Article Text

Abstract
Objective We reviewed cohort studies to determine the magnitude and temporal direction of the association between recent intimate partner violence (IPV) and a range of adverse health outcomes or health risk behaviours.
Design Systematic review and meta-analysis.
Methods Medline, EMBASE and PsycINFO were searched from the first record to November 2016. Recent IPV was defined as occurring up to and including the last 12 months; all health outcomes were eligible for inclusion. Results were combined using random-effects meta-analysis.
Results 35 separate cohort studies were retrieved. Eight studies showed evidence of a positive association between recent IPV and subsequent depressive symptoms, with a pooled OR from five estimates of 1.76 (95% CI 1.26 to 2.44, I2=37.5%, p=0.172). Five studies demonstrated a positive, statistically significant relationship between depressive symptoms and subsequent IPV; the pooled OR from two studies was 1.72 (95% CI 1.28 to 2.31, I2=0.0%, p=0.752). Recent IPV was also associated with increased symptoms of subsequent postpartum depression in five studies (OR=2.19, 95% CI 1.39 to 3.45, p=0.000), although there was substantial heterogeneity. There was some evidence of a bidirectional relationship between recent IPV and hard drug use and marijuana use, although studies were limited. There was no evidence of an association between recent IPV and alcohol use or sexually transmitted infections (STIs), although there were few studies and inconsistent measurement of alcohol and STIs.
Conclusions Exposure to violence has significant impacts. Longitudinal studies are needed to understand the temporal relationship between recent IPV and different health issues, while considering the differential effects of recent versus past exposure to IPV. Improved measurement will enable an understanding of the immediate and longer term health needs of women exposed to IPV. Healthcare providers and IPV organisations should be aware of the bidirectional relationship between recent IPV and depressive symptoms.
PROSPERO registration number CRD42016033372.
- substance misuse
- public health
- mental health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first systematic review of cohort studies to measure the magnitude of the association and temporal direction between recent exposure to intimate partner violence (IPV) and health outcomes.
As the review considers a broad range of outcomes, we identified gaps in the evidence base, including a need for cohort studies on recent IPV and non-communicable diseases such as cardiovascular disease hypertension and obesity, as well as post-traumatic stress disorder and anxiety disorder.
Due to the large number of abstracts retrieved and the limited timeframe for the review, we were not able to employ double screening of abstracts; however, two researchers conducted the review of the final set of full-text papers, with a third reviewer of all full text papers where there was uncertainty about their inclusion.
As some studies measured the outcome variable (either IPV or the health condition) continuously, it was not possible to combine all measures of effect, which limited the number of studies in the meta-analysis.
It was not possible to quantitatively assess publication bias, as too few studies were in the meta-analysis of each health condition.
Background
Worldwide, almost a third (30%) of all women who have been in a relationship have experienced physical and/or sexual violence by their intimate partner.1 2 Women’s lifetime exposure to intimate partner violence (IPV) is associated with myriad health outcomes. Systematic reviews of longitudinal data find that women who have been physically and/or sexually abused by their partner at some point in their life are twice as likely to have an abortion, twice as likely to suffer from depression, and in some regions are 1.5 times more likely to acquire HIV compared with women who have not experienced IPV.2 Not surprisingly, given its high prevalence and adverse health effects, lifetime exposure to IPV is estimated to result in a high burden of disease. IPV is the second most common risk factor for disability-adjusted life years globally in women aged 20–24 years.3
In our previous systematic reviews, we began to explore the relationships between ‘ever’ exposure to IPV and depressive symptoms and alcohol use, which revealed evidence of a bidirectional association. Devries et al 4 found evidence suggestive of an association between IPV and incident depressive symptoms (OR=1.97, 95% CI 1.56 to 2.48), as well as an association in the reverse direction between depressive symptoms and incident IPV (OR=1.93, 95% CI 1.51 to 2.48). In another systematic review the authors found increased odds of alcohol use following IPV (OR=1.25, 95% CI 1.02 to 1.52) and increased odds of IPV following alcohol use (OR=1.27, 95% CI 1.07 to 1.52).5
Although available evidence finds important associations between IPV and a range of mental and physical health outcomes, the nature of the associations is not always clear. It is possible that exposure to IPV results in subsequent mental and physical health outcomes, that different mental and physical health conditions increase the risk of subsequent IPV, or that a bidirectional relationship is present.
Both IPV and some associated health outcomes, such as depression, anxiety and substance abuse, are chronic, episodic conditions, which can occur with varying frequency over longer time periods. Studies that measure lifetime exposure to IPV therefore hide the complexity of the relationship between IPV and mental and physical health outcomes. This is because estimates of ‘ever’ exposure to IPV are heterogeneous, and may include anything from past year, before the past year and more distant experiences of IPV. Recent violence may lead to more severe health outcomes, but this may be influenced by duration and severity, for example, recent violence with no history versus recent violence experienced as part of ongoing historical abuse.
In the current systematic review, we build on this by closely examining the issue of temporality with regard to recent exposure to IPV and a broader range of health outcomes. In this paper we aim to (1) review what health outcomes have been examined in cohort studies of recent IPV (‘recent’ defined here as IPV experienced up to and including the last 12 months); (2) quantify the magnitude of the association between IPV and different health outcomes; and (3) examine the temporal direction of IPV and health outcomes.
Methods
A systematic review protocol was registered on PROSPERO on 18 March 2016 (CRD42016033372) and is available at http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42016033372.
Literature searches
We searched Medline, EMBASE and PsycINFO from the first record up to 27 January 2016 (with an updated search conducted in November 2016). Terms for IPV were adapted from a previous systematic review on the prevalence of IPV and health outcomes, which was conducted for the 2010 Global Burden of Disease of IPV.1 Controlled vocabulary terms and text words related to longitudinal studies were used for each database. In order to ensure a wide yield of studies, terms for specific health outcomes were not included. An example of search strategy appears in online supplementary appendix 1. Reference list screening was undertaken for key systematic review papers. One study was included from a systematic review on IPV and perinatal mental health disorders published in 2017, which we identified while this paper was under review.
Supplementary file 1
Inclusion criteria
English-language publications.
Longitudinal studies reporting on female participants aged 15 and over were considered. Studies were deemed longitudinal if either the exposure or the outcome was measured on at least two occasions.
Studies where IPV was conceptualised as the independent variable, or where IPV was the dependent variable, in order to capture any evidence of bidirectional causality.
All author definitions of recent IPV victimisation that occurred up to and including 12 months prior.
All author definitions of women-related health outcomes that were measured on at least two occasions.
A 12-month cut-off period was chosen for recent IPV as this is the most commonly used period for prevalence estimates, it is consistent with internationally recognised IPV measures,6 7 and has been used in a number of intervention studies for IPV.8–10
Screening and data extraction
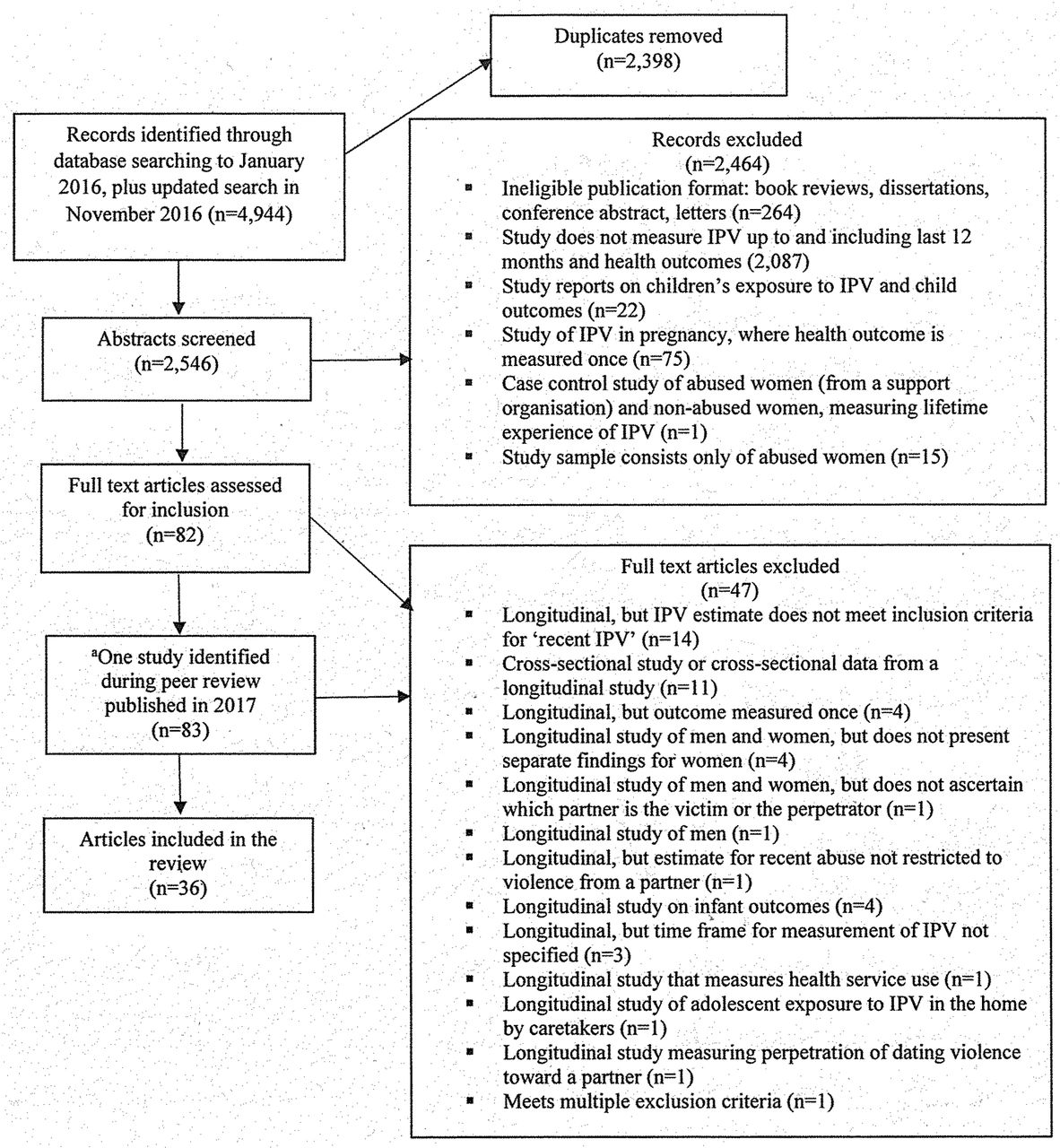
Records were initially screened by one reviewer (LJB), and studies not meeting the inclusion criteria were removed. Full-text articles were reviewed by one reviewer (LJB), and where there was uncertainty about the inclusion of an article it was referred to the senior author (KD). The final set of full-text articles was formally appraised by two reviewers (LJB and MR). Data were extracted and entered into an Excel spreadsheet by one reviewer (LJB). The study selection process including the number of studies, abstracts and full texts screened with reasons for exclusion is summarised in the flow chart in figure 1.

Flow of studies through review. aNew systematic review published in 2017 on domestic violence in pregnancy and perinatal mental health disorders identified by editorial team during the peer review of our paper. IPV, intimate partner violence.
Quality appraisal
The quality of each effect estimate was appraised and presented in table 1, which corresponds to the major relevant domains of potential bias in quality assessment tools. Consideration was given to whether definitions of IPV and health outcomes were based on valid, reliable measures. We considered whether studies controlled for potential confounders for two reasons. IPV and the health outcomes of interest commonly occur episodically over a period of time, and episodes of either that are incident over the study period may be a continuation of previous IPV or health outcomes. Therefore, we examined whether studies adjusted for time 1 levels (ie, at the beginning of the study period) of the outcome variable. Additionally, IPV and the health outcomes of interest are associated with demographic characteristics and other risk factors that may explain the association between them, such as childhood sexual abuse. Due to the complexity of the potential causal pathways between IPV and the health outcomes, we did not specify a minimum set of confounders that should be adjusted for. Additionally, it has been noted that it is not always appropriate to adjust for baseline levels of an outcome variable in longitudinal studies. When exposures are associated with baseline health status, bias can arise if change in health status preceded baseline assessment or if the dependent variable measurement is unreliable or unstable.11 However, we recorded whether key variables were adjusted for and examined the results in the light of these adjustments. Information was also extracted in relation to mode of administration of surveys, length of follow-up, number of waves and attrition rates.
Quality assessment of 36 papers reporting on 35 studies included in the review and effect estimates
Data analysis
Analyses were conducted by LJB and KD using Stata V.14.0. Study characteristics and quality are summarised descriptively. Studies reported a range of effect estimates (eg, ORs, relative risks and correlation coefficients). Adjusted ORs were extracted directly from the publications, with the exception of one unadjusted OR which was calculated for a study on perceived stress, which is not one of the health outcomes included in the meta-analysis. Studies measured IPV or health outcomes in heterogeneous ways; therefore, the results are summarised descriptively for each health outcome. Where there were at least two estimates, random-effects meta-analysis was used to calculate the pooled ORs representing associations between IPV occurring up to and including the last 12 months and various health outcomes. Higgins’ I2 statistic, which describes the percentage of variability in point estimates that is due to heterogeneity rather than sampling error,12 was calculated. Some studies reported multiple estimates using overlapping definitions of IPV on the same sample of participants. In order to avoid double counting participants in these studies, which can lead to falsely precise pooled estimates, preference was given to one estimate using the following algorithm implemented in the following sequence: (1) those derived from multivariate analysis, (2) where the definition of IPV closely matched that of the other studies in the meta-analysis, (3) where the reference group was unexposed to any violence and (4) where the estimate was most precise (ie, the smallest CI). This algorithm was applied to three studies. Studies that provided multiple estimates, but on different subsamples of participants were included in the meta-analysis. Studies that reported other types of estimate (eg, correlations coefficients, betas, risk ratios) are documented separately.
Patient and public involvement
Patients and the public were not involved in this systematic review.
Results
Study characteristics
Thirty-five separate cohort studies described in 36 articles published between 2002 and 2017 with 48 863 participants met the inclusion criteria and contained 174 effect estimates of association between IPV and health outcomes. Eighteen articles were from the USA,13–30 three from Australia,31–33 two from New Zealand,34 35 three from South Africa,36–38 two from India,39 40 one from Puerto Rico,41 one from Spain,42 one from Korea,43 one from Nicaragua,44 one from Kenya,45 one from Japan,46 one from the UK47 and one from Tanzania.48 Among the 35 cohort studies, 11 were household surveys,13 19 27 28 32 35 39 43 44 47 49 14 sampled participants from clinical settings,14 20 21 23 25 26 30 31 33 40 42 45 46 48 7 from schools16 17 22 24 29 36 50 and 3 from the local community.15 38 41 Some studies were based on subpopulations of women, including one study (reported in two papers) of women receiving methadone maintenance treatment,20 21 women attending a clinic with depressive symptoms at baseline,31 HIV-positive female sex workers45 and eight studies of pregnant women.30 33 38 40 42 46–48 Six studies focused on adolescents16–18 22 24 29 and one (reported in two papers) included women and young girls.36 37
Table 2 presents the different health outcomes measured in the studies, the number of studies that measure each health condition, the overall number of estimates that contribute to each health condition and the number of estimates that contribute to the meta-analysis.
Health outcomes/health risk behaviours measured in the 35 studies and the number of estimates
Table 1 summarises quality issues in relation to the 36 papers reporting on 35 separate cohort studies included in the review. All but 3 of the 35 cohort studies used recognised, validated IPV instruments or used items that were taken from validated instruments.40 43 47 All but nine studies assessed for IPV that occurred in the last 12 months; one measured IPV in the last 3 months,39 two in the last 6 months,20 21 23 one in the last 4 months,29 four measured IPV that occurred during pregnancy,40 46–48 and one measured IPV during or within 12 months of pregnancy.30 Most of the studies assessed for physical and/or sexual violence from a partner, with some also including threats, emotional or verbal abuse. The attrition rate was reported or calculated in 19 studies and ranged from 4.6%48 to 37.4%.31 The length of follow-up ranged from 1 month46 to 10 years,49 and the number of waves ranged from two (multiple studies) to six.33 The smallest sample size was 73 adolescents29 and the largest was 1303 adult women.48 Table 1 presents all study estimates grouped by health outcome.
IPV and depressive symptoms
Thirteen studies examined the relationship between recent IPV and depressive symptoms,13 17 19 22–26 31 32 37 39 43 of which one examined the association in both directions.43 Of these, nine studies provided nine estimates of association between IPV and subsequent depressive symptoms.13 19 22 23 25 31 32 39 43 Eight of these estimates showed a positive direction of association between experience of IPV and subsequent depressive symptoms.9 13 19 22 23 31 32 39 Of the nine estimates of the association between IPV and subsequent depression, all but two reached statistical significance.25 39 Five studies provided five estimates of association between depression and subsequent IPV, all of which showed a positive and statistically significant relationship.17 24 26 37 43
We were able to include seven estimates reporting binary IPV measures and binary depressive symptoms or disorder measures in the meta-analysis. For IPV and subsequent depressive symptoms or disorder, the pooled OR from five estimates13 25 31 32 39 was 1.76 (95% CI 1.26 to 2.44, I2=37.5%, p=0.172). Two estimates17 37 were included in the meta-analysis of the relationship between depressive symptoms and subsequent IPV, resulting in a pooled OR of 1.72 (95% CI 1.28 to 2.31, I2=0.0%, p=0.752). One study, not included in the meta-analysis, examined the bidirectional relationship between IPV and depression.43 A Korean study of married women found that IPV at wave 1 was positively associated with the depression level at wave 1 (beta=0.030, SE=0.03, p<0.001), but negatively associated with the growth rate of depression over the study period (beta=−0.03, SE=0.01, p=0.004). IPV experienced at wave 4 was associated with a larger growth rate of depression in the model (beta=3.34, SE=0.61, p<0.001) and the experience of IPV at wave 1 (beta=0.68, SE=0.11, p<0.001) (see figure 2).

Forest plot estimates of the association between intimate partner violence and depression. Woolhouse et al 33 estimates are based on different subsamples and are mutually exclusive. Meta-analysis with depression as the dependent variable was also undertaken excluding the Chowdhary and Patel39 study which removes women with baseline depressive disorder from the analysis, but it did not materially change the overall pooled estimate (OR=1.85, 95% CI 1.35 to 2.49, I2=35.1%, p=0.202).
Depression measurement
Of the nine studies that measured IPV and subsequent depressive symptoms, one measured depressive symptoms occurring in the past 12 months,25 one in the last 2 weeks,31 five in the last week,13 19 22 32 43 one ‘current’39 and one did not specify a time period.23 Of the five studies that measured depressive symptoms and subsequent IPV, three measured depressive symptoms in the past week,17 37 43 one in the past 6 months24 and one did not specify a time period.26
All but one of the studies used screening questionnaires that measured depressive symptoms as opposed to diagnostic tools. Of the 13 studies, eight used the Center for Epidemiological Studies-Depression Scale,13 17 19 22 23 32 37 43 one study used the WHO International Classification of Diseases, 10th Revision,39 one used the Composite International Diagnostic Interview-Short Form (CIDI-SF),25 one used the Patient Health Questionnaire,31 one used the Beck Depression Inventory (BDI)26 and one used a scale from Kandel and Davies.24
Common risk factors/confounding
Of the nine studies that measured IPV and subsequent depressive symptoms and disorder, all but one controlled for time 1 levels of depression. Chowdhary and Patel39 excluded women with baseline depressive disorder in their analysis, but this may have resulted in the exclusion of cases of IPV that preceded depressive symptoms at baseline and the remaining cases may not have been representative of women experiencing IPV. All but one of the five studies that measured depressive symptoms and later IPV controlled for time 1 levels of IPV.26 Of the 13 studies, all but 2 controlled for sociodemographic factors.26 39 Other confounders were not comprehensively controlled for. Two studies controlled for childhood physical and/or sexual abuse17 31 and two for alcohol use,24 37 of which one also controlled for childhood adversity which measured emotional and physical neglect, and physical and sexual abuse.37 There were no discernible differences in effect estimates regardless of which confounders were adjusted for, and studies found similar directions and varying magnitudes of association.
IPV and postpartum depressive symptoms
Eight studies provided eight estimates of association between IPV and subsequent postpartum depressive symptoms.30 33 38 40 42 46–48 All eight estimates showed a positive direction of association between IPV and subsequent postpartum depressive symptoms, with all but one of the estimates reaching statistical significance.46 Seven estimates from five studies were included in the meta-analysis of the relationship between IPV and subsequent postpartum depression,30 33 42 47 48 resulting in a pooled OR of 2.19 (95% CI 1.39 to 3.45). This was heterogeneous (I2=79.8%, p=0.000). One of the studies examined the bidirectional relationship and found that depression symptom severity was associated with a greater risk of subsequent IPV.38 Each 5-point difference in the Edinburgh Postnatal Depression Scale (EPDS) was associated with a 0.9-point to 2.3-point difference in subsequent IPV risk (beta=0.054, 95% CI 0.030 to 0.079).
Postpartum depression measurement
Of the eight studies that measured IPV and subsequent depressive symptoms, one measured depressive symptoms occurring in the past 12 months,42 six studies measured depressive symptoms in the last week33 38 40 46–48 and one study did not specify the time period.30 One study measured postpartum depression in the last week and subsequent IPV.38 Of the eight studies, six used the EPDS,33 38 40 42 47 48 one used the Hospital Anxiety and Depression Scale46 and one used the BDI.30
Common risk factors/confounding
Six of the eight studies that examined IPV and subsequent postpartum depression controlled for time 1 levels of depressive symptoms.30 33 38 42 46 47 One study did not control for time 1 levels of depressive symptoms as it was not significant in the bivariate analysis.48 Five studies controlled for sociodemographic factors.33 38 42 46 48 One study controlled for HIV serostatus38 and one controlled for HIV/AIDS diagnosis.48
IPV and alcohol use
Ten studies examined the relationship between recent IPV and alcohol use. Of these, eight studies provided 15 estimates of association between IPV and subsequent alcohol use.14–16 19 21 27–29 35 49 All but one of these 15 estimates showed a positive direction of association between IPV and subsequent alcohol use,15 with two studies providing 4 estimates which reached statistical significance.27 49 Three studies21 28 29 provided three estimates showing a positive direction of association between alcohol use and subsequent IPV, of which one was statistically significant.29
For IPV and later alcohol use, the pooled OR from six estimates provided by three studies16 21 35 was 1.19 (95% CI 0.91 to 1.55, I2=0.0%, p=0.523). Three estimates from two studies21 28 were included in the meta-analysis of the relationship between alcohol use and subsequent IPV, resulting in a pooled OR of 1.11 (95% CI 0.91 to 1.35, I2=0.0%, p=0.672).
Alcohol use measurement
Of the eight studies that measured IPV and subsequent alcohol use, five measured alcohol use in the last 12 months,15 16 27 35 49 two in the last 6 months14 21 and one in the last 30 days.19 Of the three studies that measured alcohol use and subsequent IPV, one measured alcohol user in the last 12 months,28 one in the last 4 months29 and one in the last 6 months.21 Alcohol consumption was measured in a variety of ways. Of the 10 studies, one assessed alcohol abuse or dependence using the CIDI-SF,49 four measured binge drinking which was based on the number of alcoholic drinks consumed on one occasion,14 16 21 35 three measured heavy drinking which was assessed using a combined quantity–frequency measure,27–29 one used the Alcohol Dependence Scale and the Michigan Alcohol Screening Test,15 and one used the National Survey of Alcohol and Drug Abuse.19
Common risk factors/confounding
Of the eight studies that measured IPV and subsequent alcohol use, only four adjusted for time 1 levels of alcohol use.14–16 27 Of the three studies that examined the association between alcohol use and subsequent IPV, all but one adjusted for time 1 levels of IPV.21 Of the 10 studies, 7 controlled for sociodemographic factors.14–16 21 27 28 35 Two studies adjusted for a history of trauma. El-Bassel et al 21 controlled for childhood sexual abuse, post-traumatic stress disorder, multiple concurrent partners and frequency of condom use. Gilbert et al 14 also controlled for childhood sexual abuse, as well as psychological distress, coping strategies, the partner’s illicit drug use and binge drinking and sexual relationship power. Regardless of the confounders controlled for, all but one study found a positive direction of association and reported varying magnitudes of association.27
IPV and hard drug use (crack, cocaine, heroin)
Four studies examined the relationship between recent IPV and hard drug use,14 21 28 41 of which one reported an association in both directions.21 Two studies provided two estimates of IPV and subsequent hard drug use, both of which showed a positive direction of association, although only one was statistically significant.21 41 The pooled OR from these studies was 2.05 (95% CI 1.19 to 3.52, I2=0.0%, p=0.948). Three studies provided four estimates of hard drug use and subsequent IPV, which showed a positive direction of association and three of these were statistically significant.14 21 28 Three of these estimates were included in the meta-analysis, resulting in a pooled OR of 2.20 (95% CI 1.52 to 3.17, I2=0.0%, p=0.455).
Hard drug use measurement
Of the two studies that measured IPV and subsequent hard drug use, one study measured drug use in the last 12 months41 and the other in the last 6 months.21 Of the three studies that measured hard drug use and subsequent IPV, one assessed use in the last 12 months28 and two in the last 6 months.14 21 Of the four studies, two used the Drug Use and Risk Behaviour Questionnaire14 21 and two asked about use of specific hard drugs including crack, cocaine and heroin.28 41 Of the latter, one of the studies used two methods for assessing hard drug use at each wave, including self-report information only and combined self-report and toxicological information.41
Common risk factors/confounding
Of the two studies that measured IPV and subsequent hard drug use, one controlled for time 1 levels of hard drug use.41 Of the three studies that measured hard drug use and subsequent IPV, two controlled for time 1 levels of IPV.14 28 All four studies controlled for sociodemographic factors. El-Bassel et al 21 controlled for childhood sexual abuse, post-traumatic stress disorder, multiple concurrent partners and frequency of condom use. Gilbert et al 14 controlled for childhood sexual abuse, psychological distress, coping strategies, the partner’s illicit drug use and binge drinking and sexual relationship power.
IPV and marijuana use
Four studies examined the relationship between recent IPV and marijuana use,14 16 21 28 of which two studies reported an association in both directions.14 21 Three studies provided three estimates of IPV and subsequent marijuana use, all showing a positive direction of association, although none were statistically significant.14 16 21 Two of these studies were included in the meta-analysis, resulting in a pooled OR of 1.52 (95% CI 1.04 to 2.24, I2=5.4%, p=0.304). Three studies provided four estimates of marijuana use and subsequent IPV,14 21 28 of which one showed a positive and statistically significant relationship. Three of these estimates were included in the meta-analysis, resulting in a pooled OR of 1.96 (95% CI 0.8 to 4.83). This was heterogeneous (I2=85.4%, p=0.001).
Marijuana use measurement
Of the four studies, two measured marijuana use in the last 12 months16 28 and two in the last 6 months.14 21 All studies used self-report information to assess for marijuana use.
Common risk factors/confounding
Of the three studies that measured IPV and subsequent marijuana use, two controlled for time levels of marijuana use.14 16 Of the three studies that measured marijuana use and subsequent IPV, two controlled for time levels of IPV.14 28 All the studies controlled for sociodemographic factors. El-Bassel et al 21 controlled for childhood sexual abuse, post-traumatic stress disorder, multiple concurrent partners and frequency of condom use. Gilbert et al 14 controlled for childhood sexual abuse, psychological distress, coping strategies, the partner’s illicit drug use and binge drinking and sexual relationship power.
IPV and STIs (excluding HIV)
Three studies provided three estimates of the association between recent IPV and subsequent sexually transmitted infections (STIs),20 39 45 of which one showed a positive and statistically significant relationship.39 The meta-analysis of two of these studies20 39 resulted in a pooled OR of 1.10 (95% CI 0.56 to 2.18, I2=35.5%, p=0.214).
STI measurement
One study assessed for STIs (chlamydia, gonorrhoea or trichomoniasis) within the last 3 months using biological measures,39 another relied on self-report to assess for STIs at the last wave,20 and the third study assessed women quarterly for gonorrhoea, chlamydia or trichomoniasis using biological measures.45
Common risk factors/confounding
All the studies controlled for sociodemographic factors. El-Bassel et al’s study21 of women attending a methadone maintenance clinic adjusted for time 1 HIV risk factors (ie, frequency of condom use, frequency of requesting condom use, having unprotected anal sex, exchanging sex for drugs, being HIV-positive and having had an STI), as well as drug and alcohol use. Chowdhary and Patel39 removed women with an STI at time 1 from the analysis. However, this would likely have introduced bias in the resulting cases, as it would have excluded women with IPV that preceded the acquisition of an STI at baseline. Wilson et al’s45 study of HIV-positive sex workers did not control for time 1 sexual risk behaviours, although it did control for a lifetime history of sexual violence since the age of 15 by someone other than the index partner. Figure 3 presents the forest plots for alcohol use, hard drug use, marijuana use and STIs.

{kind=link}
{kind=link}
{kind=link}
Discussion
Summary of main findings
Our review identified cohort studies that examined the relationship between recent IPV (ie, IPV occurring up to and including the last 12 months) and depression, postpartum depression, alcohol use, hard drug use, marijuana use and STIs. Although a few other health or health-related outcomes were identified (ie, sexual risk behaviours, HIV infection, general anxiety, perceived stress and gynaecological problems), these could not be included in a meta-analysis because there was only one estimate. We found evidence consistent with a bidirectional relationship between recent IPV and depressive symptoms. Recent IPV was also associated with increased symptoms of postpartum depression. There was some evidence of a bidirectional relationship between recent IPV and hard drug use, and IPV and subsequent marijuana use, although there were a limited number of studies. There was no evidence of an association between recent IPV and alcohol or STIs, although the evidence was weak with few studies and inconsistent measurement of alcohol and STIs.
Although the search strategy did not limit the types of health outcomes identified, the review found no cohort studies for recent IPV exposure and non-communicable diseases such as cardiovascular disease, hypertension and obesity. Nor did we find longitudinal evidence for recent experience of IPV and post-traumatic stress disorder or anxiety disorder. There is limited evidence from cross-sectional data that lifetime IPV increases the risk of cardiovascular disease.51 Cohort studies measuring history of IPV have reported an association with increased body mass index,52 increased risk for cardiovascular disease53 and hypertension.54 Physiological mechanisms may explain the association between IPV and some adverse health outcomes through complex neural, neuroendocrine and immune responses to acute and chronic stress. For example, sustained and acute elevated stress levels have been linked to cardiovascular disease, hypertension, gastrointestinal disorders and chronic pain. When exposed to prolonged or acute stress, areas of the brain (eg, hippocampus, amygdala and prefrontal cortex) undergo structural changes that can impact on mental and cognitive functioning, which can lead to mental disorders.55
We found evidence consistent with a bidirectional relationship between recent experience of IPV and depressive symptoms. The magnitude of the association in either direction is similar to that reported in our previous review of ‘ever’ IPV and depressive symptoms,4 although there were fewer estimates in our meta-analysis of recent IPV and depressive symptoms.
All the studies on postpartum depressive symptoms conceptualised IPV as the dependent variable and there was evidence that recent experience of IPV or IPV during pregnancy increased symptoms of subsequent postpartum depression, although there was substantial heterogeneity. The magnitude of the association was slightly lower (OR=2.19, 95% CI 1.39 to 3.45) compared with Howard et al,56 who reported a threefold increase in the levels of depressive symptoms in the postnatal period after having experienced IPV during pregnancy (OR=3.1, 95% CI 2.7 to 3.6). However, the authors state that study heterogeneity and lack of data on baseline symptoms prevented conclusions on temporality. In addition, we excluded one study that was included in the Howard et al 56 review as it measures postnatal depressive symptoms using the EPDS at the final wave, but assesses common mental health disorders during pregnancy with the Self-Reporting Questionnaire-20.57 A recently published systematic review explored studies of IPV during pregnancy and perinatal mental disorders in low-income and middle income countries. However, most of the studies were cross-sectional and considered partner violence experienced during pregnancy. Furthermore, estimates were not pooled in a meta-analysis.58
There was no evidence of an association between recent IPV and alcohol use in either direction. This might be because there were fewer estimates in the meta-analysis of recent IPV, and measurement of problematic alcohol use was conceptualised in a number of different ways, for example, binge drinking, heavy episodic drinking and high-risk alcohol use, which may have diluted the effect. None of the estimates in the meta-analysis measured alcohol use disorder. Furthermore, not all the estimates in the meta-analysis controlled for time 1 levels of alcohol use, and only one included the perpetrator’s alcohol use, which may be related to IPV and/or the woman’s drinking behaviour. This finding is in contrast to our previous review of ‘ever’ IPV and alcohol use, which did find evidence consistent with a bidirectional relationship.5 Although the pooled estimates in both reviews are based on studies that assess binge drinking, the Devries et al 5 review includes estimates of IPV that occurred in the distant past (ie, before the last 12 months).
Our review found evidence consistent with a bidirectional relationship between recent IPV and hard drug use. However, this finding should be treated with caution as there were very few studies overall, and one of the studies was based on a sample of women attending a methadone maintenance clinic. For marijuana use, there were few studies, but the evidence suggests that IPV predicts subsequent marijuana use. Pooled estimates did not support that marijuana use predicts subsequent IPV, although estimates were heterogeneous. The evidence for recent IPV and STI infection was in conflicting directions and there were only two estimates. Our review adds to previous systematic reviews as it focuses on longitudinal studies that measure recent experiences of IPV. Furthermore it includes a broader range of health or health-related outcomes and explores bidirectionality. The review also highlights that longitudinal studies on recent IPV are lacking for important health outcomes that are known to be associated with partner violence.
Limitations of the review
To our knowledge, this is the first systematic review of cohort studies to measure the magnitude of the association between recent exposure to IPV and health outcomes/health risk behaviours. Although we conducted an extensive search of the global literature, the review has a number of limitations. Due to the large number of abstracts retrieved and the limited timeframe for the review, we were not able to employ double screening of abstracts. Citation tracking was not undertaken, although we conducted reference list screening of key systematic review papers. However, two researchers reviewed the final set of included papers, with a third reviewer of all full text papers where there was uncertainty about their inclusion. One researcher was responsible for extracting data from included papers. As some studies measured the outcome variable (either IPV or the health condition) continuously, it was not possible to combine all measures of effect, which limited the number of studies in the meta-analysis. However, we comment on the direction of the association of studies that were not included in the meta-analysis in the Results section for each health condition. It was not possible to quantitatively assess publication bias as too few studies were in the meta-analysis of each health condition.
Sources of bias and limitations of included studies
One of the main limitations of the included studies relates to the lack of consistency in controlling for key potential confounders. With regard to studies on depression, hard drug use and marijuana use, most controlled for time 1 levels of the health condition or IPV (where IPV was the dependent variable). Far fewer of the estimates on IPV and later alcohol use and IPV and STI controlled for time 1 levels of the health outcome.
With regard to the studies on depressive symptoms, only two controlled for early childhood trauma (ie, childhood sexual and/or physical abuse) and two controlled for alcohol use, even though both are known to increase the risk for depression.59 60 This makes it difficult to rule them out as potential contributors to the causation of the outcomes. Nevertheless, we found that studies showed a positive direction of association, regardless of which variables were adjusted for, and there was no clear pattern of differing magnitude of association that indicated the relationship between IPV and depressive symptoms was not likely to be entirely accounted for by shared risk factors.
Little is known about the potential causal mechanisms between depression and subsequent IPV. However, women who are depressed may experience symptoms (eg, lethargy and withdrawal) that impact their capacity for engaging in self-care behaviours including help-seeking and contact with healthcare providers that could enable them to extricate themselves from the relationship. It is also plausible that earlier, perhaps unmeasured experiences of violence, such as childhood sexual abuse and trauma, are causing depression and later IPV, or that depression is mediating the relationship between childhood sexual abuse and later IPV. A path analysis with cross-sectional data supports this hypothesis,60 but few longitudinal studies have explored these relationships.
Only two studies on alcohol use controlled for childhood sexual abuse and one controlled for the partner’s level of alcohol use, both of which are potential causes of women’s alcohol use. It has been suggested that women who drink heavily are more likely to have a partner who drinks heavily, which can increase their risk of IPV because heavy alcohol use by men is associated with IPV perpetration.61 This can occur because people tend to choose a partner with similar drinking patterns to themselves or through the influence of their partner’s drinking patterns and expectations.62 Research also suggests that the partner’s or the woman’s drinking may fuel conflict in the relationship. A nationally representative study from the USA found that couples with similar drinking patterns (eg, both abstinent or both binge drinkers) were less likely to experience IPV in their relationship compared with those with discordant drinking habits.63 This implies that relationship conflict may result in IPV, as opposed to alcohol use alone because high alcohol use would be more predictive than discordant use. Alcohol use was measured in a variety of ways, with most assessing binge drinking or heavy drinking and only two studies measuring alcohol dependence. Although heavy alcohol consumption increases the risk for disease, injury and premature death,64 65 the adverse consequences may vary considerably between people who sporadically drink heavily and those who develop an alcohol use disorder. Although the evidence points to a bidirectional relationship between IPV and hard drug use and IPV and marijuana use, there were few estimates. Women may self-medicate with alcohol, tobacco or drugs in an attempt to cope with the trauma and stress of living in an abusive relationship, which in themselves are important risk factors for poor health. However, alcohol or substance abuse by the abuser or the woman has also been identified as a trigger to violent episodes or a factor that contributes to more severe violence.66 The evidence for the association between recent IPV and STIs is uncertain.
It was not possible to examine whether the duration or severity of the violence influenced the relationship between IPV and health. Studies conceptualised violence as physical, sexual, verbal or emotional (or psychological), with most using a combination of types of violence. Only one study provided estimates of minor and severe violence. Studies reported the timeframe in which the violence occurred, but not the duration.
The majority of the studies were from high-income countries, most notably the USA, and only eight studies were from middle-income countries, where it is known that the prevalence of past-year IPV is higher. Six of the studies were of adolescents, again mostly in high-income countries, where these were likely to be in dating relationships with no cohabitation. One study included young girls and women. Experiences of IPV in adult and adolescent relationships may be qualitatively different, in that there is a lower likelihood of experiencing systematic and chronic violence in dating relationships.67 About a third of the studies were drawn from clinical settings, schools or were taken from subpopulations and therefore subject to bias (eg, HIV-positive sex workers, women with depressive symptoms and women on methadone maintenance). More population-based cohort studies are needed in order to generalise the findings. Most studies measured physical violence and some modelled exposure to physical and sexual and other forms of violence separately. However, other forms of violence (eg, emotional abuse, threats) may also be associated with some of the health outcomes. Most studies constructed the reference categories for IPV as binary opposites, meaning that some participants in the reference group may have been exposed to other forms of IPV that were not measured or modelled. This can bias the effect estimates towards the null and underestimate the magnitude of the association between recent IPV and health outcomes. Some studies included only women who were in a relationship for all waves of data collection. However, research shows that the prevalence of IPV is higher among women who are no longer with abuser compared with those currently in a relationship,68 and excluding these women may dilute the association between IPV and health outcomes.
Implications
The evidence on the association between exposure to IPV and mental and physical health outcomes has important implications for the delivery of interventions and services. IPV against women has received increasing attention from public health experts globally.2 The results of this review indicate that healthcare providers and specialist IPV organisations should be aware of the bidirectional relationship between recent IPV and depression. Women with depression may be at risk of IPV, including IPV that is ongoing, and services, particularly healthcare, should be trained to enquire about IPV experiences and respond and refer appropriately. Little is known about what pattern of exposure to IPV is more strongly associated with different health outcomes. In order to establish these connections, longitudinal studies of IPV and health are needed that distinguish recent violence with no history from recent violence that is part of ongoing abuse and historical violence that no longer occurs. Other factors that are known to mediate the relationship, such as the duration and severity of IPV, childhood physical and sexual abuse, poverty-related stress, and risk behaviours such as alcohol and substance abuse, should be carefully considered in analyses.
References
Footnotes
Contributors Conceived and designed the study: LJB, KD. Data collection: LJB. Analysed the data: LJB, MR, KD. Wrote the first draft of the manuscript: LJB. Contributed to the writing of the manuscript: LJB, CW, KD, MR. Agreed with manuscript results and conclusions: LJB, CW, KD, MR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval All data used in this review were already in the public domain and ethical approval was not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.