frequently prescribed by sleep specialists due to its efficacy, there is no validated standard criterion for determining the success or failure of this treatment for OSA based on long-term subjective symptomatic improvement or occurrence of medical comorbidities. Theoretically, an apnoea–hypopnoea index (AHI)<15/hour or AHI<5/hour without symptoms such as witnessed snoring, apnoea, and daytime sleepiness are required for treatment success. However, these polysomnography (PSG)-based definitions of success do not always agree with subjective improvement experienced by patients. Furthermore, the literature provides various criteria for defining treatment success. One recent study reported that the success rate of OSA treatment with MAD can vary remarkably according to the success criteria.15 However, success or failure cannot be defined by PSG findings alone. A long-term observation of symptom improvement or occurrence of complications is necessary to identify the relationship between success/failure and PSG findings with MAD.
To the best of our knowledge, no long-term follow-up study based on subjective symptom changes or occurrence of new-onset hypertension has thus far identified the optimal PSG success criteria for MAD treatment. Therefore, in the present study, we aimed to determine adequate success criteria for MAD treatment of OSA on the basis of long-term symptoms and occurrence of new-onset hypertension.
Methods
Patients
This observational cohort study included consecutive patients (age >18 years) who were diagnosed with OSA (AHI ≥5/hour and symptoms of snoring, fragmented sleep, witnessed apnoea or daytime sleepiness) by an attended, full-night, in-laboratory PSG or Watch peripheral arterial tonometry (PAT), and who had been treated with MAD at our sleep clinic between January 2007 and December 2014. The MAD was designed to hold the mandible fixed at 60% of the maximum protrusion. All the patients were regularly followed up to evaluate any dental or temporomandibular joint problems and to adjust the advancement length. Data regarding demographic parameters, including body mass index (BMI), daytime sleepiness (by the Epworth Sleepiness Scale (ESS)), medical diseases and current medication use were collected. Blood pressure was measured at the start of MAD treatment. Patients underwent PSG or Watch PAT twice; before and 3 months after the application of MAD.
Patients with the following conditions were excluded for MAD treatment: central sleep apnoea; regular use of sedatives or narcotics; pre-existing pulmonary or psychiatric diseases; and any contraindication for MAD such as poor teeth, periodontitis and temporomandibular joint disorders. Patients who were not available for telephone interviews or have missing data for any of the variables were excluded from the study.
Criteria of treatment success
The following six criteria for OSA treatment success which have been used in the literature were analysed, as described in our previous study16: AHI<10/hour with MAD; AHI<20/hour with MAD; AHI<10/hour and AHI reduction of >50% with MAD; AHI<15/hour and AHI reduction of >50% with MAD; AHI<20/hour and AHI reduction of >50% with MAD; and AHI reduction of >50% with MAD. We added another criterion of AHI<15/hour with MAD, which is the cut-off AHI to differentiate mild from moderate OSA. Thereafter, patients were categorised into the success and failure groups based on each of the seven criteria (table 1).
The criteria for success of obstructive sleep apnoea (OSA) treatment
Collection of follow-up data
Follow-up data were obtained via telephonic interviews using a specially designed questionnaire. Telephonic interview was performed at least twice for each patient with the same questionnaires to confirm their answers. For data on MAD compliance, time of use per night and number of nights per week were assessed. Good compliance was defined as the use of MAD >4 hour/night for ≥5 days/week.17 Witnessed apnoea and snoring were asked to score on a scale from 0 (no symptom) to 10 (very bad), and the ESS score was used to assess the likelihood of falling asleep in eight different situations. In addition, occurrence of physician-diagnosed new-onset hypertension and antihypertensive medications since commencement of MAD treatment was assessed based on longitudinal review of our electronic medical system and telephonic interview.
Statistical analysis
All statistical analyses were performed using SPSS V.18. Continuous variables are expressed as the mean ±SD, and categorical variables are expressed as proportions. Paired t-tests were used to compare the sleep-related parameters before and after MAD application in all patients. Unpaired t-tests were used to examine the differences in witnessed apnoea, snoring and ESS score between the success and failure groups. A repeated-measure analysis of variance (ANOVA) was used to assess changes in variables from pretreatment to post-treatment between groups. Survival analysis was used to compare the time elapsed from MAD prescription to newly diagnosed hypertension between groups. Survival analysis was conducted using Kaplan-Meier survival curves. With regard to the post-treatment AHI value as a parameter for differentiating patients with new-onset hypertension from healthy subjects, sensitivity and specificity values for optimal cut-off were calculated using the receiver operating characteristic (ROC) curve. A p value <0.05 was considered statistically significant.
Patient and public involvement
Patients were not involved in setting the research question and in the design of the study. We introduced the purpose of this research to the patients. Informed consents were sought from all the participants. All the participants completed this survey on the voluntary basis. Small gifts were given to the participants who completed this telephonic interview. No patient was asked for advice on interpretation or writing up of results. The results of the research will not be disseminated to the patients.
Results
Out of 214 MAD-treated patients who underwent the follow-up sleep study, 107 were not available for telephone interviews because of phone number change or rejection or had missing data. Thus, a total of 97 patients (77 (79.4%) men and 20 (20.6%) women) were enrolled, and their characteristics are presented in table 2. The baseline age, BMI and AHI was 50.8±9.9 years (range, 19–68 years), 25.8±2.8 kg/m2 and 35.5±19.8/hour, respectively. According to Cartwright’s criteria,18 90 patients had position-dependent OSA and 7 patients had position-independent OSA.
Characteristics of 97 subjects treated with a mandibular advancement device
Short-term PSG follow-up with MAD
Table 3 summarises the sleep-related parameters before and 3 months after application of the MAD. After treatment, there was significant improvement in AHI (p<0.001), apnoea index (p<0.001), supine AHI (p<0.001), lateral AHI (p=0.004), lowest O2 saturation (p<0.001), oxygen desaturation index (p<0.001) and the percentage of sleep time with snoring (p<0.001).
Changes in the sleep-related parameters before and after treatment with a mandibular advancement device
Long-term symptomatic changes
The mean follow-up duration was 60.5±26.6 months (range, 8–107 months). Table 4 shows the changes in witnessed apnoea, snoring and ESS after MAD treatment in the success and failure groups according to the seven criteria. The highest rate of treatment success was 74.2% (72/97 patients) when using criterion 3 (AHI<20/hour with MAD) and lowest at 45.4% (45/97 patients) when using criterion 4 (AHI<10/hour and AHI reduction of >50% with MAD).
Change in the witnessed apnoea, snoring and Epworth Sleepiness Scale score after mandibular advancement device treatment in the success and failure groups according to the seven criteria
Repeated-measure ANOVA analyses adjusted for age, sex, BMI and compliance identified adequate criteria in determining the success or failure of MAD based on long-term symptom improvement. With criteria 2 (AHI<15/hour with MAD), 3 (AHI<20/hour with MAD) and 5 (AHI<15/hour and AHI reduction of >50% with MAD), there was no significant difference in the improvement of symptoms between the success and failure groups. With criteria 6 (AHI reduction of >50% with MAD) and 7 (AHI<20/hour and AHI reduction of >50% with MAD), only ESS improved to a larger extent than that in the success group. In contrast, there was a significantly larger improvement in the witnessed apnoea, snoring and ESS from pretreatment to post-treatment in the success group compared with the failure group when using criteria 1 (AHI<10/hour with MAD) and 4 (AHI<10/hour and AHI reduction of >50% with MAD).
Survival analysis for new-onset hypertension
Among the 97 patients, 34 (35.1%) had hypertension before treatment and 7 patients were newly diagnosed with hypertension during the follow-up and all of the 7 patients showed poor compliance. Kaplan-Meier survival analyses were performed for all the seven success criteria and the analysis showed that only criterion 2 (AHI <15/hour with MAD) could significantly differentiate between success and failure on the basis of new-onset hypertension (p=0.045) (figure 1).

Kaplan-Meier survival curves for new-onset of hypertension (HTN) in success and failure groups. AHI, apnoea–hypopnoea index.
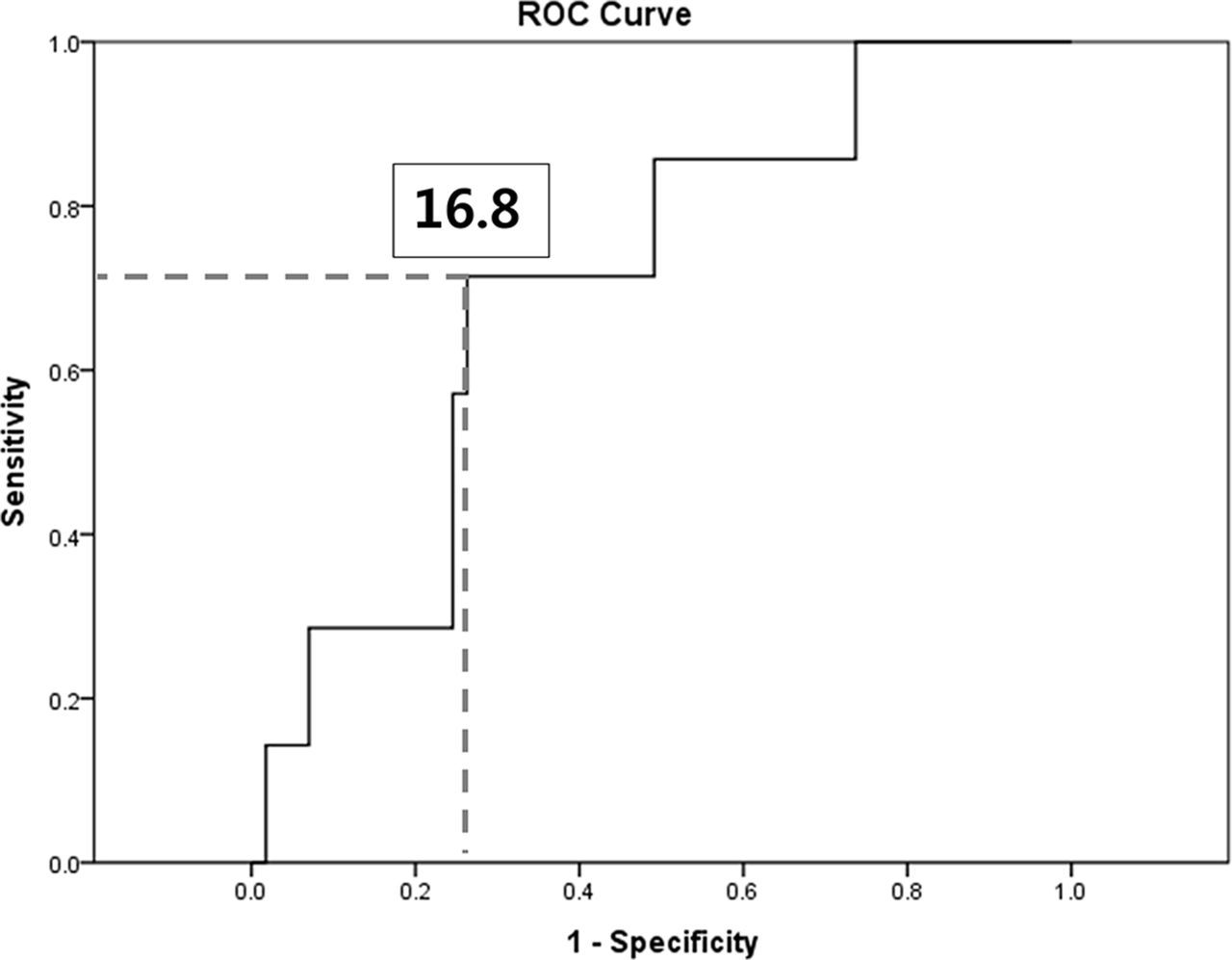
ROC curve analysis for new-onset hypertension
For assuming post-treatment AHI value as a parameter differentiating patient with new-onset hypertension from healthy ones, the ROC curve analysis indicated that the cut-off AHI was 16.8/hour, with an area under the curve of 0.704 (p=0.080), a sensitivity of 71.4% and a specificity of 75.0% (figure 2).

{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curve of apnoea–hypopnoea index with mandibular advancement device for new-onset hypertension.
Discussion
To our knowledge, this is the first study to identify adequate criteria to determine the success or failure of MAD as a treatment based on long-term symptom improvement and occurrence of new-onset hypertension in OSA. The most commonly used criterion for surgical success for OSA is postoperative AHI<20/hour and AHI reduction of >50%.19 CPAP therapy is a standard treatment of OSA and considered to be successful if the AHI reduces to <5/hour with CPAP.20 Although MAD is one of the treatment options of OSA, there is no standardised criterion to define successful outcome of MAD treatment. Although one study emphasised the need to establish a uniform definition of treatment success of OSA by using the MAD, they did not suggest an adequate criterion.15
Generally, the effectiveness of treatments for OSA is reported as change in AHI. However, it is unclear whether symptoms or comorbidities persist when AHI is improved by such treatment. Recent evidence indicates that there is no correlation between AHI and clinical outcomes21–23 and emphasises subjective sleepiness, snoring, quality of life and prevention of deleterious effects on comorbidities. Furthermore, several studies have demonstrated a discrepancy between statistically significant outcomes and clinically relevant outcomes. One review24 highlighted the importance of ‘highly effective treatment’ over ‘subtherapeutic treatment’ as a necessity for improved health outcomes in OSA. Thus, we focused on the long-term sleep-related symptomatic changes and occurrence of new-onset hypertension.
We found that two success criteria based on the AHI change with MAD—AHI<10/hour with MAD and AHI<10/hour and AHI reduction of >50% with MAD—could differentiate between success and failure on the basis of all three long-term OSA-related symptoms such as witnessed apnoea, snoring and daytime sleepiness. Given that PSG-based assessment of treatment response may not always agree with subjective improvement experienced by patients, these criteria may be helpful when sleep doctors interpret subjective symptomatic changes after application of MAD.
This study also showed that the criterion of AHI<15/hour with MAD differentiated success from failure on the basis of new-onset hypertension. OSA is known to be an independent risk factor for the development of hypertension.6 25 26 In contrast, in a sleep heart health cohort study, sleep-disordered breathing was a not a significant independent predictor of incident hypertension after adjusting for BMI. However, in a subgroup analysis, sleep-disordered breathing predicted future hypertension among women and less obese persons (BMI ≤27.3 kg/m2).27 In our study, all patients were Asians, who are generally less obese than the Western population. A meta-analysis showed that MAD treatment for OSA improves blood pressure control and suggested that blood pressure reduction may portend significant risk reduction for prevalent comorbidities such as hypertension.13 A recent study reported that the effects of an adjustable MAD were not significantly different to CPAP in terms of 24-hour mean ambulatory blood pressure, daytime sleepiness and disease-specific and general quality of life.11 Furthermore, the latest guideline for oral appliance use in OSA by the American Academy of Sleep Medicine (AASM) and American Academy of Dental Sleep Medicine (AADSM) shows a modest impact on reducing blood pressure.12
In the current study, nearly half of the patients had severe OSA. The guideline of the AASM on OSA treatment suggests that MAD should primarily be used in patients with mild-to-moderate OSA.10 However, in a previous study, patients with severe OSA had comparable successful outcomes to those with moderate OSA who received MAD treatment.28 In particular, in the group with moderate-to-severe OSA, patients with position-dependent OSA had better treatment outcomes with an MAD than patients with position-independent OSA.29 In the present study, most patients (92.8%) had position-dependent OSA. In addition, recent meta-analysis by AASM/AADSM showed significant efficacy across all level of OSA severity in adult patients using oral appliance.12
However, our study was limited in its telephonic interview-based study design. There was a period between the follow-up sleep apnoea/hypopnoea test and the telephonic interview. Potential interviewer bias and respondent’s recall bias may exist. The efficacy of the MAD may be changed or there may be some other changes in bodyweight or compliance that may influence the symptomatic benefit. Therefore, we adjusted the effects for the age, sex, BMI and compliance in the statistical analyses. In this study, diagnosis of hypertension was estimated based on a physician-diagnosed disease. However, even in sleep heart health study, they reported the association between sleep-disordered breathing and self-reported cardiovascular disease.7 In addition, subjective compliance was assessed using self-report. Objective compliance can be measured when using MAD that embedded temperature-sensitive microsensor. However, a previous study has reported a high agreement between self-reported and objectively measured compliance.30 Considering that most previous studies have focused on simple comparisons between AHI without or with MAD, this study may have another clinical implication as it highlights the relationships between the AHI changes with MAD and long-term symptom improvement or occurrence of one of medical comorbidities. Patients underwent PSG or Watch PAT. Although the same sleep studies were performed for pre treatment and post treatment in terms of each patient, there is still a limitation in the reliability of using Watch PAT. A previous study showed that Watch PAT has a limited value in detecting mild OSA while it is useful in detecting moderate to severe OSA.31
In conclusion, the present study demonstrated that AHI<10/hour with MAD or AHI<10/hour and AHI reduction of >50% with MAD may be useful as criteria to distinguish successful patients from unsuccessful ones on the basis of long-term symptom improvement. In addition, AHI<15/hour with MAD may be a criterion to differentiate between success and failure groups on the basis of new-onset hypertension. Future prospective studies are warranted to validate our proposed success criteria.
Acknowledgments
The authors thank all members of research team for the patient advisers and for the assistance in data collection.
References
Footnotes
Contributors JHW, C-SR and J-WK conceived the study design. JHL and JEG coordinated the study. JHW and JHL completed data collection and made the statistical analysis. JHW and J-WK conducted interpretation of results and drafted the manuscript. CSR and J-WK revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Funding This study was partly supported by the research Fund from the Seoul National University Bundang Hospital (Grant No. 02-2015-035) and the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science and ICT (NRF-2015M3A9D7066972).
Disclaimer The funding organisations had no role in the design and conduct of the study; in the collection, management, analysis and interpretation of the data; in the preparation, review or approval of the manuscript; and in the decision to submit the manuscript for publication.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the Seoul National University Bundang Hospital Institutional Review Board, and the study was conducted according to the principles expressed in the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.