Article Text

Abstract
Objective To identify and assess the performance of clinical decision rules (CDR) for chest pain in general practice.
Design Systematic review of diagnostic studies.
Data sources Medline/Pubmed, Embase/Ovid, CINAHL/EBSCO and Google Scholar up to October 2018.
Study selection Studies that assessed CDRs for intermittent-type chest pain and for rule out of acute coronary syndrome (ACS) applicable in general practice, thus not relying on advanced laboratory, computer or diagnostic testing.
Review methods Reviewers identified studies, extracted data and assessed the quality of the evidence (using Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2)), independently and in duplicate.
Results Eight studies comprising five CDRs met the inclusion criteria. Three CDRs are designed for rule out of coronary disease in intermittent-type chest pain (Gencer rule, Marburg Heart Score, INTERCHEST), and two for rule out of ACS (Grijseels rule, Bruins Slot rule). Studies that examined the Marburg Heart Score had the highest methodological quality with consistent sensitivity (86%–91%), specificity (61%–81%) and positive (23%–35%) and negative (97%–98%) predictive values (PPV and NPV). The diagnostic performance of Gencer (PPV: 20%–34%, NPV: 95%–99%) and INTERCHEST (PPV: 35%–43%, NPV: 96%–98%) appear comparable, but requires further validation. The Marburg Heart Score was more sensitive in detecting coronary disease than the clinical judgement of the general practitioner. The performance of CDRs that focused on rule out of ACS were: Grijseels rule (sensitivity: 91%, specificity: 37%, PPV: 57%, NPV: 82%) and Bruins Slot (sensitivity: 97%, specificity: 10%, PPV: 23%, NPV: 92%). Compared with clinical judgement, the Bruins Slot rule appeared to be safer than clinical judgement alone, but the study was limited in sample size.
Conclusions In general practice, there is currently no clinical decision aid that can safely rule out ACS. For intermittent chest pain, several rules exist, of which the Marburg Heart Score has been most extensively tested and appears to outperform clinical judgement alone.
- coronary heart disease
- primary care
- medical history
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study provides an up-to-date overview on chest pain rules applicable in general practice.
We applied stringent inclusion criteria and standardised quality assessment tools.
Various diagnostic study designs were included (ie, derivation, validation).
Chest pain rules that relied on advanced diagnostic testing (ie, HEART, TIMI or GRACE) were not included.
Decision rules based on exclusively non-chest pain symptoms (ie, dyspnoea) were not part of the literature search.
Introduction
Chest pain is a common symptom for contacting the general practitioner (GP). During office hours, 1.5% of all consultations and 4% of all new episodes are related to chest pain.1–5 The highest frequency of chest pain consultations is in the age category 45 to 64 years, with notable differences between men and women in its presentation.1 3 4 6 The initial task for GPs is differentiating less frequent but urgent diagnoses of chest pain, such as acute coronary syndrome, or pulmonary embolism, from more common but less urgent diagnoses (such as gastro-oesophageal reflux, musculoskeletal pain or anxiety).1–5 To make this important differentiation, GPs mainly depend on history taking, medical history, physical examination and past experience to establish a working hypothesis/diagnosis. The most prevalent reason for referral is rule out of acute coronary syndrome (ACS) in patients with acute-onset chest pain as well as rule out of coronary artery disease (CAD) in patients who present with intermittent-type chest pain.
The GPs’ evaluation of patients with chest pain, based on symptoms and signs alone (‘clinical gestalt’), is unfortunately insufficient for diagnosing or excluding stable angina and particularly ACS reliably (sensitivity of 69% and specificity of 89%).7 GPs are very well aware of their own limitations and therefore apply a low referral threshold. A validated clinical risk score could aid GPs in decision-making by calculating the risk of an unfavourable diagnosis based on patient characteristics, symptoms and other readily available information. In this systematic review, we aim to identify and assess the performance of existing clinical decision aids/rules for stable angina and/or acute coronary syndrome in patients with chest pain that are applicable and have been validated in low-resource general practice or equivalent settings.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to undertake this review.8
Data sources and searches
We searched PubMed, Embase, CINAHL and Google Scholar from database inception through to the search date 17 October 2018. We searched for studies written in English, Dutch or German. We used keywords: chest pain, coronary artery disease, acute coronary syndrome, general practice, primary care practice, prediction rule, decision model or decision aid. Online supplement A of the supplemental data document displays the full search strategy.
Supplementary file 1
Study selection
Two investigators (REH, SCL) identified potentially eligible studies, with a third (WAML) to resolve any disagreements. We used an online systematic review platform (Covidence, Veritas Health Innovation, Melbourne, Australia) for this purpose. In addition to the language (English, Dutch, German) and human research restrictions, the following inclusion criteria for eligible studies were applied: (1) original studies in adults (≥18 years of age) with enrolment in a primary care setting; (2) chest pain either acute or intermittent-type; (3) ascertainment of the diagnosis of coronary artery disease or acute coronary syndrome at follow-up; (4) predictive tool based on multivariable analysis; (5) predictive tool derived from findings that are applicable in primary care setting. These findings may include: medical history, physical examination, ECG or previously documented laboratory findings (such as lipid levels). We excluded studies with a retrospective study design and studies that used a prediction rule that was based on serial biomarker testing (ie, sequential troponin testing at 2–3-hour time interval), required advanced computer algorithms or advanced diagnostic testing (cardiac imaging, coronary angiography).
Clinical decision rules and outcomes of interest
The clinical decision aids may include items from history taking, physical examination, laboratory and electrocardiographic data. The outcomes of interest are diagnostic test characteristics of included rules, including: sensitivity, specificity, negative and positive prediction values.
Reference diagnosis
The clinical outcomes that we used as reference diagnosis were (1) any form of coronary artery disease (CAD) or coronary heart disease; or (2) a more restricted form including unstable angina or myocardial infarction (referred to as acute coronary syndrome) in patients with acute chest pain. We applied no restrictions on minimum or maximum time of follow-up. The assessment of applicability of the reference standard for each study is assessed by the QUADAS-2 tool, which can be found as supplemental data in online supplement B.
Study population
We included studies with adult populations that present at a GP office or out-of-office setting (ie, patient visits when making house calls). In-hospital, emergency department (ED) and/or preselected outpatient populations were not eligible.
Data extraction and quality assessment
Two investigators (REH, SCL) extracted data elements from each study, with a third investigator (WAML) independently reviewing these data for accuracy. The quality of the studies was assessed by three investigators (REH, SCL, WAML) using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool for assessing risk of bias in diagnostic accuracy studies. This tool comprises four key domains, namely: patient selection, index test, reference standard and flow and timing.9 We assessed whether a clinical decision rule (CDR) was ready for application in clinical practice based on the level of evidence for each rule using the definitions of the Mount Sinai Evidence-Based Medicine Working group.10
Data synthesis and analysis
The extracted data on study and patient characteristics, outcome measures and follow-up information of the included studies will be displayed in tables. Subsequently, we extracted data on the discriminatory properties (C-statistic) of the decision rule from each studies, as well as data on sensitivity, specificity, positive (PPV) and negative predictive values (NPV) and true and false positives and negatives. We constructed a summary receiver operating characteristic curve based on 2×2 tables from the individual study data using Review Manager (RevMan V.5.3. The Cochrane Collaboration, Copenhagen, Denmark).
Patient and public involvement
This study did not involve direct patient involvement. For the current analysis, we did not a priori consult with representatives of patient organisations. After peer review and acceptance of publication, we will share the findings of our research with the Dutch Heart Foundation, relevant patient organisations, as well as general practitioners within our academic network.
Results
Search results
Our search resulted in 3105 unique studies of which we assessed 94 in full text. Of those, eight studies met the inclusion criteria of our study, in which five different CDRs were evaluated. All studies were written in English. The flowchart of our search strategy and reasons for exclusions can be found in figure 1.

Flow chart of systematic search of the literature. ACS, acute coronary syndrome; CAD, coronary artery disease; ED, emergency department.
Quality assessment
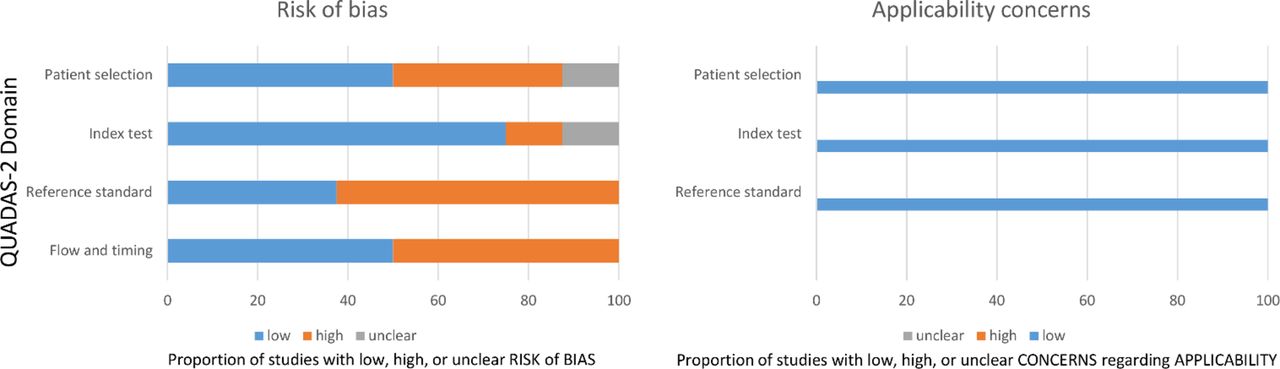
The overall quality of the studies was moderate as graphically displayed in figure 2. In six out of eight studies, we found a high risk of bias in the reference standard, as the assessors who determined the final diagnosis (delayed type) were not blinded to the index test results. In three studies, we found a high risk of bias in patient selection as a significant proportion of patients were excluded prior to enrolment.11–13 Also, in four studies, a high risk of bias was found in flow and timing, due to relatively high dropout rates of patients.7 12–14 In one study, >15% of participating GPs stopped recruiting prematurely.7 Quality concerns of the pooled individual data study (INTERCHEST) included possible bias due to missing data in >20% of the study population and unverifiable risks of bias regarding patient selection.14 Details of the quality assessment can be found as online supplement B in the supplemental data file.
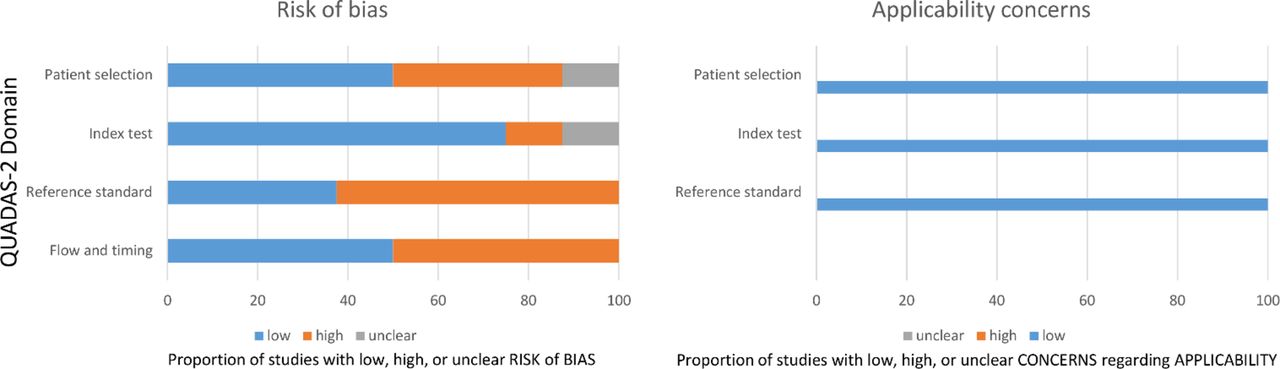
Quality assessment by QUADAS-2.
Study and patient characteristics
As shown in table 1, a total of seven single cohort studies were included involving 6959 patients and one pooled individual data study from five cohorts (INTERCHEST) involving 3099 patients. The sample size of the individual cohort studies ranged from 289 to 1249 patients. Studies were conducted in Europe and the USA and were published 1995 and 2017. All studies were conducted in general practice, with two studies mandating immediate work-up of all patients at the ED.12 13 The prevalence of CAD, with a variable diagnostic follow-up period of up to 1 year, ranged from 8.0% to 15.0%. In three studies concentrating on acute-onset chest pain, the prevalence of ACS ranged from 22.0% to 47.8%.11–13 The reported mean age of patients ranged from 41 to 67 years, with women comprising 44% to 58% of the population. In studies that reported the prevalence of comorbidities, hypertension (45%–50%) and dyslipidaemia (31%–41%) were common, and diabetes was present in approximately 13%. The inclusion and exclusion criteria as well as the definitions that were used for the reference diagnoses for each of the studies can be found as online supplement C and D in the supplemental file.
Characteristics of the study design and study population
Clinical decision rules
We identified a total of five CDRs, namely the Gencer rule,7 the Marburg Heart Score,15–17 INTERCHEST,14 Grijseels rule12 13 and Bruins Slot rule.11 As shown in table 2, the CDRs have been developed based on readily available clinical information, such as patient characteristics, medical history and physical examination. The Grijseels rule also requires an ECG. The former three scores (Gencer, Marburg Heart Score and INTERCHEST) were developed for rule out of CAD, whereas the Grijseels and Bruins Slot rules were constructed for rule out of ACS.
Components of the clinical decision rules
Decision rules for stable coronary artery disease in patients with intermittent chest pain
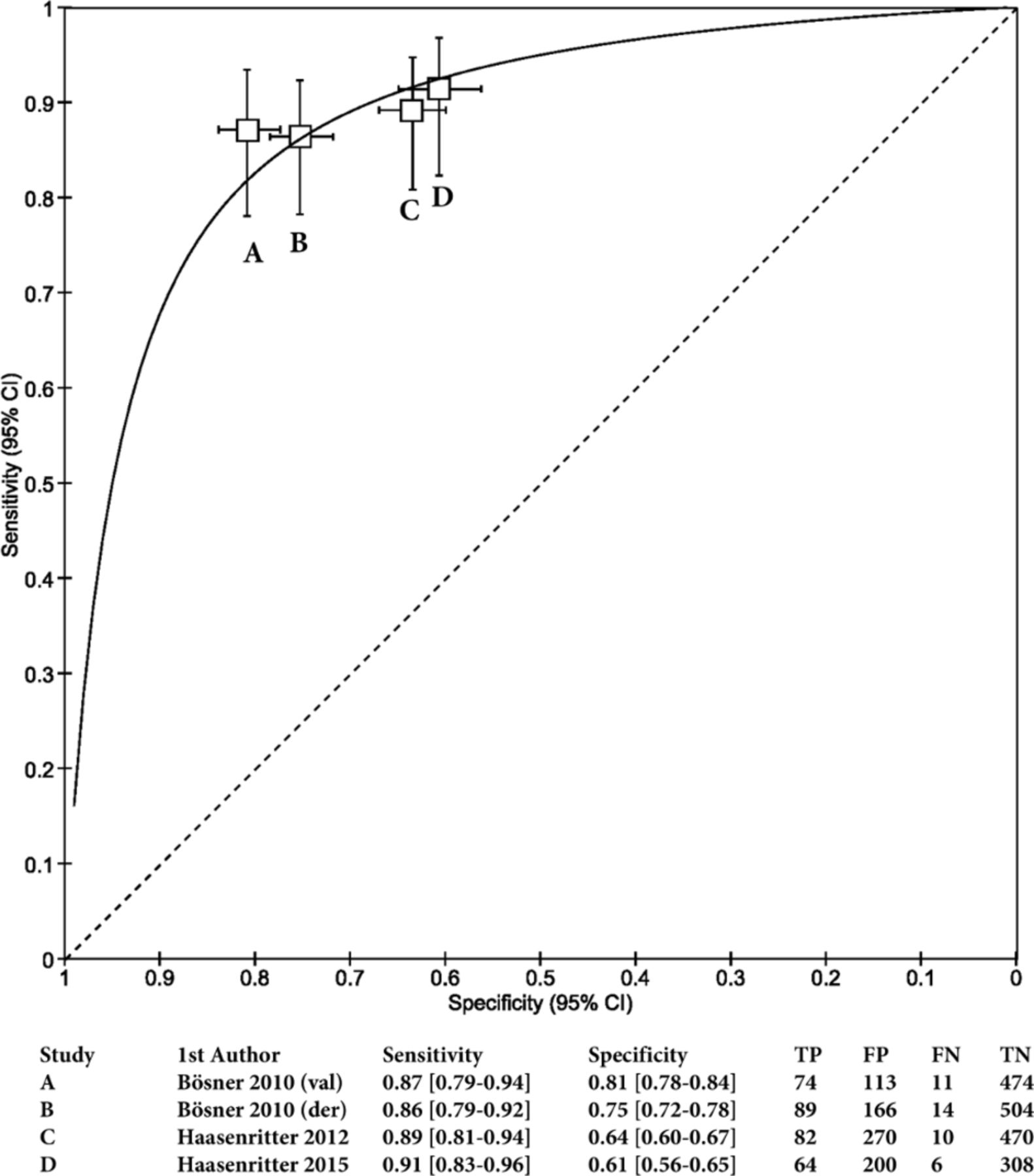
As shown in table 3, the decision aid that was most extensively tested is the Marburg Heart Score. This study has good overall discrimination (C-statistic of 0.84–0.90), with a sensitivity of 86%–89%, specificity of 64%–81%, with a PPV of 23%–40% and a NPV of 97%–98%. The diagnostic properties of the Marburg Heart Score are visualised in figure 3, illustrating its consistent diagnostic performance in terms of sensitivity and specificity. As shown in table 4, The Marburg Heart Score was found to outperform unaided clinical judgement. When used as a decision aid, both the sensitivity (+8.0%) and specificity were higher (+5.8%). Moreover, when the Marburg Heart Score was used for an initial triage tool, it led to higher specificity (+11.6%) with similar sensitivity (−1.5%) compared with unaided clinical judgement. Based on the combined body of evidence, the level of evidence is 2 for the Marburg Heart Score, which implicates that this rule can be used in a general practice setting of low-risk patients with intermittent chest pain with confidence in its accuracy.
{kind=link}
{kind=link}
{kind=link}
Summary receiver operating characteristic curve of specificity and sensitivity of the Marburg Heart Score across the individual studies.
Diagnostic performance data of the clinical decision rules for coronary artery disease*
The clinical judgement of the general practitioner
The other two CDRs for rule out of stable CAD were the INTERCHEST rule and the Gencer rule. The INTERCHEST rule which was derived from a pooled data analysis also shows promise (C-statistic of 0.84, sensitivity 82%–88%, specificity 74%–82%, PPV of 35%–43% and NPV of 96%–98%), but has a number of quality concerns, and has not been compared with unaided clinical judgement. As such, the INTERCHEST rule should not be considered ready for clinical application (level of evidence is 4). The Gencer rule was developed and externally validated in only one study (C-statistic: 0.75–0.95, sensitivity 87%–98%, specificity 42%–71%). Given the limited evidence, the Gencer rule can only be used with caution (level of evidence for its use is 3).
Decision rules designed for acute coronary syndrome
Grijseels et al developed a decision rule for ruling out ACS in general practice in the late 1990s that was later updated by Bruins Slot et al. These studies show that the discrimination of these decision rules was mediocre (C-statistic of 0.66 and 0.72). Unaided clinical judgement provided a better overall fit (C-statistic of 0.75) with a 51% agreement in risk estimation. Other diagnostic properties are listed in table 4. Although the study by Bruins Slot is limited by sample size, it appears that the CDR was safer than clinical judgement alone, as four patients that were considered low risk by the GP (8.2%) were correctly identified as high risk by the decision aid. The INTERCHEST score was also assessed among 169 patients with acute chest pain; the authors found a reasonable overall performance (C-statistic of 0.79). However, data on its test characteristics were lacking, and as such, we are unable to assess its safety and accuracy. Overall, neither the Grijseels, Bruins Slot or INTERCHEST rules ought to be recommended for rule out of ACS in a general practice setting.
Discussion
Chest pain presents a diagnostic dilemma in general practice. Advances in therapeutic options, the ageing of our populations and associated increase in patients with chest pain, as well as the fear of medico-legal consequences, have led to a dramatic increase in the number of referrals that threaten to overwhelm the emergency services.18 19 CDRs have been coined as an idea to aid in the diagnostic process and to make safe and efficient referral decisions. A prior systematic review on this topic showed that CDRs are not sensitive enough to safely rule out CAD in primary care patients.20 We performed an updated systematic review in which we included both derivation, validation and comparative studies with clinical judgement (‘gestalt’). Moreover, we made a clear distinction between intermittent-type and acute-onset chest pain, as the diagnostic demands for CDR vary between these two clinical presentations. In summary, we found five primary care-based CDRs that have been developed to differentiate cardiac from non-cardiac chest pain. Three CDRs were developed for ruling out CAD in patients with intermittent chest pain, and two CDRs were developed for patients with symptoms suggestive of ACS. Overall, the Marburg Heart Score holds most promise for ruling out CAD in patients with intermittent chest pain with a consistent, high sensitivity and acceptable specificity and an NPV of 97.3%–98.7% in multiple prospective studies. Moreover, the Marburg Heart Score was more accurate in differentiating CAD from non-CAD than the GP’s own clinical judgement, an important argument for implementation into clinical practice. As such, the Marburg Heart score can be used for rule out of CAD in low-risk general practice populations with intermittent-type chest pain (level of evidence of 2). The other CDRs for CAD or ACS lack sufficient validation in external populations or lack sufficient safety or overall accuracy (level of evidence of 3 and 4).
In order for a CDR to be useful in GP settings, it should consist of readily available and/or easy to measure elements. The Marburg Heart Score with its five-item checklist is both user friendly and seems to do an acceptable job in ruling out CAD in (low-risk) patients with intermittent chest pain. Because of its consistent performance, a point-of-care guide issued by the American Family Physician proposes to integrate the Marburg Heart Score into an algorithm for the evaluation of patients with chest pain in primary care.1 It proposes that low-risk patients (score 0 or 1) should not receive further cardiac follow-up, whereas high-risk patients (>3) should be referred for cardiac evaluation. In the intermediate/moderate-risk group (score 2 or 3), the algorithm proposes the use of the ECG and, when negative, to consult with the cardiologist for further work-up or to order a sequential troponin test. When the troponin test is negative, the risk of a cardiac event is deemed <1% within the next 30 days. The guide also states that certain anamnestic elements, including the character of chest pain, should be factored in when making this decision.
While this algorithm may seem appealing, it should be noted that the supportive evidence for the Marburg Heart Score is only applicable for patients with intermittent chest pain in a general practice setting. As such, while risk stratification may be of use to guide referral and diagnostic work-up decisions (ie, exercise testing, etc), there are no data to support the Marburg Heart Score as an ACS rule out tool. This is unfortunate, because it is particularly in the setting of acute-onset chest pain that GPs feel a great need for a CDR. In a recent survey conducted among GPs in the Netherlands, the vast majority of respondents would accept a <1.0% risk for missing a diagnosis of ACS in a patient and would accept no more than 25 (in hindsight) unnecessary referrals.21 The currently available Grijseels (NPV 82.4%, PPV 56.9%) and Bruins Slot (NPV 91.7%, PPV 23.4%) rules fall short of both these targets. The question is whether a CDR based on anamnestic elements will be sufficient to reach a >99% NPV. Perhaps, the additional use of point-of-care tests for cardiac markers may increase the safety of a CDR. Studies in general practice found an NPV for troponin and heart-type fatty acid binding protein of 94%–96% for ACS and 99.0%–99.7% for myocardial infarction, respectively.22–26 As such, current research efforts focus on whether combining these tests (as point-of-care kits) with a CDR could enhance safety and still provide an effective decision aid. This could be particularly helpful for patients with acute onset of chest pain. Similarly for those with intermittent chest pain, the use of the Marburg Heart Score as a primary care-derived clinical risk assessment tool similar to the Diamond-Forrester chest pain rule27 is appealing. However, whether such a strategy is cost-effective compared with usual care should be further evaluated.
Strengths and limitations
We performed a rigorous systematic search and quality assessment of the included articles involving chest pain rules in primary care. We avoided bias in the selection of studies by two reviewers individually identifying eligible studies, with a third to resolve any disagreements. While not being the first systematic review on this topic, this review is to our knowledge the first that examines the results of the CDRs while taking into account the results of the derivation, validation, and compared the performance of the CDR with the unaided clinical judgement of the GP.
Our study also has a number of limitations. First, we accepted a final diagnosis of coronary artery disease based on a delayed-type reference diagnosis based on consensus of a panel of experts using available symptom-related data and work-up. Such a strategy is valid, as mandating the use of coronary angiography as the reference standard would not be feasible in primary care.28 A second limitation is the substantial heterogeneity in the prevalence of ACS among studies of CDRs for acute chest pain (range of 22%–47.8%), which could indicate that GPs may have preselected patients.
Furthermore, we should acknowledge that while we searched for clinical prediction rules for chest pain to rule out CAD or specifically ACS, a minority of patients may present with non-chest pain symptoms (ie, dyspnoea, jaw pain) but do have myocardial ischaemia, these patients (which are more frequently elderly, women and diabetics) may not be properly represented in the included studies.29–31 A third limitation is that not all included studies reported sufficient data to allow construction of two-by-two contingency tables. Therefore, we cannot accurately assess the performance data of these CDRs. Finally, the CDRs were derived over a span of 22 years. Since the criteria for CAD, the prevalence of risk factors and prevalence of CAD may have changed over the years, some CDRs might be outdated.
Chest pain rules outside primary care
Our aim was to research the availability of chest pain rules that are applicable and have been validated in low-resource primary care settings. We, therefore, purposefully restricted the scope of this systematic review and excluded CDRs that rely on advanced laboratory, computer or diagnostic testing for their respective scoring systems. We therefore did not include studies on CDRs that are commonly used in EDs, such as the History, ECG, Age, Risk factors and initial Troponin (HEART),32 Global Registry of Acute Coronary Events33 and Thrombolysis in Myocardial Infarction34 scores as well as the more recent Manchester Acute Coronary Syndromes rule.35 For a comprehensive overview of chest pain rules recently validated in ED patients, we refer to the systematic review by Liu et al.36
Future directions
Chest pain represents a diagnostic challenge for doctors, particularly in the GP setting, due to an unselected patient population, fewer diagnostic options and time restraints. CDRs may be of assistance, as long as they rely on readily available information and directly applicable. The existing CDRs should be more rigorously tested and further optimised, perhaps with the use of machine-learning techniques. Thereafter, we ought to conduct a randomised study in which a CDR-assisted strategy is compared with usual care, in which both safety (clinical outcomes) and efficacy (referral rate) should be assessed. Aside from these research activities, we should also put effort into finding consensus among physicians, patients and other stakeholders in what safety/efficacy balance we are willing to accept when it comes to chest pain. The current trend towards defensive medicine is not sustainable, and as such warrants a discussion on this topic.
Conclusion
Chest pain is a common symptom in primary care, but there is only one validated CDR (Marburg Heart Score) that appears to outperform clinical judgement when applied in patients with intermittent chest pain in a low-risk setting. For ruling out acute coronary syndrome, none of the CDRs was sensitive enough. Future research is warranted for the role of implementing point-of-care cardiac marker tests into CDRs for acute chest pain, as well as the cost-effectiveness of a Marburg Heart Score work-up strategy for intermittent chest pain.
References
Footnotes
Contributors REH and WAML conceived the study and were responsible for the design and search strategy. REH and SCL were responsible for conducting the search. REH, SCL and JCLH conducted the data analysis and produced the tables and graphs. HCPMvW provided input into the data analysis and interpretation. The initial draft of the manuscript was prepared by REH and SCL then circulated among the coauthors for critical revision. All authors helped to evolve analysis plans, interpret data and critically revise successive drafts of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. Funding to cover author processing charges of this publication was provided by the Department of General Practice, Amsterdam UMC, University of Amsterdam, Amsterdam Public Health, Academic Medical Center, Amsterda, The Netherlands.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional data available.
Patient consent for publication Not required.