Article Text

Abstract
Introduction Racial/ethnic minority school-age children are at risk for unhealthy weight gain during the summer, and there is a dearth of information regarding the underlying behavioural and environmental factors. The study objective is to provide an in-depth examination of dietary and physical activity behaviours and food, physical activity, and social environments of African American and Hispanic school-age children during the summer.
Methods and analysis An observational study will be conducted using a multistate (Ohio and Indiana, USA) prospective design examining the weight gain trajectory among a racially/ethnically diverse convenience sample of economically disadvantaged school-age children. In addition, a subset of these children will be evaluated to learn their daily health behaviours and food, physical activity, and social environments during the summer. Comparisons will be made between children who routinely attend programming and those who do not, both in the larger sample and subset. Determinants of programme participation and factors that may enhance the beneficial effects of programme participation will also be identified. Data collection at the Indiana site is planned for summer 2018.
Ethics and dissemination This study is approved by The Ohio State University Behavioral and Social Sciences Institutional Review Board. Results from this study will be disseminated in publications for practitioners, scientists and stakeholders.
Trial registration number NCT03010644; Pre-results.
- childhood obesity
- summer
- structured programming
- diet and physical activity behaviors
- food, physical activity, and social environments
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- childhood obesity
- summer
- structured programming
- diet and physical activity behaviors
- food, physical activity, and social environments
Strengths and limitations of this study
The primary strength of the current study is the prospective cohort design.
The multistate nature of the trial is another main strength as it allows the opportunity to examine the two racial and ethnic minority groups identified as being at highest risk for unhealthy summer weight gain.
An additional study strength includes reliance on multiple objective measures of weight status and obesogenic behaviours.
The primary limitation is reliance on a convenience sample.
Another study drawback relates to the limitation in the generalisability of findings, that is, children living in other regions of the country may experience differences in the behavioural and environmental exposure factors that contribute to unhealthy summer weight gain.
Background
Troubling data indicate that school-age children, particularly those from economically disadvantaged households and racial and ethnic minority backgrounds including African American and Hispanic children, are at risk for experiencing unhealthy gains in weight during the summer when school is out of session.1 2 There is limited knowledge of the external factors that may negatively impact health behaviours (eg, diet, physical activity) and weight during the summer; however, loss of the potential protective effect of schools (ie, provision of health snacks and meals, opportunity for structured and unstructured physical activity, positive role modelling by peers and teachers, structure from daily routines, health-promotion policies and programmes) have been suggested.3 Unfortunately, despite recommendations to identify solutions to address the problem (based in or out of the school setting),4 few efforts have been directed at designing evidence-based nutrition and physical activity programmes to prevent excess weight gain during the summer among economically disadvantaged children. In the absence of such interventions, the childhood overweight and obesity epidemic that currently affects more than one in three US children is expected to worsen, and the racial and ethnic minority health disparities will widen.5
To address the problem, the current research team has led the development and piloting of an evidence-based Nutrition Education, Recreation and Fitness summer intervention Camp, which via a group randomised control trial study design, tested the effect of three types of structured programming during the summer.6 Sites were randomised to one of three treatment or programming groups: (1) Enhanced Care (nutrition, physical activity and mental health programming); (2) Standard Care (nutrition and physical activity programming) and (3) Active Control (non-nutrition, non-physical activity and non-mental 4 hours (Head, Heart, Hands and Health) programming).7 The hypothesis was that Enhanced Care site participants would demonstrate greater improvements in weight status, as well as diet and physical activity behaviours compared with the Active Control and Standard Care site participants. Results showed that all three groups were equally protected from weight gain.8 Based on these findings, it was concluded that it is not the type of programming, but rather mere engagement in structured programming that may lead to protection of weight gain.8 Importantly, these results align with the Structured Days Hypothesis9 which posits that exposure to a non-independent or structured environment (eg, week days during the school year) is beneficial to a child’s obesogenic behaviours and weight status. Also, results from this previous study8 corroborate with other similar studies demonstrating that routine participation in structured programming during the summer—summer school10 or summer programming11–15—may be beneficial to child weight status.
To conclusively determine the potential protective effect of structured summer programming on child weight status, it will be critical for future research to include a negative control (ie, children who do not engage in any type of summer programming) in the study design. In addition, there is a near complete dearth of information regarding the health behaviours and environmental settings of economically disadvantaged school-age children during the summer months; as such, future studies should include an in-depth examination of key dietary and physical activity behaviours as well as the food, physical activity and social environments of children.
Project Summer Weight and Environmental Assessment Trial (SWEAT) proposes to fill this gap in knowledge by conducting an observational study using a multistate, prospective design that examines the weight gain trajectory among a racially and ethnically diverse convenience sample of economically disadvantaged school-age children who attend structured programming on a routine basis during the summer months and those who do not participate in structured programming. In addition, a subset of these children will be evaluated to learn their daily health behaviours, as well as their food, physical activity and social environments during the summer months.
Methods
Objectives and hypotheses
The specific aims of Project SWEAT are to:
Assess child weight gain trajectory during the summer months among a racially and ethnically diverse convenience sample of economically disadvantaged school-age children who are and are not engaged in daily structured programming.
Hypothesis: Children who are involved routinely in daily structured programming will be protected from unhealthy weight gain during the summer compared with their counterparts who are not involved in structured programming.
Examine the health behaviours (diet, physical activity, screen time, sleep) of racially/ethnically diverse economically disadvantaged school-age children who are and are not engaged in daily structured programming during the summer time.
Hypothesis: Children who routinely engage in daily structured summer programming will demonstrate more positive health behaviours, leading to decreased risk of inappropriate weight gain during the summer.
Examine the food, physical activity and social environmental settings of economically disadvantaged school-age children who are and are not engaged in daily structured programming during the summer time.
Hypothesis: Children who routinely engage in daily structured summer programming will demonstrate more positive food, physical activity and social environments, which will relate to a decreased risk of inappropriate weight gain during the summer.
Determine the child, caregiver, household and neighbourhood factors that prevent or promote participation in structured summer programming, as well as potential factors that enhance beneficial effects that result from involvement in programming.
For this exploratory aim, it is anticipated that determinants of participation in summer programming and factors that enhance programmatic effects exist that may ultimately inform policy reform will be determined.
Study design
Project SWEAT will be a multistate, prospective, observational study. It will be a collaboration between two Midwestern state universities to broaden the diversity of the sample by capturing the populations most at risk for unhealthy weight gain during the summer months—African American and Hispanic populations. Project SWEAT will be implemented at two elementary schools in severe low-income neighbourhoods in each participating state. To capture the most robust data on the health, social and physical environments as well as health behaviours of children during the summer months, a mixed-methods—quantitative and qualitative—approach will be employed guided by the social ecological framework (table 1).
Project SWEAT socioecological framework approach
Participants and recruitment
The research team at each university will work in collaboration with each respective school district for approval of and assistance with all research-related activities. The project will take place over the course of two School Years—School Year 1 and School Year 2. All children, through permission of their caregivers, in prekindergarten (pre-K) through fifth grades will be invited to participate in the main study during School year 1. An informational sheet describing the study and a demographic survey will be sent home with each child in pre-K through fifth grades at the selected schools. Data will be collected from all children from whom the Project SWEAT research team receives a completed demographic survey. Child assent will be obtained at time of data collection. Participating caregivers will be given a US$5 gift card per child and children will receive a Project SWEAT bracelet.
A subset of SWEAT participants will be recruited from the larger sample for the Project SWEAT substudy. Based on caregiver responses to questions on the demographic survey regarding expected child participation in summer programming, caregivers will be contacted and asked to participate. At least four children and their caregivers will be recruited from each grade (pre-K–fifth) at each respective school—two children who intend to attend some sort of structured programming during the summer and two children who do not intend to attend any structured programming during the summer. Only one child per family will be selected for the Project SWEAT substudy. Children and caregivers will complete additional caregiver permission forms, caregiver consent forms and child assent forms. Participating caregivers/families will be given a US$25 gift card at baseline (B0), a US$50 gift card at time point 1 (T1) and a US$50 gift card and a family pass to a local learning science centre at time point 2 (T2).
Data collection
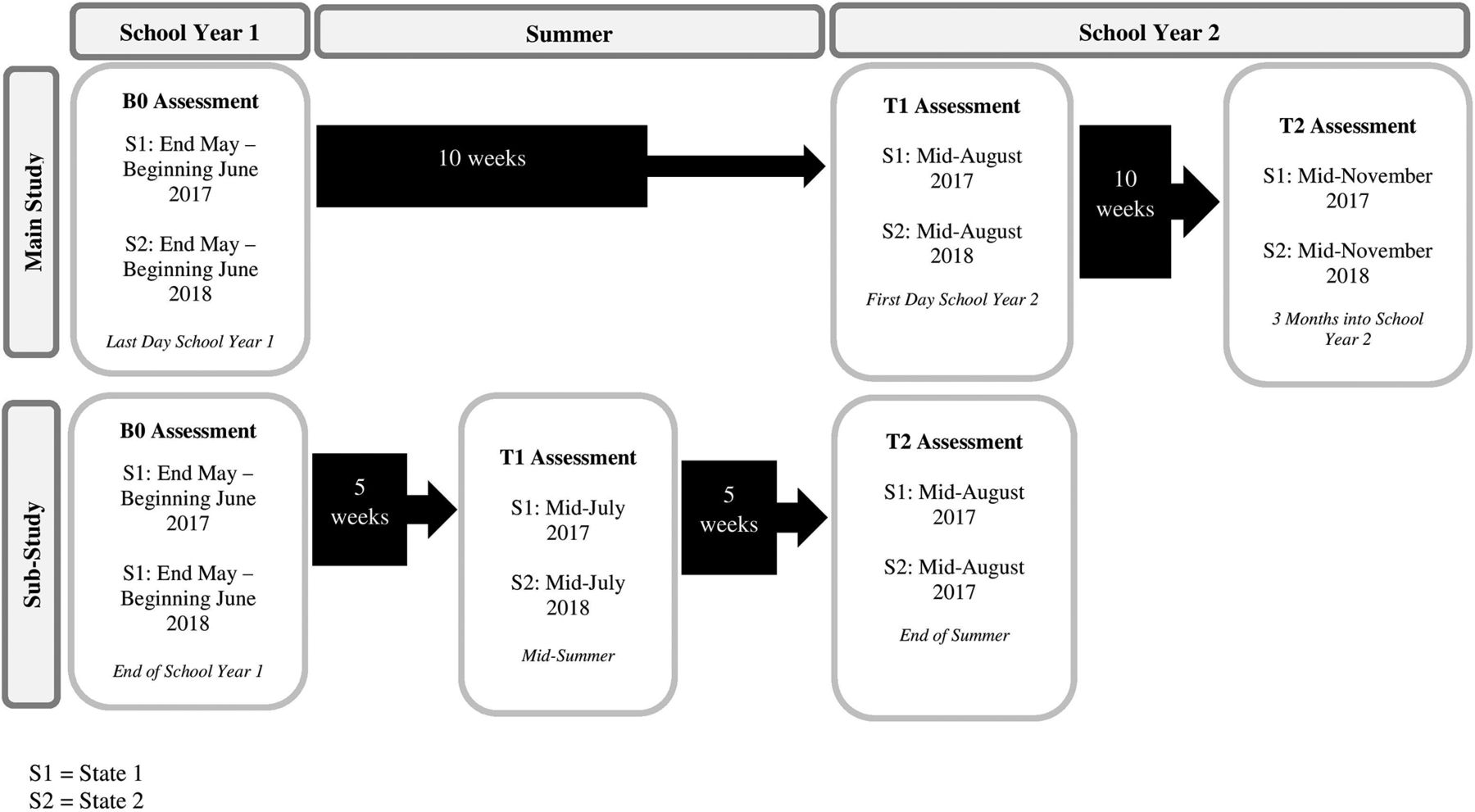
All data will be collected by trained data collectors, which will consist of graduate and undergraduate students studying nutrition, child development or other related fields. Described below are all Project SWEAT outcomes to be assessed, organised by main study and substudy Assessment and the socioecological framework. Table 2 and figure 1 provide an overview of the Project SWEAT evaluation plan. Note: data collection occurred at the Ohio site in summer 2017 and is planned for summer 2018 at the Indiana site.
Project SWEAT Study evaluation chart
{kind=link}
Project SWEAT evaluation plan. The study timeline for Project SWEAT, main study and substudy, will span two academic years and one summer. SWEAT, Summer Weight and Environmental Assessment Trial.
Main study
Individual level
Main study children will be assessed at baseline (B0; end of the School Year 1), time point 1 (T1; end of the summer/beginning of School Year 2) and time point 2 (T2; 3 months into School Year 2).
Child z-score body mass index (height and weight)
Child height and weight will be measured by a trained data collector using a Hopkins Road Rod Portable Stadiometer and BalanceFrom High Accuracy Digital Scale. Body mass index (BMI) z-scores and percentiles will be calculated using the statistical software Stata zanthro package, which transforms child height and weight data to z-scores using the Least Mean Square (LMS) method and reference datasets including the 2000 Centers for Disease Control and Prevention (CDC) Growth Reference, the British 1990 Growth Reference, World Health Organization (WHO) Child Growth Standards, WHO Reference 2007, the UK-WHO Preterm Growth Reference and the UK-WHO Term Growth Reference.16 17
Child waist circumference
Child waist circumference will be assessed using the The National Health and Nutrition Examimnation Survey (NHANES) waist circumference assessment protocol.18 Waist circumference z-scores and percentiles will be calculated.
Child blood pressure
Child blood pressure will be assessed using the National Heart Blood and Lung Institute (NHBLI) blood pressure protocol.19 Child blood pressure will be assessed by a trained data collector using an automated, calibrated CONTEC08A blood pressure monitor. Blood pressure systolic and diastolic z-scores and percentiles will be calculated.
Child attendance at structured summer programming
On the SWEAT informational sheet, caregivers will be asked the following questions regarding summer programming: (1) Do you plan to send your child to camp? (2) If yes, what is the name of the camp and where is it located? (3) How often do you think your child will attend? (4) Can we send you a weekly text this summer to ask how many days your child attended or did not attend a programme/camp? During the summer, at the end of each week using the TextIt20 text messaging platform, consenting caregivers will receive a text message that states: ‘Hello from Project SWEAT! How many days this week did (Child Name) attend a summer programme? Please respond with a number from 0 to 5, where 0—no days, 2–2 days.’ Non-responders will receive a follow-up text message and phone call.
Interpersonal level
Household demographics
On the SWEAT informational sheet, caregivers will be asked to complete the SWEAT Demographic Survey. The questions on the SWEAT Demographic Survey pertain to: (1) the child(ren)’s sex, age, current grade, ethnicity and race; (2) the primary caregiver’s sex, age, ethnicity and race; (3) the education level and current employment status of the primary caregiver and (4) household income.
Household food security
Household food security will be assessed using the Short Form of the United States Department of Agriculture (USDA) Household Food Security Scale.21 Based on the number of affirmative responses, a food security category or scale score will be calculated.
Substudy
Substudy children will be assessed at baseline (B0; end of the School Year 1/beginning of the summer), time point 1 (T1; middle of the summer between School Year 1 and School Year 2) and time point 2 (T2; end of the summer/beginning of School Year 2).
In additional to the Main Study assessments, the Project SWEAT substudy participants will undergo a more intensive evaluation using mixed quantitative and qualitative methodology. The quantitative portion will be an extension of the survey methodology used with the larger sample to capture information related to the child’s social, food and physical activity environments, as well as dietary and physical activity information about the caregiver (see table 1). The qualitative portion will use the Healthy Eating Active Living: Mapping Attributes using Photographic Participatory Surveys (HEAL MAPPS) methodology22 in order to capture child environmental exposures in a robust fashion, as well as in-depth interview methodology.
Main study measures described above will be assessed with child and caregiver substudy participants. Described below are all additional measures to be assessed with substudy participants
Individual level
Child dietary intake
Three 24-hour dietary recalls—2 weekdays and 1 weekend day—for the child will be completed at time points B0, T1 and T2. The first recall will be completed in person and the following two will be completed over the telephone.23–26 Trained data collectors will use the USDA’s five-step multipass dietary recall method to complete the 24-hour dietary recalls with the caregivers.27–29 The data will be entered into and analysed using the Nutrition Data System for Research (NDSR), V.2015.29 The primary dietary outcomes will include, total fruit servings, total vegetable servings, total fruit and vegetable servings, sugar-sweetened beverage servings, and the Healthy Eating Index30 score.
Child physical activity and sleep
Each participating child will wear a Garmin Vivosmart HR device which has demonstrated validity in certain adult populations31 for three 1-week periods at time points B0, T1 and T2. Garmin devices will be synced to the Garmin Connect app and data downloaded. Then an excel spreadsheet will be generated with variables of interest: total intensity minutes, per cent highly active, per cent active, per cent sedentary, per cent sleep, total step counts, total floors climbed, resting heart rate and time spent in sleep will be obtained.
Child screen time
Participating caregivers will be asked to complete the personal, family and home influences on Physical Activity Questionnaire at times points B0, T1 and T2.32 33 The measure includes questions regarding the number of times per week their child uses sedentary equipment (eg, computer, television, smart phone, tablet).
Child cognition
The term ‘summer setback’ was coined by Entwisle and Alexander and refers to disparities between high-socioeconomic status children and low socioeconomic status children with regard to math and reading skills lost and gained during the summer.34 This trend has been demonstrated in Atlanta,35 Baltimore34 36 and with a national sample of elementary school children.37 These losses in academic strides may not be the only realm of child development at risk during the summer months. The ‘summer setback’ trends that have been well documented over the past couple of decades are being paralleled by emerging trends in unhealthy summer weight gain among economically disadvantaged, racial/ethnic minority children and the association between the two will be explored in Project SWEAT.
Spelling and computational math abilities show the most marked decline over the summer in elementary school-age children.38–41 To assess changes in learning outcomes, child participants in the SWEAT subset will complete four Woodcock-Johnson IV subtests at B0 and T2: letter–word identification, spelling, calculation and applied problems.42
Child emotional eating
To assess the potential impact as a response to emotions that children may be experiencing during the summer months, for example, boredom, the Emotional Eating Scale for Children43 will be used. Children will complete this 26-item self-report measure with trained data collectors at B0, T1 and T2 to determine eating in response to: (1) anxiety, anger and frustration; (2) depressive symptoms and (3) feeling unsettled.43
Caregiver BMI (height and weight)
Caregiver height and weight will be measured by a trained data collector using a Hopkins Road Rod Portable Stadiometer and BalanceFrom High Accuracy Digital Scale at B0, T1 and T2 and BMI will be calculated in kg/m2.
Caregiver waist circumference
Caregiver waist circumference will be assessed using the NHANES waist circumference assessment protocol.18
Caregiver blood pressure
Caregiver blood pressure will be assessed by a trained data collector using an automated, calibrated Panasonic Portable Blood Pressure Monitor.
Caregiver physical activity
The Godin and Shepherd44 Leisure-Time Physical Activity (LTPA) Survey will be used to rank caregivers in terms of their reported LTPA. An LTPA rank score and an ‘active’ or ‘insufficiently active’ category will be calculated.45
Caregiver self-reported health status
The family stress theory attempts to explain the relationship between income, parenting and child outcomes in that lower income parents experience high levels of stress due to lack of income, underemployment and low-wage jobs experience.46–48 These high levels of stress have the potential to negatively change emotions and behaviours—(Health Related Quality of Life (HRQOL)—that impact parenting and in turn their children.46–48 According to McCurdy et al and from support of evidence in the peer-reviewed literature, the family stress model has clear implications for understanding the relationship between poverty and overweight and obesity, especially among children and adolescents.48 Economic stress likely increases the rate of depression, particularly maternal depression.48 This can result in parents, particularly mothers, of young children being unable to execute effective family food behaviours—active and responsive food acquisition strategies (ie, buying in bulk) and management strategies (ie, eating as a family)—and creating an obesogenic food environment.48 To explore the potential relationship between caregiver HRQOL and child weight status during the summer months, the PROMIS-2949 will be completed by trained data collectors with substudy caregivers at B0, T1 and T2.
Caregiver in-depth interviews
Trained data collectors will conduct in-depth interviews with the caregivers at time points B0, T1 and T2 to assess their perceptions of their child’s food and physical activity environments during the summer months. A semistructured in-depth interview guide was developed and contains modified questions used by Tovar et al.50 The Project SWEAT Caregiver In-Depth Interview Guide has been reviewed by nutritionists and dietitians (n=5) for content validity and modified accordingly. All interviews will be audio recorded and transcribed verbatim.
Interpersonal level
Home food inventory
The home food inventory (HFI)51 will be completed by trained data collectors at B0, T1 and T2. The HFI provides a method of assessing availability of foods in the home that have been associated with obesity. An obesogenic home food availability score (0–71) will be calculated.51
Parenting style
The home environment, including caregiver parenting and feeding styles, has been associated with child diet quality and potentially weight status.52–59 The concept of parenting styles—authoritarian, authoritative, permissive and uninvolved—and their influence on child development has been studied for decades.60–64 The 57-item Parenting Dimensions Inventory-Short Form (PDI-S) assesses multiple dimensions of parenting including nurturance, amount of control, consistency, organisation and type of control.65 The caregivers of the SWEAT subset will complete the PDI-S with a trained data collector at B0 and T2.
Caregiver feeding style
At the turn of the century, Hughes et al 66 specified parenting styles in the context of eating interactions as feeding styles with similar demandingness and responsiveness constructs. Despite the similarities of these constructs—parenting styles and feeding styles—they are not synonymous.60 67 68 Research has demonstrated that parenting style may be too broad to impact child eating behaviour, dietary intake, physical activity or weight status.57 60 Due to its specificity to the feeding environment, measuring feeding style instead of parenting style when studying the relationship with childhood obesity may be more informative.60 The caregivers of the SWEAT subset will complete the 24-item Caregiver Feeding Styles Questionnaire66 with a trained data collector at B0 and T2 and caregiver feeding style categories will be assigned accordingly.
Caregiver feeding strategies
Caregiver child feeding practices are one aspect of the home food environment and it is known that caregivers play a critical role in shaping the home food environment, which provides a context for the child’s early eating experiences.69 70 Caregiver feeding practices affect what is offered, timing of food occasions, portion size and social context,69 71 and the data have indicated that caregiver feeding practices affect child food preferences,69 72 73 intake, self-regulation of food intake69 74 and child weight status.69 70 75 76 The caregivers of the SWEAT subset will complete the 31-item Child Feeding Questionnaire 69 with a trained data collector at B0, T1 and T2.
Physical activity environment
A physical activity environment questionnaire was developed and tested by Timperio et al 32 and has also been tested by other researchers.33 The survey assesses several constructs of the physical activity environment including modelling, reinforcement, social support, family-related barriers, rules and restrictions, and home environment (availability and usage of physical and sedentary activity equipment). Caregivers will complete the survey with a trained data collector at B0, T1 and T2.
School teacher in-depth interviews
In-depth interviews will be conducted with school teachers who could provide insight or perceptions on children’s summertime food and physical activity environments because of their engagement with schools during these non-academic months. A Project SWEAT Community Stakeholder In-Depth Interview Guide will be used by a trained data collector during the interview. The SWEAT Community Stakeholder In-Depth Interview Guide has been reviewed by nutritionists and dietitians (n=5) for content validity and modified accordingly. All interviews will be audio recorded and transcribed verbatim. Interviews will be conducted until researchers (n=3) determine that the point of saturation has been reached. Approximately 10–15 interviews are expected to be conducted.
Organizational level
School principal in-depth interviews
In-depth interviews will be conducted with the school principals of the participating schools. See ‘School Teacher In-Depth Interview’ section above for details pertaining to the in-depth interview guide. Four interviews are expected to be conducted.
Summer structured programming audit
The Project SWEAT research team will work with staff at participating schools as well as other community stakeholders (eg, city government and local non-profit organisations) to identify all summer structured programming sites—defined as a place in the community (eg, schools, churches, parks, non-profit organisations) that offer daily meal(s) and child engaging programming during the summer when school is out of session—that service the children at participating schools. A database of all sites with geographical location and contact information will be created and maintained. This audit will serve as a base for other components of the Project SWEAT analysis, that is, Summer Structured Programming Site Environment Assessments and Community Food and Physical Activity Environment Mapping (see Community level).
Community level
Neighbourhood physical activity environment
A trained data collector will complete the Active Neighbourhood Checklist77 for the street segment, defined as a section of road between two consecutive intersections, on which each substudy family resides at time point B0. This 57-item tool was designed to assess five areas—land use, public transit stops, street characteristics, quality of the environment for a pedestrian and places to walk and bike—of the neighbourhood environment that are related to physical activity behaviour.77
Summer structured programming site environmental assessments
A Project SWEAT Site Environmental Assessment form will be completed by site staff for all identified structured programming sites to assess the food and physical activity environments to which children who attend programming are exposed. The SWEAT Environmental Assessment has been modified from an existing tool78 and reviewed by nutritionists and dietitians (n=5) for content validity and modified accordingly.
Community food and physical activity environment mapping
The Project SWEAT research team will work in collaboration with the geographical information system scientists to develop food and physical activity environment maps for the participating schools and surrounding neighbourhoods. All food and physical activity locations within a 1-mile radius of the selected schools will be identified and incorporated onto the maps. At all time points (B0–T2) a trained data collector will observe all identified food and physical activity locations and record the number of children at or using these locations. At each time point, 2 weekdays and 1 weekend day will be observed during the morning, afternoon and early evening hours.
Healthy Eating Active Living: Mapping Attributes using Photographic Participatory Surveys
Community-based participatory research projects (CBPR) is a phenomenon where investigators work in partnership with communities to define social ecological influences on health and identify solutions to make positive changes.79 The process allows for researchers and the target population to codiscover community health determinants and intervention strategies. CBPR builds trust within the community because researchers are seen as responding to their perceived needs.79 HEAL MAPPS is a CBPR tool that can engage communities to address food access issues. Using photography and mapping, HEAL ‘MAPPERS’ navigate regular routes in their community, telling the story of what makes it easy or difficult to access healthy, safe food and physical activity opportunities in socially acceptable ways. Participants will have the opportunity to share their experiences and engage with community stakeholders and decision-makers in finding solutions to challenges concerning access to healthy foods. The result is a community action plan to make communities healthier and more food secure.
HEAL MAPPS was developed by Oregon State University and the steps will be modified by the Project SWEAT research team to catalyse community change22:
Community participants (children with assistance from caregivers) will be trained on digital photography and global positioning systems (GPS) using the Garmin Oregon 650 device. The Project SWEAT subset child participants, with assistance of the primary caregivers, will use a Garmin Oregon 650 device to record barriers and facilitators of eating and physical activity during the summer months through photography
Participants (children) take digital photographs and GPS coordinates of community features that support or inhibit healthy eating and physical activity ‘paths’ (ie, commute to local recreation centre, walk to the nearby corner store, etc). Participants (children) will be given US$20 to spend while they map.
Participants (children and caregivers) and the research team reconvene individually for in-depth interviews to discuss each mapped photograph, and barriers and facilitators to healthy eating and physical activity during the summer months.
Participants (children and caregivers) and the research team reconvene collectively and a focus group will be conducted with the children, with assistance of the primary caregivers, to discuss the photographs taken, barriers and facilitators of healthy eating and physical activity during the summer months.
Using geographical information systems, the Project SWEAT research hub then will overlay the selected pictures onto community maps according to where they were taken. The photomaps and possibly some other data sources (ie, maps of Supplmental Nutrition Assistance Program(SNAP) authorised retailers, USDA Summer Food Service Programme feeding sites, etc) will be used to develop a presentation for the community. The research team uses the presentation to facilitate a ‘community conversation’ with stakeholders in a focus group format. Stakeholders will provide opinions about each of the features and answer questions about community readiness to make changes.
Using qualitative research techniques, the Project SWEAT research hub will organise the stakeholder opinions to develop a community action plan based on the community’s readiness to change.
The community will use the plan to improve environments so they better support healthy eating and physical activity.
Policy level
Community stakeholder in-depth interviews
In-depth interviews will be conducted with other community stakeholders (ie, volunteers at the schools, local non-profit organisations, etc) who could provide additional insight or perceptions on children’s food and physical activity environments during the summer months, as well as facilitators and barriers to improving those environments. See ‘School Teacher In-Depth Interview’ section above for details pertaining to the in-depth interview guide. Approximately 10–15 interviews are expected to be conducted.
HEAL MAPPS community action plan
See the Healthy Eating Active Living: Mapping Attributes using Photographic Participatory Surveys section, particularly steps 6 and 7.
Statistical analyses
Specific aim #1
Assess child weight gain trajectory during the summer months among a convenience sample of economically disadvantaged school-aged children who are and are not engaged in daily structured programming.
Summary statistics for anthropometric and biometric measures, as well as demographic characteristics, will be calculated. To assess the association between participation in structured programming and summer weight gain, a hierarchical linear model (HLM) analysis will be conducted with zBMI as the outcome and attendance as the predictor. An HLM analysis will be employed as it is likely that families will have multiple children in the grade range of kindergarten through fourth grade. Thus, attendance will be the level 1 variable, and household characteristics (income, race, ethnicity, etc) will be the level 2 variables.
Similarly, to assess the association between participation in structured programming and child blood pressure and child waist circumference, two HLM analyses will be conducted with child blood pressure and child waist circumference as the outcomes and attendance as the predictor.
Specific aims #2 and #3
Specific aim #2: Examine the social, food and physical activity environmental settings during daytime, weekday hours of economically disadvantaged school-aged children who are and are not engaged in daily structured programming during the summer time through coupled qualitative (HEAL MAPPS, in-depth interviews, etc) and quantitative (dietary recall, survey, etc) methods and the relation of these factors with weight gain trajectory over the summer period. Specific aim #3: Examine the health behaviours (diet, physical activity, screen time, sleep) of economically disadvantaged school-aged children who are and are not engaged in daily structured programming during the summer time through coupled qualitative (HEAL MAPPS, in-depth interviews, etc) and quantitative (dietary recall, accelerometry, survey, etc) methods and relation of these factors with weight gain trajectory over the summer period. For quantitative measures, variables will be added to the specific aim #1 models as covariates (mediators) or interaction terms (moderators) and impact of the addition of these factors into the models will be assessed.
All dietary and activity photographs from the HEAL MAPPS methodology will be analysed using quantitative photograph analysis and coding.80 81 A priori codes for the photographs will be developed by the researchers (n=3) and the codebook will be modified as necessary based on the photographs received from the children. Each photograph will be assigned a code. Frequencies and proportions of photograph codes and environmental scales (Home Food Environment, Caregiver Feeding Style, Caregiver Feeding Strategies and Physical Activity Environment) will be calculated and compared by change in weight status and participation in structured programming during the summer months.
Specific aim #4
Determine the child, caregiver and household factors (ie, age, ethnicity, income, neighbourhood, food security, etc) that prevent or promote participation in structured summer programming, as well as potential factors that enhance beneficial effects that result from involvement in programming. Potential child, caregiver and household factors will be added to the specific aim #1 models as covariates (mediators) or interaction terms (moderators) and impact of the addition of these factors into the models will be assessed.
Additional analyses
For the community environment assessment mapping observation data, counts will be calculated and analysis of variance tests will be conducted to determine temporal differences in child presence at food and physical activity locations throughout the summer months. These data will be used as formative data to determine what children are doing and where they are spending their time during the summer months.
All in-depth interviews including community stakeholder, child and caregiver in-depth interviews will be audio recorded and transcribed verbatim to preserve the emic terminology. Data analysis will be guided by grounded theory.82 Line-by-line open coding will be conducted by researchers (n=3) to determine emerging themes and constant comparative analysis will be employed to develop a codebook to derive focused codes from all interviews.
Note: Given the formative nature of the research, a formal sample size calculation is not appropriate and therefore not performed.
Patient and public involvement
Community stakeholders and key informants were involved in the study design and development of recruitment methods. Results from this study will be disseminated to study participants via community stakeholder meeting.
Ethics and dissemination
Results from this study will be disseminated in publications for practitioners, scientists and stakeholders.
Discussion
Despite the recent plateau in prevalence, the number of obese children remains high, which is problematic given the negative short-term and long-term health consequences.5 83 84 Emerging research has indicated that summertime is a particular window of risk for unhealthy weight gain among children, especially economically disadvantaged, racial/ethnic minority children.1 2 Unfortunately, there is a near complete dearth of information regarding the health behaviours and environmental settings of economically disadvantaged school-age children during the summer months.
The purpose of this paper is to describe the aims and research methods of Project SWEAT, a prospective, observational cohort study rooted in the socioecological framework to assess factors in multiple levels of the social and physical environments to which children are exposed that may be contributing to this national trend in excessive weight gain among school-age children during the summer months. To our knowledge, this is the first study of its kind in which a robust, mixed-methods approach with innovative, novel assessment strategies will be used.
At the conclusion of this project, it is expected that compared with non-participating children, the children who routinely participate in daily structured summer programming, will manifest improved diet and physical activity behaviours, and a more positive food, physical activity and social environment, which may reduce the risk of inappropriate weight gain during the summer and ultimately obesity. This study can be expected to have a significant positive impact by providing information on the factors that protect at-risk children from unhealthy summer weight gain, which can be used by stakeholders at the local, state and federal level to reform current policy to increase child participation in health promoting programming during the summer.
Acknowledgments
Study participants and staff.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
Footnotes
Contributors CG led conceptual development of the study with input from LCH and BJ. LCH and CG developed the study methodology with input from BJ. LCH and CG wrote the manuscript with input from BJ, CE and CP. All authors read and approved the final manuscript.
Funding This study was supported by United States Department of Agriculture, North Central Nutrition Education Center of Excellence (Grant number: GRT00041857).
Competing interests None declared.
Patient consent Not required.
Ethics approval This study is approved by The Ohio State University Behavioral and Social Sciences Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.