Article Text

Abstract
Objectives To conduct a systematic review with meta-analysis of cohort studies to evaluate the association of coffee consumption with the risk of prostate cancer.
Data sources PubMed, Web of Science and Embase were searched for eligible studies up to September 2020.
Study selection Cohort studies were included.
Data extraction and synthesis Two researchers independently reviewed the studies and extracted the data. Data synthesis was performed via systematic review and meta-analysis of eligible cohort studies. Meta-analysis was performed with the “metan” and “glst” commands in Stata 14.0.
Main outcomes and measures Prostate cancer was the main outcome. It was classified as localised prostate cancer which included localised or non-aggressive cancers; advanced prostate cancer which included advanced or aggressive cancers; or fatal prostate cancer which included fatal/lethal cancers or prostate cancer-specific deaths.
Results Sixteen prospective cohort studies were finally included, with 57 732 cases of prostate cancer and 1 081 586 total cohort members. Higher coffee consumption was significantly associated with a lower risk of prostate cancer. Compared with the lowest category of coffee consumption, the pooled relative risk (RR) was 0.91 (95% CI 0.84 to 0.98), I2= 53.2%) for the highest category of coffee consumption. There was a significant linear trend for the association (p=0.006 for linear trend), with a pooled RR of 0.988 (95% CI 0.981 to 0.995) for each increment of one cup of coffee per day. For localised, advanced and fatal prostate cancer, the pooled RRs were 0.93 (95% CI 0.87 to 0.99), 0.88 (95% CI 0.71 to 1.09) and 0.84 (95% CI 0.66 to 1.08), respectively. No evidence of publication bias was indicated in this meta-analysis.
Conclusions This study suggests that a higher intake of coffee may be associated with a lower risk of prostate cancer.
- epidemiology
- prostate disease
- nutrition
Data availability statement
Data are available upon reasonable request. The data are available upon request from the corresponding author (wangkefenguro@sina.com)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Risk of selection and recall bias may be minimised due to the inclusion of prospective cohort studies.
Large sample size ensures adequate statistical power to detect even a small effect of interest.
Uncontrolled/residual confounding may distort the association between coffee consumption and prostate cancer.
Misclassification of coffee consumption may occur due to the self-reported nature of the exposure.
Significant heterogeneity among study results may come from various sources.
Introduction
Prostate cancer is the second most frequently diagnosed cancer and the sixth leading cause of cancer death in men. There were 1 276 000 new cancer cases and 359 000 cancer deaths in 2018.1 It is estimated that nearly three-quarters of prostate cancer cases occur in developed countries.1 Since the 1970s, the incidence of prostate cancer has also increased rapidly in some Asian countries such as China, Singapore and Japan, where the incidence has always been much lower than in some Western countries.1 2 Therefore, primary prevention of prostate cancer is a significant public health problem worldwide.
Coffee is one of the most popular beverages. Since its popularity continues to increase worldwide, even a small effect on individual health may exert a substantial public health impact. Coffee is known to be a major source of dietary caffeine, cafestol and antioxidants in industrialised nations.3 Its various constituents such as caffeine, caffeic acid and chlorogenic acid can potentially impact the development of cancer through multiple carcinogenesis pathways.4 5 Inverse associations were observed between coffee consumption and the risk of cancer in sites such as the liver, colorectum and breast.6 However, previous studies have reported inconsistent results on the association of coffee consumption with the risk of prostate cancer. Although earlier cohort studies did not detect an association,7–15 more recent studies conducted in major Western countries such as the USA, Sweden and the UK reported that coffee consumption was associated with a lower risk of localised and advanced prostate cancer.16–20 In Japan, a country with increasing popularity of coffee, a cohort study also found a significant inverse association between coffee consumption and the risk of prostate cancer.21
Previous meta-analyses of cohort studies up to 2015 reported a significant positive association for coffee consumption on total prostate cancer risk, with highly variable results in different subgroups.22 23 Since then, five cohort studies have explored the association but still reported inconsistent results.24–28 It was hypothesised that higher coffee consumption was associated with an increased risk of prostate cancer. Thus, the objective of this updated meta-analysis was to explore and evaluate the association of coffee intake with the risk of prostate cancer in adult men, and to direct the future primary prevention strategy on prostate cancer.
Methods
This systematic review was conducted and reported in adherence to the PRISMA and MOOSE guidelines29; the corresponding checklists are shown in online supplemental table 1 and online supplemental file 1. Two researchers (YZ and ZT) independently conducted the literature search, study selection, data extraction and study quality assessment. Any discrepancies were resolved by discussion, but whenever consensus could not be reached between the two reviewers, a third reviewer (KW) acted as arbitrator.
Supplemental material
Supplemental material
Patient and public involvement
This is a meta-analysis based on study-level data and no individual-level data were involved in the study or in defining the research question or outcome measures.
Inclusion criteria
The eligibility criteria of the studies were as follows: (1) The study should use a longitudinal cohort design or case–control design nested within a cohort study. (2) The study should present information on coffee consumption as the exposure of interest. Coffee consumption was ascertained by self-reported dietary records or food diaries on the intake levels (highest intake category vs lowest intake category) or frequency measures (eg, per unit/cups/mL per day/week). Since the intake levels were classified and defined differently in each study, the absolute coffee consumption in the highest and lowest intake categories varied across the included studies. (3) The study should report prostate cancer as the outcome of interest. Prostate cancer was defined by clinical diagnosis, physician diagnosis, medical records, self-reports or data linkage to a registry system such as a cancer registry. Based on definitions in each original study, the prostate cancer categories were classified as follows: (a) localised prostate cancer, which included localised or non-aggressive cancers; (b) advanced prostate cancer, which included advanced or aggressive cancers; and (c) fatal prostate cancer, which included fatal/lethal cancers or prostate cancer-specific deaths. (4) The study should provide relative risk (RR), HR, risk ratio, rate ratio or OR estimates with confidence intervals (CIs) or standard errors for the association of coffee consumption with the risk of prostate cancer. If multiple estimates were provided, priority was given to the multivariable-adjusted risk estimates. If more than one study was conducted in the same population, the earlier reports or reports with less applicable information were excluded.
Literature search
A literature search was performed using PubMed, Web of Science and Embase up to September 2020 with the following keywords: coffee and prostate and (cancer or carcinoma or neoplasm or tumour). The full search strategy is shown in online supplemental file 2 The reference lists of relevant publications were also manually searched for identification of additional eligible studies. No language limitation was imposed.
Supplemental material
When data or information in the publication were insufficient, we attempted to contact the corresponding authors of the original study to request the relevant data. Then two authors (Russnes and Nilsson) provided us with the relevant information about the person-years of follow-up for specific categories of coffee intake to facilitate the dose-response analyses.15 20 Of note, we finally did not include the study by Russnes et al20 in the current meta-analysis because the study population is the same as another included cohort study by Wilson et al18 which reported more applicable information.
Data extraction
We extracted the following information from each eligible study: first author’s name, year of publication, study country, follow-up time, number of participants in the cohort, number of prostate cancer cases, assessment of coffee consumption, primary study outcome, definitions and categories of coffee consumption, RRs and 95% CIs for all prostate cancer outcomes associated with coffee consumption, and the potential confounders considered or adjusted in the analysis.
Study quality assessment
The 9-star Newcastle–Ottawa Scale tool was used to assess study quality.30 The quality of each cohort study was judged on three broad categories—namely, selection of the study population, comparability of groups and ascertainment of either the exposure or outcome of interest.
Statistical analysis
In the meta-analysis, the RR estimate was used to measure the association between coffee consumption and the risk of prostate cancer in this meta-analysis. We pooled the study-specific RR estimates for the highest versus the lowest category of coffee consumption. A fixed effects model was used to pool the study-specific estimates; whenever significant heterogeneity was detected, the random effect model was used to address the heterogeneity across studies.31 Subgroup analyses were conducted stratified by study location, prostate cancer stage and potential confounder adjustments including a history of prostate-specific antigen (PSA) testing, a family history of prostate cancer, total energy intake, cigarette smoking, alcohol consumption, physical activity, body mass index (BMI) or history of diabetes. Since PSA testing was generally introduced after 1986,32 studies with follow-up periods that ended before 1986 were classified in the PSA-adjusted group. To explore the influence of each study on the pooled results, sensitivity analyses were also performed by excluding one study at a time and then repeating the meta-analysed approach.
We further examined the potential dose–response relationship between coffee consumption and the risk of prostate cancer. When the mean coffee intakes in each category were not reported, the midpoint values in each category were used instead; when the upper boundary of the highest intake category was not presented, we calculated the midpoint value assuming that the highest category had the same magnitude of intake as the preceding category.33 34 The pooled RR for each increment of one cup of coffee per day was estimated using the method proposed by Orsini and Greenland.35 We examined a potential non-linear relation between coffee consumption and prostate cancer risk by modelling coffee consumption using restricted cubic splines for non-linear trends with 4 knots at fixed percentiles (5%, 35%, 65% and 95%) of the distribution.36 Non-linearity of the association was explored by testing the null hypothesis that the coefficients of the second and third splines were equal to zero.
We assessed the heterogeneity by using the Q and the I2 statistic. A p value <0.10 or an I2 >50% suggest that statistical heterogeneity may exist.37 Small study effects such as publication bias were evaluated by funnel plots, as well as Begg’s test and Egger’s test.38 39 Meta-analysis was conducted using the “metan” and “glst” commands in Stata version 14.0 (StataCorp, College Station, Texas, USA). Two-sided p values <0.05 were considered statistically significant in the meta-analysis.
Results
Literature search
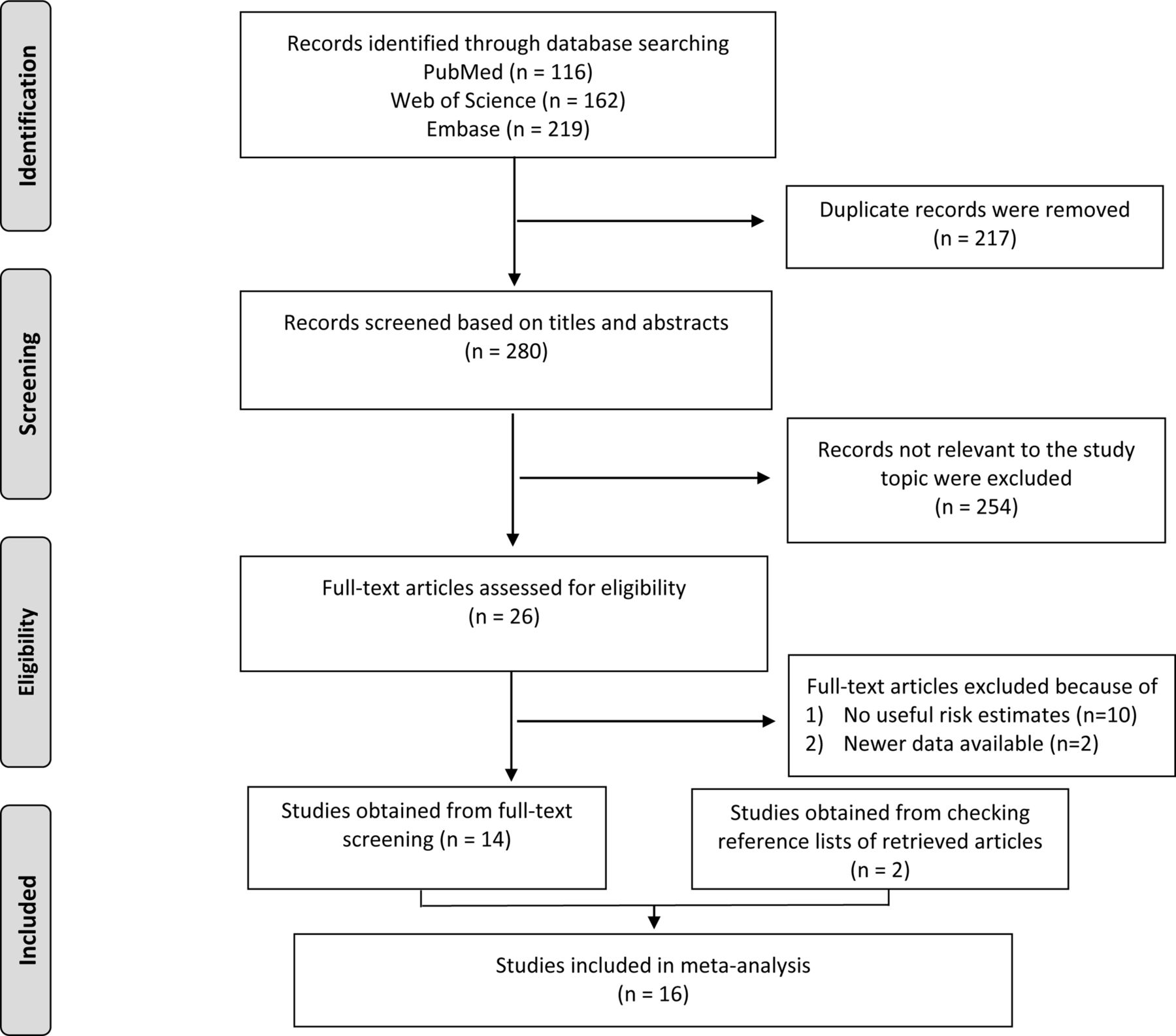
We identified 497 records after searching the three databases. After 217 duplicate records were removed, 280 records remained for screening of titles and abstracts, and after screening the titles and abstracts, 254 irrelevant records were excluded. Following a further full-text review of the 26 remaining studies, 10 studies were excluded because of no useful risk estimates or 95% CIs; two studies were excluded as newer data or more informative data were available. Fourteen studies were obtained from full-text screening and a further two studies were identified by checking the reference lists of retrieved articles.9 11 Thus, 16 studies were included in the final analysis,9–11 13–19 21 24–28 of which 15 reported on the risk of prostate cancer associated with the highest versus the lowest coffee consumption9–11 13–19 21 24–27; 13 studies reported the risk associated with an increase of one cup of coffee per day or provided sufficient data to estimate the dose–response risk9 13–19 21 24 25 27 28 (figure 1).

Flow diagram of study selection in the meta-analysis.
Study characteristics and quality assessment
The characteristics of the eligible cohort studies are shown in online supplemental file 3. The included studies were conducted in North America (n=7), Europe (n=7) and Japan (n=2). There was a total of 1 081 586 men in the 16 cohort studies, of whom 57 732 developed prostate cancer. To measure coffee consumption, 11 studies used food-frequency questionnaires and five used a self-administered dietary questionnaire. Most studies considered or adjusted for the most potential confounders in the analysis, such as age at baseline, family history of prostate cancer, race, cigarette smoking, alcohol drinking, total energy intake, BMI and physical activity. The results of study quality assessment are presented in online supplemental file 4. The total scores for each cohort study ranged from 6 to 9. Fourteen studies awarded a total score of ≥7, which were considered as relatively high-quality studies with a low risk of bias.
Supplemental material
Supplemental material
Overall analyses and dose–response analyses
The reported RRs for the original cohort studies ranged from 0.47 (95% CI 0.25 to 0.87) in the study by Pounis et al to 1.42 (95% CI 0.77 to 2.61) in the study by Ellison et al (figure 2). Compared with the lowest coffee intake category, there was a 9% reduction in the risk of prostate cancer for the highest category (RR=0.91; 95% CI 0.84 to 0.98). Statistically significant heterogeneity was detected across the studies (p=0.008, I2=53.2%). In dose–response analyses, we found evidence of a linear inverse association between coffee consumption and prostate cancer risk (p=0.006 for linear trend) (figure 3). The pooled RR of prostate cancer was 0.988 (95% CI 0.981 to 0.995) for an increase of one cup of coffee per day. No evidence of a non-linear relationship was observed between coffee consumption and risk of prostate cancer (p=0.193 for non-linearity). Moreover, there was no indication of small study effects such as publication bias from the results of the Egger’s test (p=0.409), Begg’s test (p=0.843) as well as the funnel plot. The funnel plot and Egger’s publication bias plot are shown in online supplemental file 5.
Supplemental material

Forest plot for the association between coffee consumption and prostate cancer risk.

Dose–response relationship of coffee consumption with prostate cancer risk.
Subgroup and sensitivity analyses
As shown in table 1, compared with the lowest coffee intake category there was a 7% reduction in risk for the highest intake category (RR=0.93; 95% CI 0.87 to 0.99) for localised prostate cancer. For advanced and fatal prostate cancer, the corresponding pooled RRs were 0.88 (95% CI 0.71 to 1.09) and 0.84 (95% CI 0.66 to 1.08) (figure 4). When stratified by study location, the pooled RRs were 0.96 (95% CI 0.90 to 1.03), 0.85 (95% CI 0.74 to 0.98) and 0.85 (95% CI 0.48 to 1.51) for studies conducted in North America (six in the USA and one in Canada), European countries and Japan. Furthermore, significant inverse associations were observed in all of the confounder adjusted subgroups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for the association between coffee consumption and risk of prostate cancer stratified by cancer stages.
Summary risk estimates and corresponding 95% CIs for prostate cancer associated with the highest versus the lowest coffee consumption
In sensitivity analyses, we sequentially excluded one study at a time and recalculated the pooled RRs of the remaining studies. The pooled RRs did not change substantially, ranging from 0.89 (95% CI 0.82 to 0.97) to 0.93 (95% CI 0.86 to 1.00) after omission of the studies by Hashibe et al and Terdal et al, respectively.
Discussion
Summary of the findings
In this meta-analysis, higher coffee consumption was significantly associated with a reduced risk of prostate cancer in men. In the dose–response analysis, a reduction in the risk of prostate cancer of nearly 1% was observed for each increment of one cup of coffee per day. The combined estimate for prostate cancer was robust across subgroup and sensitivity analyses.
Comparison with other studies
The previous meta-analysis detected a statistically significant positive association between coffee consumption and prostate cancer risk (RR=1.16; 95% CI 1.01 to 1.33).22 However, this observed effect was confined to case–control studies (RR=1.21; 95% CI 1.03 to 1.43), with no significant association in cohort studies (RR=1.06; 95% CI 0.83 to 1.35) when stratified by study design.22 Considering the case–control design, patients with prostate cancer might differentially recall their past coffee consumption habits compared with healthy controls, which might generally lead to biased estimates. This potential recall bias could generate a spurious positive association between coffee consumption and prostate cancer risk. Additionally, selection bias, which can occur in case–control studies, may distort the association between coffee consumption and prostate cancer risk. In another meta-analysis of cohort studies with 539 577 participants and 34 105 prostate cancer cases, the pooled RR for the highest category of coffee intake was 0.90 (95% CI 0.85 to 0.95) for total prostate cancer compared with the lowest intake category. In this updated meta-analysis of 1 081 586 cohort members and 57 732 incident cases, the overall result was similar to the previous one. However, for subgroups of localised, advanced and fatal prostate cancers, the strength of associations tended to be weaker compared with the previous study.
Possible biological mechanisms
It is biologically plausible that coffee may reduce the risk of prostate cancer in men. Coffee improves glucose metabolism, decreases concentrations of plasma insulin and insulin-like growth factor-1, has anti-inflammatory and antioxidant effects, and affects sex hormone levels, all of which may play roles in the initiation, development and progression of prostate cancer.3 18 20 40 Coffee is also a major source of chlorogenic acids; intake of quinides, the degradation products of chlorogenic acids, has been observed to increase insulin sensitivity and lower blood glucose levels.3 Moreover, coffee intake may be associated with increased levels of adiponectin plasma,41 42 which may act as an endogenous insulin sensitiser.43 Higher adiponectin levels in plasma are supposed to relate to lower concentrations of plasma insulin.43 In two prospective studies, insulin levels were observed to be directly associated with prostate cancer-specific mortality.44 45
Coffee is a major contributor of dietary antioxidants such as caffeic acid and chlorogenic acid.20 A prospective cohort study from the USA found that dietary antioxidants from coffee (eg, caffeic acid) were inversely associated with the risk of total, advanced and lethal prostate cancer.20 It was suggested that antioxidants protect cells from damage caused by oxidative stress and inflammation, which may further lead to neoplastic transformation in the prostate.46 Additionally, dietary antioxidants may inhibit prostate cancer progression through suppression of oxidative stress, which might play a critical role during the progression of prostate cancer.46 Coffee intake was indicated to be related to increased levels in sex hormone-binding globulin (SHBG), as well as total testosterone.47 48 A pooled analysis of 18 prospective studies found that SHBG levels may be inversely associated with the risk of prostate cancer.40 Of note, a nested case–control study found that caffeine or caffeinated coffee intakes were suggested to be associated with an increased level of plasma SHBG. However, such an association was not observed between decaffeinated coffee and plasma SHBG levels. Thus, it was suggested that caffeine may be the key component in coffee, which may be responsible for determining plasma SHBG levels.48
Strengths and limitations
A strength of this study was the inclusion of prospective cohort studies. Cohort studies could minimise the risk of selection and recall bias, which is a major concern for case–control design. Besides, large numbers of total cohort members and prostate cancer cases ensure adequate statistical power to detect even a small effect of interest. Furthermore, the dose–response analysis may further lend confidence to the study hypothesis that increased coffee consumption was linearly associated with a lower risk of prostate cancer. Besides, most of the studies were of high quality with a low risk of bias, which could further lend confidence to the current pooled results.
This meta-analysis also has several limitations. First, one weakness is that only three databases were searched for eligible studies and other databases, especially non-English databases, were not considered in the literature search. Second, because of the observational design, unmeasured or uncontrolled confounders in the original studies may bias the pooled risk estimate; however, the residual confounding effects from the original studies were difficult to handle in a meta-analysis approach.49 50 For example, the inverse association between coffee consumption and prostate cancer could be attributed to risk factors related to coffee consumption, such as physical activity and healthy diet. However, most of the original studies have considered or adjusted for these major potential confounders in the analysis. In the sensitivity analysis of restricting the meta-analysis in studies considering most confounders, the strength of association tended to be larger in comparison with the overall association. Third, misclassification of coffee consumption may occur because of the self-reported nature of exposure measurement. However, validation studies by diet records indicated a relatively high validity of coffee consumption measured by food frequency questionnaire. The correlations between questionnaire and diet records were 0.80 in US men,16 0.71 in Swedish men17 and 0.72 in Japanese men.21 Of note, misclassification of exposure would most likely be non-differential in cohort studies and bias the observed association toward the null.49 50 Therefore, the true association between coffee consumption and risk of prostate cancer may be even stronger. Fourth, since coffee intake and the incidence of prostate cancer in the USA and Europe are relatively high, most of the studies were conducted in these regions. Since the effect size is small, we should be cautious when generalising the results to other areas, especially where the incidence is relatively low. Last, significant between-study heterogeneity may limit interpretation of the results. The observed heterogeneity may come from various sources. For example, the highest and lowest categories of coffee intake are different in the original studies. Studies with a broader range between the highest and lowest categories were assumed to generate a higher risk estimate. Moreover, the type of coffee and different brewing methods included in the coffee consumption groups differed. The different cohort sizes and follow-up periods may also lead to heterogeneous results. Taken together, due to the significant heterogeneity in the current meta-analysis, the pooled results should be interpreted with caution.
Conclusions
This study suggests that increased coffee consumption may be associated with a reduced risk of prostate cancer. Further research is still warranted to explore the underlying mechanisms and active compounds in coffee. If the association is further proved to be a causal effect, men might be encouraged to increase their coffee consumption to potentially decrease the risk of prostate cancer.
Data availability statement
Data are available upon reasonable request. The data are available upon request from the corresponding author (wangkefenguro@sina.com)
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the authors of the original studies for their contribution to our meta-analysis, especially those authors who provided their raw data for the analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors KW obtained the funding, developed the research design, interpreted the results and also had primary responsibility for the final content. XC, YZ and ZT analysed the data and interpreted the results. XC and KW drafted manuscript. All authors critically reviewed and approved the manuscript.
Funding This work was supported by the Natural Science Foundation of Liaoning Province of China (Grant No 2019-MS-3608) for Kefeng Wang and 345 Talent Project of Shengjing Hospital of China Medical University for Kefeng Wang (Grant No M0122).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.