Article Text

Abstract
Objective The current study aimed to investigate the relationships among the perceived quality of healthcare services, satisfaction and behavioural intentions among international students in Kuala Lumpur, Malaysia.
Setting A cross-sectional study on public universities in Kuala Lumpur, Malaysia.
Participants All participants in this study were international students joining public universities in Kuala Lumpur, Malaysia.
Primary independent variable Perceived quality of healthcare services measured on a SERVQUAL scale.
Primary dependent variable Participants’ satisfaction of healthcare services assessed using five items.
Secondary dependent variable Behavioural intentions measured on six items.
Results Of the 556 international students, 500 (90%) completed the survey. The study used structural equation modelling (SEM) through the AMOS (Analysis of Moment Structures) software to analyse the data. SEM analyses showed that the perceived quality of healthcare services significantly and directly affected satisfaction, with a value of 89% and an effect size of 0.78. It also had a significant indirect impact on the behavioural intentions (0.78) of international students. The results indicated that participants’ satisfaction had a statistically significant impact on their behavioural intentions (0.77).
Conclusion Perceived quality of care is an important driver of international students’ satisfaction and their behavioural intention with healthcare services. Such relations of effects among the three investigated factors were also positive and significant.
- servqual scale
- quality of health care services
- satisfaction
- behavioural intentions
- international students
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- servqual scale
- quality of health care services
- satisfaction
- behavioural intentions
- international students
Strengths and limitations of this study
To the best of our knowledge, this study is the first to examine the association between perceived quality of care, satisfaction and behavioural intentions from international students’ perception in Malaysia.
The study provides novel information on using SERVQUAL and the use of structural equation modelling on the relationships among perceived quality of healthcare services, satisfaction and behavioural intentions of international students in Malaysia.
A methodological concern is that there is no comparison group of patients to compare with the international student population.
Introduction
Recently, within the increasing force of globalisation, the role of higher education in supporting the national economy of any country has been highly recognised worldwide. Higher education has gone tremendous transformations and reforms as to enable universities to meet the increasingly growing demands for information and knowledge.1 In the Malaysian context, internationalisation of higher education has attracted a wide number of international students.2 Malaysia ranks 11th in the world in terms of intake of international students.3 Most of the international students come from various countries, including the Middle East countries.2 Moreover, the government aims to increase the number of international students from 108 000 today to 250 000 students by 2025 (Malaysia Education Blueprint 2015–2025, Higher Education). However, this raises the need to enhance the quality of services in meeting such international students’ requirements, including healthcare.
In this regard, the quality of healthcare has been approached by previous studies from different angles, including satisfaction.4–6 The findings of these studies indicate that satisfaction is a value added to other kinds of outcome measures since it plays a role in identifying the problems and imperfections in healthcare services. Other researchers7–9 that focused on the quality of healthcare services from patients’ behavioural intentions concluded that satisfaction serves as a mediator between the quality of healthcare and behavioural intentions. Furthermore, high perceived service quality, patient satisfaction and perceived value are conducive to positive behavioural intentions.9–11
Previous studies have investigated the relationship between patients’ perceived quality of healthcare and their satisfaction. The findings indicated that patients’ perceived healthcare quality positively affects their satisfaction of healthcare services.12 In the last few years, the relationship between these two constructs in healthcare has attracted the attention of many researchers.13–15 These studies, in addition to other recent studies16–20 that have examined the quality of healthcare service, used the service quality (SERVQUAL) model. They also reported that this model is the most reliable and valid model for investigating the quality of healthcare services. It is stated that SERVQUAL21 is a widely used scale to measure different quality dimensions.
Several researchers have examined the relationship between perceived healthcare quality and patients’ behavioural intentions in the healthcare context. They found that the perceived healthcare quality positively affects patients’ behavioural intentions.22 23 It is indicated that patients’ behavioural intentions can be determined by their perceived healthcare quality.24 Despite the importance of satisfaction and behavioural intentions in examining the quality of healthcare services, the majority of previous studies have focused on patients. In other words, many studies have focused on the quality of healthcare services from patients’ perspective, while only a very few studies have investigated this among international students worldwide.25 This could be due to the sufficient services offered by universities as a support to international students in better adjusting to the host country.26 However, the population of international students in different host countries still faces several challenging issues, including healthcare issues, which affect their adjustment and academic performance.27 28
However, studies among international students are very scant, and they are general in comparison with those studies carried out in other countries.29 For instance, while research on international students’ challenges and difficulties has reached its third phase of development in other host countries like Australia,30 in the Malaysian context such research is still in its early phase of development.29 In other words, no study has been conducted to investigate healthcare quality among international students, except for two studies26 31 which focused on their satisfaction. In the first study,31 the researchers reported that international students were unsatisfied with healthcare services, and more specifically most of them were unsatisfied with assurance as one of the healthcare quality dimensions. The second study26 reported that majority of international students agree that it is the care that is lacking. This means that they were dissatisfied with healthcare services. Therefore, these researchers emphasised the need for further investigating critical issues among international students, including their perception of medical and healthcare services in the Malaysian context. Moreover, there should be further empirical investigations into issues pertaining to international students’ needs and requirements in order to improve their achievement and performance.31 In relation to the health sector in the context of the current study, there is still a need for both public and private healthcare sectors to enhance the quality of healthcare services,32 especially because of the increasing number of international students joining Malaysian universities. Such investigation is expected to contribute to better understanding of the issues faced by international students in relation to healthcare. It will also enable policy makers, managers and providers of healthcare services to enhance the quality of healthcare services. Moreover, problems arising from students’ lack of satisfaction may result in students’ academic and social withdrawal, thus leading to non-completion of their degree programmes.33 Therefore, the current study aimed to investigate the relationships among perceived service quality, satisfaction and behavioural intention of healthcare services among international students in Kuala Lumpur, Malaysia. To achieve this aim, the following research hypotheses were tested:
Hypothesis 1: International students’ perceived healthcare quality has significant effect on their satisfaction.
Hypothesis 2: International students’ satisfaction significantly affects their behavioural intentions.
Hypothesis 3: There is an indirect significant correlation between international students’ perceived quality of healthcare services and their behavioural intentions via satisfaction.
Methodology
Study design
The current study used a cross-sectional design to collect the data at one point in time. Quantitative research is defined as a means for testing objective theories by examining the relationships among variables.34 Therefore, this design is appropriate for describing the status of phenomena or relationships among phenomena at a fixed point of time.35
Study setting
The context of the current study is Malaysia, which is a host country for many international students who come from different countries. Therefore, the population of this study comprises all international students joining Malaysian universities in Kuala Lumpur who had ever received a medical treatment service in Kuala Lumpur hospitals or clinics.
Sample size and sampling
The sample size needed for this study was calculated applying the formula for estimating a population proportion (prevalence of international student satisfaction) with a specified absolute precision.36 With desired confidence level (α) for α=0.05, Z2 1-α / 2=1.96 and precision or error that is allowable of 4.38%, the total sample size was 500. To factorise in 10% attrition, if (n) is the sample size required as per the formula and if (d) is the dropout rate, then the adjusted sample size N new is obtained as N1=n/(1−d). Therefore, the total sample size required after adjusting for dropout rate is 556. Hence, a total of 556 of international students from different countries joining two universities were selected through random sampling of Malaysian public universities in Kuala Lumpur.
A multistage sampling technique was used, and 556 students were selected randomly from the two universities. Moreover, the sampling frame included the lists of international students from the two universities. The participants were divided into homogeneous groups according to their positions before sampling, and then a random sample within each group was performed.
These groups are non-overlapping and together constitute the whole population of this study. These groups are categorised as postgraduate students and undergraduate students from both universities. A stratified sampling technique was used because it is appropriate when the population consists of different groups.34
The number of participants in the two groups was selected based on the overall number of the population in the two universities using a proportional to size method. The participants were contacted personally by the researcher. Each eligible respondent received a copy of the questionnaire manually. The contact number of the data collector and his email were provided to each respondent in case the respondents needed any clarification. All the international students who were joining the selected universities and who had ever taken medical treatment service in Kuala Lumpur hospitals or clinics and were willing to participate were eligible to be included in the sampling frame. However, those international students who had never received medical treatment services in Kuala Lumpur hospitals or clinics were excluded from this study.
Data collection
A self-administrated questionnaire consisting of four parts—demographic information, service quality, student satisfaction and behavioural intention—was distributed to the participating students. The second part of the questionnaire was for measuring the service quality. The current study used the SERVQUAL scale, which had been designed in a previous study,37 and later modified by many other recent studies.11 38–40 This scale contains 22 items that measure 5 exogenous constructs of service quality: tangibility, reliability, assurance, responsiveness and empathy. However, the application of SERVQUAL was contingent on five dimensions: tangible elements (physical facilities, equipment and appearance of personnel), reliability (ability to perform the promised service dependably and accurately), responsiveness (willingness to help customers and provide prompt service), empathy (caring and individualised attention that the firm provides to its customers) and assurance (including competence, courtesy, credibility and security).7 Based on these studies from which the SERVQUAL questionnaire was adopted, this questionnaire is a research instrument that has good reliability and validity, which have been tested and reported in several domains, including healthcare. It was also used in the current study because it was designed based on the SERVQUAL model.
In addition, the present study used a questionnaire to measure participants’ satisfaction and behavioural intentions as endogenous variables derived from an extensive literature review. Satisfaction was assessed using five items. These items were derived from three previous studies.11 41 42 On behavioural intentions, the instrument adopted from other studies9 43–46 encompasses six items. However, after testing this instrument for reliability and validity, three items were dropped. Each construct consists of items to which respondents would indicate on a 5-point scale the extent of their agreement or disagreement with each assertion, ranging from ‘Strongly disagree (score 1)’ to ‘Strongly agree (score 5)’. The internal consistency of this questionnaire as indicated by the Cronbach’s α value was 0.96. Moreover, the questionnaire includes sociodemographic information. Participation in the survey was voluntary.
The participants were contacted personally by the researcher. Each eligible respondent received a copy of the questionnaire manually. Thus, the total number of administered questionnaires was 556, while the returned questionnaires were only 518. Out of the 518 returned questionnaires, 18 were excluded because they were incomplete. So only 500 questionnaires were used for data analysis.
Patient and public involvement
In this study, no patient was involved in setting the research question or the outcome measures. The participants were also not involved in the design or conduct of the study. No patients were requested to provide advice on interpreting or reporting the results. The results of the study were not planned to be disseminated to the participants.
Data analysis
This study used SPSS (version 22) and AMOS (Analysis of Moment Structures) software as the two main statistical tools to analyse the data. To analyse the descriptive data of the respondents and the investigated variables, this research adopted a number of steps: descriptive analysis, assessment of reliability and validity, factor analysis, correlation analysis, and structural equation modelling (SEM) analysis.
Results
Descriptive results for respondents’ personal and professional characteristics
A total of 556 questionnaires were distributed and collected. After excluding the incomplete questionnaires, 500 questionnaires were included for the analysis. Therefore, the response rate was 90%. Regarding the descriptive results, 65% of the participants were joining the first public university, while 35% of them were joining another public university. The majority of the sample were from Asia (61.2%), followed by students coming from Africa (36.8%), Europe (1.6%) and North America (0.4%). Moreover, 76.6% of the participants were male, whereas 23.4% were female.
In terms of age, over two-thirds of the participants were younger than 40 years old. The results revealed that those who are between 19 and 29 years represented the highest percentage (65.8%) in the present study. However, the group of participants between 30 and 39 years represented 27.8% out of the overall number of participants. The percentage of the participating students in the age group of between 40 and 50 accounts for 6.4%, which is the lowest percentage in this study (table 1).
Descriptive results of respondents’ personal and professional characteristics
With regard to participants’ educational levels, students who were joining bachelor’s degree programmes accounted for 33.2% (166), while those joining postgraduate educational programmes represented almost 66.8%. Almost 38.2% of them are master’s degree students and 28.6% are PhD postgraduates. Approximately most of the participants (64.8%) were single, whereas married students represented 30.8%. Others were engaged (3%) and divorced (1.4%).
The results of the distribution of the respondents’ last time of visit to medical care indicated that 53.6% of the students had their last visit to a medical care sector more than 3 months ago before the data were collected. Moreover, 25.4% of the participants stated that their last visit to a medical care was between 1 and 2 months ago. Only 21.0% of the respondents stated that they had their last visit almost less than 1 month ago. In terms of the type of health sector that the respondents had their last visit for medical care, the majority of them (51.6%) stated that they had received health services from public hospitals. Other respondents (5.4%) stated that they were served by private hospitals, whereas 21.6% of the respondents tended to visit public clinics and 11.4% had been served by private clinics (table 1).
Results of reliability and validity analysis
The initial scale for service quality comprised the modified SERVQUAL items which were designed to capture the five dimensions: tangibility, reliability, responsiveness, assurance and empathy. Measurement analyses were intended to evaluate the properties of measurement (reliability and validity) for this scale proposed in the study. To achieve this, we performed exploratory factor analysis, correlation analyses and SEM as suggested in a previous study.47 48
In the present study, the three sections of the survey were tested in terms of its reliability using Cronbach’s α for each item and construct. Based on the results, as shown in table 2, some items of the responsiveness and assurance dimensions of the service quality were removed. First for the responsiveness dimension, which includes six items, the results of the factor analysis of the six items showed that the reliability is α=0.782. Yet, after removing items related to RES5 and RES6, the reliability improved to α=0.82. The remaining four items were used as a factor in the model analysis. Second, for the assurance dimension of the service quality which has five items, the result of the Cronbach’s α for all items was 0.67. Therefore, it was necessary to make an improvement on reliability by excluding ASS4 and ASS5 items. After removal of both items, the reliability became α=0.746, and the three remaining items of the assurance dimension were used in the model analysis.
Descriptive results of the reliability test
The satisfaction construct consists of five items. The reliability of the construct in its five items was α=0.73. However, after elimination of the item related to healthcare services (SAT3), it was enhanced to α=0.873. The latter version of the factor was used in the later model analysis. The final construct of behavioural intentions, which comprises six items, was also tested for reliability. The results indicate that the reliability of this construct was α=0.766 when involving all items in the factor analysis. However, after deleting three items—BI4, BI5 and BI6—from the construct, the reliability became α=0.889. Then, the three-item construct of behavioural intentions was used in the model analysis (table 2).
Finally, based on the result of the above steps, there were 22 reliable items conforming to their hypothesised dimensions for service quality, with a total Cronbach’s α of 0.94. The Cronbach’s α of the satisfaction and behavioural intention factors was 0.96 and 0.75, respectively. This is an indication of the high degree of reliability and consistency.49
Regarding the validity test, factors were tested for validity analysis by applying the Kaiser-Meyer-Olkin (KMO) and Bartlett’s test to the data.50 The results show that the KMO value was 0.884>0.60 for service quality constructs, 0.718>0.60 for satisfaction, 0.749>0.60 for behavioural intention and 0.905>0.60 for all constructs. Such results mean that the data are appropriate for more analyses.50–52 Previous studies proved that a value of validity test of 0.60 or higher was appropriate to continue with factor analysis. Finally, the results of reliability and validity show that the data were appropriate for further analyses.52
In estimating the hypothesised models, the covariance matrix derived from the data was used. Based on this estimation, the results satisfied the underlying theoretical framework, and it produced estimates of the desirable properties. In this study, the maximum likelihood estimation was adopted in order to generate estimates of the final research model. Once estimating the model, a set of conventionally accepted criteria was applied to assess the goodness of fit of the model.47 48 53
Descriptive results of the distribution of the items
With regard to the descriptive results of the distribution of participants’ responses to the items included, skewness and kurtosis tests were used to measure the distribution of the items in the survey. Skewness is a measure of the symmetry of the skewness value, which ranges from −3 to +3. A value of 0 indicates a perfect symmetry54 and the kurtosis value is less than 7.51 Table 3 presents the descriptive statistics obtained from the skewness and kurtosis tests for all items in the model of service quality, satisfaction and behavioural intentions in healthcare service. When the value of skewness ranges from −3 to +3 and the value of kurtosis is less than 7, a normal distribution of items is achieved.51 54 55 The results of the study indicate that all items of the model meet the criteria of normal distribution and are somehow approaching 0. This implies that the values of the skewness and kurtosis tests seem perfect. However, the negative values of the kurtosis test indicate a flatter distribution among these items. The negative values of the skewness test indicate a negative skew.
Descriptive statistics of individual items for each construct
The results of the descriptive analysis of the perceived quality of healthcare service are discussed in relation to the five dimensions: tangibility, reliability, responsiveness, assurance and empathy. Each dimension consists of a number of items in the survey. Therefore, after removal of the poorly relevant items mentioned above, the survey of the service quality consists of 22 items distributed as the following: five items for tangibility, five items for reliability, four items for responsiveness, three items for assurance and five items for empathy, which represent the SERVQUAL model to measure the perceived service quality factor.
When the respondents were asked to give their responses regarding the first five items of the tangibility construct, the results revealed that the highest M value (M=3.65) was scored by TAN3 on the staff’s neat appearance, followed by TAN1 (M=3.346) on the modernity of the equipment in the hospital. It was also found that TAN2 and TAN5 on the visually appealing physical facilities and the pleasant feature of the waiting area in the hospital scored the same mean value (M=3.324). However, when the respondents were asked about the visually appealing materials used for the healthcare service (TAN4), this item scored the lowest value among the five items of tangibility (M=3.27).
As far as the reliability dimension of the perceived quality of healthcare service, the respondents were asked to provide their responses to five items. The results show that the participating international students paid most attention to REL2 about providence of healthcare service as promised (M=3.258). This underlies international students’ assessment of the reliability of healthcare services in terms of whether they are provided as they are promised by such hospitals and clinics or not. This was followed by the right performance of the healthcare service for the first time (REL3) and the punctuality of providing healthcare services (REL5), with mean values of M=3.242 and M=3.232, respectively. However, REL1 and REL4 scored the lowest mean values (M=3.19 and M=3.10). This result indicates that such hospitals and clinics seem to pay the least attention to the sincere interest and maintenance of error-free records of the international students.
Regarding the responsiveness dimension of SERVQUAL, the international students were requested to rate their agreements and disagreements about four items of the responsiveness of staff in these Malaysian hospitals and clinics. The highest value (M=3.28) was scored by RES1 on the staff’s willingness to offer them help at hospitals and clinics. The mean values of RES2 and RES3, which stand for offering prompt healthcare services to the patients and being too busy to respond to patients’ requests for healthcare, were medium (M=3.16 and M=3.03). However, the lowest mean value was scored by RES4 (M=2.56) on the dependability of staff at hospitals and clinics (table 3).
In relation to the assurance dimension, the international students were asked about whether the staff in the hospitals and clinics make them confident, look consistently courteous with them and seem knowledgeable in answering their questions about their health. The descriptive results show that the mean values of these three items were medium (M=3.25, M=3.26 and M=3.23 for ASS1, ASS2 and ASS3, respectively).
The participants also responded to five items of the final dimension of the SERVQUAL empathy. They perceived the operating hours of the hospitals and clinics as convenient to them (M=3.136). It was followed by EMP1 related to the personal attention paid by the staff to the participants as patients (M=3.078). For other items—EMP2 and EMP3 about getting their requests responded and their needs understood by the staff of such hospitals and clinics—they scored medium mean values (M=3.064 and M=3.028). However, participants’ responses to EMP4 on whether such hospitals and clinics have their best interests at heart scored the lowest mean value (M=2.978).
The descriptive statistics of the overall dimensions of the SERVQUAL indicate that tangibility scored the highest mean value (M=3.38), followed by assurance (M=3.24), reliability (M=3.20), responsiveness (M=3.011) and empathy (M=3.035) (table 3).
With regard to the satisfaction construct, the mean value of SAT3 ‘I did the right thing when I decided to avail these hospitals/clinics’ was the highest mean value (M=3.206). The students also seemed to be satisfied about their decisions of visiting these hospitals and clinics to receive healthcare, as evident by the mean value of SAT2 (M=3.176). Following this was the mean value (M=3.11) of SAT1 on participants’ satisfaction of the healthcare service they received in the hospitals/clinics. However, SAT4, which concerns participants’ overall feelings about the service of care in this hospital according to their prior expectation, scored the lowest mean value (M=3.022) (table 3).
For the behavioural intentions of the healthcare services, the international students exhibited a good level of behavioural intentions to inform other people of the good healthcare services at the hospitals/clinics, as illustrated by BI3 with the highest value (M=3.154). BI1, which refers to students’ intention to recommend other people to receive healthcare services at such hospitals/clinics, scored the second highest mean value (M=3.104). Finally, when the participants were asked about their intention to consider such hospitals/clinics as their first choice in the future (BI2), their responses reflect the lowest mean value (M=2.996) (table 3).
In addition, the first-order factors were measured by items ranging from three to five items through SEM. Each item was assumed to load only on its respective dimension. The factor loading values for all items for the three factors—service quality, satisfaction and behavioural intentions—were statistically significant since the critical ratio (CR) is more than 1.946 and p=0.000. The values of the factor loadings were equal to 0.70 and above. Moreover, the values of factor loading for the five dimensions—tangibility, reliability, responsiveness, assurance and empathy—of second order (perceived service quality) were statistically significant in that the CR is more than 1.946 and p=0.000. The values of the factor loadings were also equal to 0. 70 and above (table 4).
Structure equation modelling results
Results of testing the measurement model of service quality
To determine the acceptability of the model fit, we used confirmatory factor analysis (CFA), specifically a number of fit indices, including the χ2, df, the χ2/df ratio, comparative fit index (CFI) and the root mean square error of approximation (RMSEA).56 57 The CFA generated significant results and are illustrated by the exogenous model in figure 1, including the χ2 statistic (χ2=483.68, df=199, p<0.00). This result indicates that the model fit was satisfactory. Given the χ2 test’s sensitivity to the relatively large sample size (n=500), we focused on increasing the fit measures: RMSEA, χ2/df and CFI. The values of these three fit measures were 0.054 (less than 0.08), 2.43 (less than 3) and 0.095, respectively. Such common measures usually provide sufficient information to evaluate a developed model since all measures are within the ranges of the recommended values.53 58 This implies that the model was suitable for structural modelling in order to test the research hypotheses.
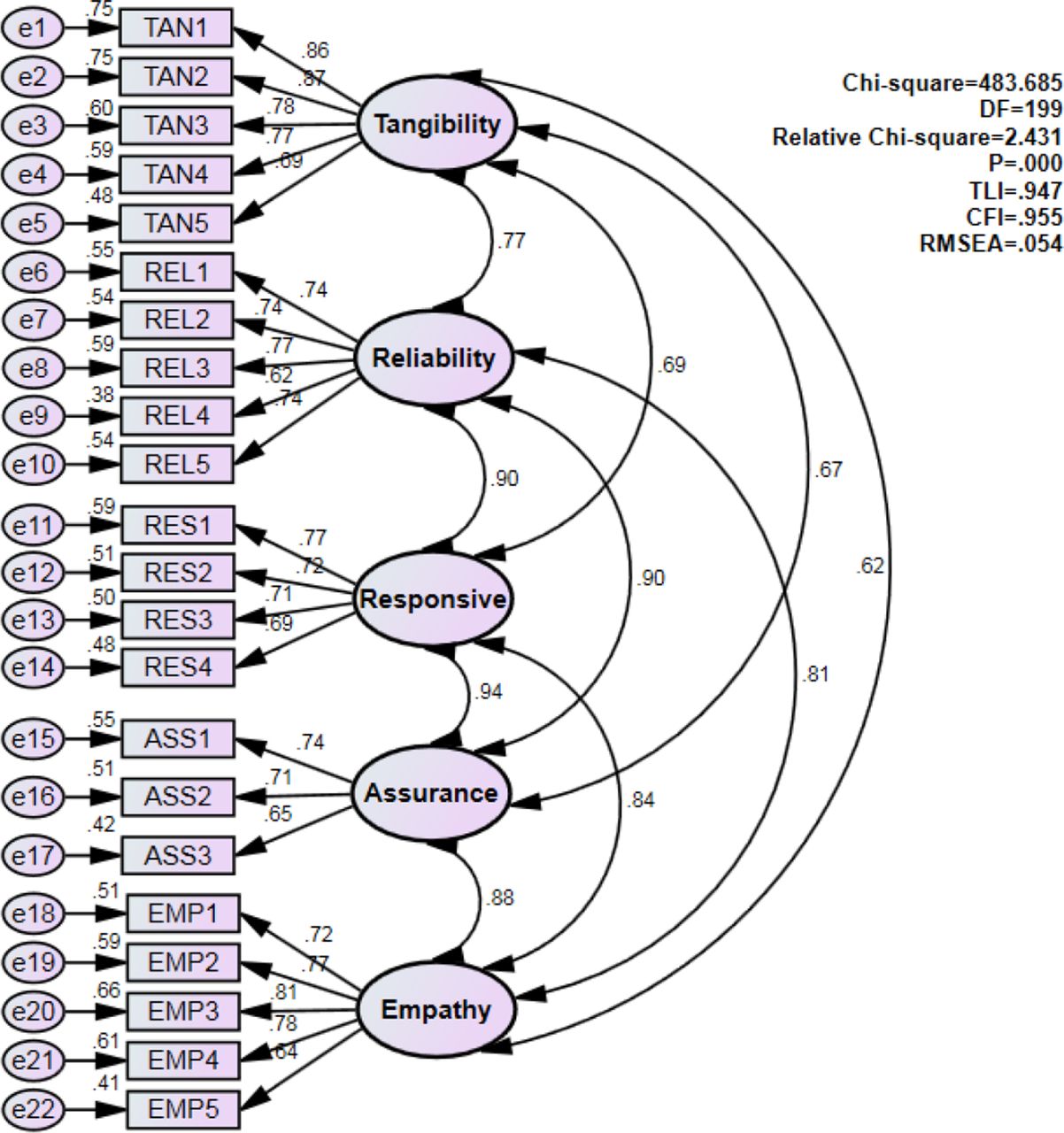
The CFA measurement model (exogenous correlation) summarised the incremental fit indices of the exogenous correlation. The model was tested through CFA. The first CFA indicated significant results, as shown in the figure. The CFA enables us to test how well the measured variables represent the constructs. However, each construct or factor contains at least three items. CFA, confirmatory factor analysis; CFI, comparative fit index; RMSEA, root mean square error of approximation.
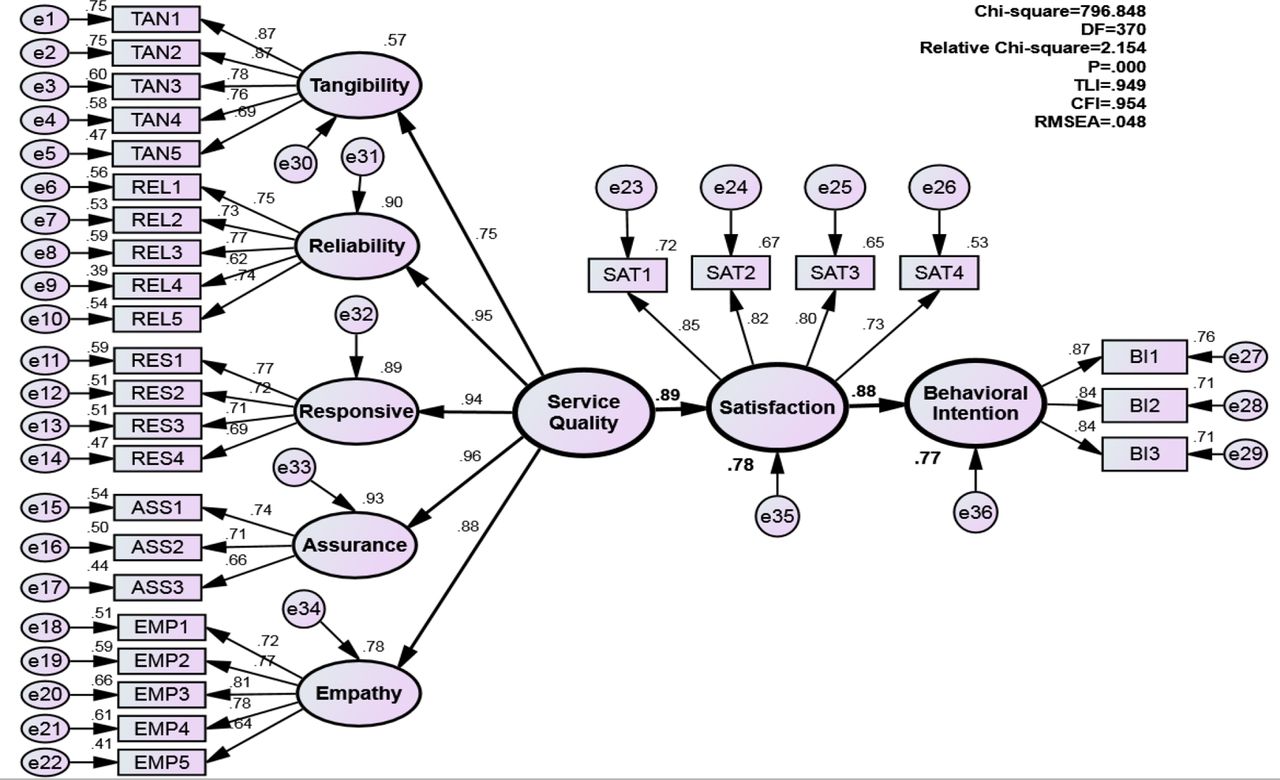
Moreover, the results of the second-order factors of the measurement model indicated that the hypothesised 29 items for the full measurement model were consistent with the data (an excellent fit of the model: χ2=2.154; CFI=0.954; Tucker–Lewis index (TLI)=0.950). The RMSEA was 0.048, which is below the recommended value of 0.080.59–61 The measurement of services quality, satisfaction and behavioural intentions generated the observed covariance matrix, and there was no evidence that the measurement model is incorrect. The factor loading values for all items of the three factors mentioned above were statistically significant and the CR/t-statistics is higher than 1.946 and p=0.000. The values of the factor loadings were also equal to 0.70 and above (figure 2 and table 4). For the five dimensions—tangibility, reliability, responsiveness, assurance and empathy of the first order (perceived service quality)—the loadings were statistically significant (CR/t-statistics is higher than 1.946 and p=0.000). The values of the factor loadings were also equal to 0.70 and above, as shown in table 4. The data supported the measurement adequacy in terms of their convergent and divergent validity, which is evident of the construct validity of the model.

{kind=link}
{kind=link}
The final full structure model which presents the model developed in this study. However, the developed structural model determines the overall goodness of fit for the causal model and estimates the magnitude and statistical significance for each path coefficient and the variance explained for each endogenous latent construct. Thus, regarding the developed model in the present study, as shown in the figure, it satisfies the criteria of goodness-of-fitness indices, as suggested by earlier researchers. Therefore, the model fits the empirical data well. Moreover, in the same figure, the path coefficient values between the factors are given. The item loadings that explain the relations between the survey item and factor are also identified in figure. The same figure also presents the results onthe goodness-of fit and estimated relationships . In this structural model, all the indices were revealed to satisfy the recommended values, which pointed out that the model fitness was excellent. CFI, comparative fit index; RMSEA, root mean square error of approximation.
Results of testing the research hypotheses
Following the confirmation of the measurement model as shown above, the structural model was used to test the proposed research hypotheses. In testing hypothesis 1 on the effect of students’ perceived quality of healthcare services on their satisfaction, the results show that this research hypothesis was statistically significant (CR/t-statistics is 15.5319>1.946 and p=0.000). The value of the relationship was 0.89. The effect size was 0.78, which implies that 78% from the students’ satisfaction is attributed to the perceived quality of healthcare services. This amount of the effect size was large as it is more than 0.60, as shown by the final full structure model in figure 2. Such result supports the effect of perceived quality on satisfaction as in hypothesis 1.
In testing hypothesis 2 on the effect of international students’ satisfaction on their behavioural intentions, the results also showed this research hypothesis was statistically significant (CR/t-statistics is 20.5701>1.946 and p=0.000). The value of the relationship was 0.88. Moreover, the effect size was 0.77, which means that 77% from the behavioural intention construct was attributed to students’ satisfaction. It was also found that the amount of the effect size was large as it is more than 0.60, shown in figure 2. These results confirm the hypothesised relationship in hypothesis 2.
Testing hypothesis 3 on the indirect effect of international students’ perceived quality of healthcare services on their behavioural intentions obtained interesting results. It was found that students’ perceived quality of healthcare services has an indirect and positive influence on their behavioural intentions via satisfaction. The value of the indirect relationship was the result of multiplying the above values of hypotheses 1 and 2 (0.89×0.88). The value was 0.78, which suggests that this indirect hypothesised relationship was statistically significant as it was tested using the Sobel test, 10.436>1.946 and p=0.0. The results of the present study confirm acceptance of the three tested research hypotheses.
Discussion
The present study aimed to examine and determine the relationships among the three investigated factors among international students in Malaysia: service quality (tangibility, reliability, responsiveness, assurance and empathy), satisfaction and behavioural intentions. The results indicated that there is a significant effect of students’ perceived quality of healthcare services on their satisfaction. This is comparable with previous research supporting the positive impact of healthcare services on their satisfaction. For instance, an earlier study reported that this factor had a significant positive influence on patient satisfaction (g21=0.82, p<0.01), and the total impact of service quality on patient satisfaction was 0.96.9 Therefore, it was concluded that service quality is an important antecedent to patient satisfaction. Another recent study has confirmed the significant impact of patients’ perceived quality of healthcare services on their satisfaction: β=0.27, p<0.01; β=0.13, p<0.01; and β=0.27, p<0.01, respectively.62 This factor was also found to have a significant direct effect on satisfaction (0.63, t=11.48, p<0.01).63
The current study revealed that the international students’ perceived quality of healthcare services explained almost 78% of their satisfaction. Such proportion of satisfaction is higher than that found in earlier studies. For instance, in some previous studies, service quality dimensions explained 54% of the total variation of outpatients’ satisfaction,64 while 42% of patient satisfaction was explained by the perceived healthcare quality.65 Therefore, the same hypothesised relation of effect between the two factors was supported by the results.
In this study, the relationship of effect between the international students’ satisfaction and their behavioural intentions was significant (0.660>0.05). This particular result was consistent with the results of previous studies in other disciplines42 66 67 which showed that the higher their satisfaction, the more intended customers will be to purchase and recommend such goods for others in the future. More specifically, in the domain of healthcare, the result of our study agrees with those reported by earlier researchers. For example, the overall customer satisfaction was strongly and positively associated with their behavioural intentions.68 The results of previous research also indicate that patients who were satisfied with the quality of healthcare services expressed their intention and willingness to pursue receiving their medical care from the same provider and also recommend them to others.69 Other researchers supported such result obtained in the present study regarding the positive effect of satisfaction on behavioural intentions.9 63 64 70 In the present study, 77% of the international students’ behavioural intentions could be explained by their satisfaction. This is higher than 72% than what was reported by a previous study64 and higher than 31% which was found in another previous study.68
The current study, in examining the relationship between the international students’ perceived quality of healthcare and behavioural intentions, provided evidence of the significant indirect effect of this factor on their behavioural intentions. The value was 0.78, which suggests that this indirect hypothesised relationship was statistically significant as it was tested using the Sobel test (10.436>1.946 and p=0.0). In contrast, in a previous study, it was found that behavioural intention was directly influenced by the perceived service quality (x31=0.18, p<0.01) and indirectly through satisfaction (b32=0.56, p<0.01).9 Moreover, in another study, the perceived quality had a total effect on behavioural intentions with a value of 0.79.63 Yet their results showed that behavioural intention was not fully mediated by satisfaction. The independent indirect relationship between the two variables via satisfaction proved to be significant in an earlier study.70
Implications and recommendations
The results of the present study underlie several important implications for managers of hospitals and clinics in the Malaysian context. Patients’ satisfaction and behavioural intentions towards healthcare services are important forms of outcomes of hospitals and clinics. This is because by being satisfied with the healthcare services offered to them, patients tend to develop positive behavioural intentions towards hospitals, which comprise a positive word of mouth, and customers’ willingness to reuse and recommend it to others. Another implication of the results is that understanding patients’ perceived quality of healthcare services cannot be well captured in isolation or independently from patients’ satisfaction and behavioural intentions and vice versa. It is necessary for policy makers in healthcare to renew policies that emphasise the importance of upgrading facilities, medical equipment and promote better medical environment that attracts more patients. This is because the international students in our study did not show high agreements with items related to equipment, facilities and environment in healthcare sectors.
However, it should also be noted that this study has some limitations. The investigation in this study was exclusive to the perceived quality of healthcare service, satisfaction and behavioural intentions. Therefore, future research could include additional relevant factors such as costs of medical care and trust that may affect patients’ perceived quality of healthcare services. Another limitation is that the study was conducted among 500 international students joining two public universities in Malaysia, and therefore, for future studies, a larger number of international students should be studied including those joining private universities to obtain results that could be more generalised and replicated. Future research should also use a mixed method combining both quantitative and qualitative data to provide deeper insights into the perceived quality of healthcare services. Finally, although the service quality scale was developed from previous research and a proposed model of healthcare service quality was validated, a caution should be taken when testing this model and making conclusions by future studies. This is because there are other factors such as the cost of healthcare services that should be added to our model.
Conclusion
The results showed that among the five investigated constructs for service quality, tangibility emerged as the most important determinant of patient satisfaction, followed by assurance. The results point out at a relative closeness between responsiveness and empathy in terms of their importance. It was also found that perceived service quality has a positive significant direct impact on student satisfaction, which has a significant direct effect on their behavioural intention, while their behavioural intention was influenced by perceived service quality positively and indirectly. The CFA indicated that 78% from satisfaction is attributed to the perceived quality of healthcare services, while 77% from the behavioural intention construct was presented by students’ satisfaction. The results of the current study have important implications for both patients and policy makers in healthcare.
References
Footnotes
Contributors MAAA and RAAA-M have been involved in the original study concept including formulating the study design and have been responsible for overseeing the work undertaken including data analysis. MHJ, MAS and LMS contributed to drafting of the paper and revising the paper in a critical way as to improve its important intellectual content. HKS and SARA-D participated in the analysis of the results and statistical analysis. All authors read and approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This research got an approval from the ethical committee on 23 July 2014 (Ref LUC/CPGS /2014/ 07/ 23/ 0006, Lincoln University College Research Ethics Committee). The data were collected through a survey after getting participants' consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data used in the current study are confidential and cannot be publicly shared. This was also stated in the participants' consent. However, it is available from the corresponding author on reasonable request.