Article Text

Abstract
Introduction Approximately 1.4%–2.2% of the global population suffers from chronic migraine. Acupuncture may serve as an alternative management for chronic migraine, where pharmacological prophylaxis is not suitable. However, the effects of acupuncture as migraine prophylaxis have not been confirmed. This study is designed as a single-blinded, double-dummy randomised controlled trial to evaluate the efficacy and safety of acupuncture compared with topiramate in patients with chronic migraine.
Methods and analysis A total of 60 participants will be randomly assigned to two different groups. Participants will receive verum acupuncture and placebo medicine in the treatment group, while participants in the control group will be treated with sham acupuncture and real medicine (topiramate). All participants will receive a 12-week treatment and then be followed up for another 12 weeks. The primary outcome is the reduction of monthly headache days, and the secondary outcomes include the reduction of the number of days with acute headache medications, and changes of Migraine Disability Assessment, Migraine-Specific Quality of Life Questionnaire, Headache Impact Test, State-Trait Anxiety Inventory-trait, and Beck Depression Inventory-II scores from baseline to endpoints.
Ethics and dissemination Ethical approval of this study was granted by the Research Ethical Committee of Beijing Hospital of Traditional Chinese Medicine Affiliated to Capital Medical University (2017BL-045-01). Written informed consent will be obtained from all participants. Outcomes of the trial will be disseminated through peer-reviewed publications.
Trial registration number ISRCTN13563102; Pre-results.
- protocol
- acupuncture
- chronic migraine
- randomised controlled trial
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study adopts needling ineffective acupuncture points as a sham acupuncture intervention to minimise performance bias.
This study uses a double-dummy design in order to blind all patients, rule out the placebo effect and make treatments of both groups possibly effective to ensure a better compliance of participants.
This study will use topiramate as the standard drug therapy in the control group, which is a widely accepted treatment for chronic migraine prevention; this study will use eight main and two additional acupuncture points in the treatment group based on the concept of a combination of standardised and individualised acupuncture treatment.
This study uses comprehensive outcome measures, including number of monthly headache days, acute headache medications, migraine-related disability, quality of life measures and psychological distress.
One potential limitation is that the placebo effects on patients produced by placebo drug and sham acupuncture may be different due to their different non-specific effects.
Introduction
Migraine is a highly prevalent neurological disorder considered to be the second largest contributor to worldwide disability.1 Migraine is considered to be a self-limited episodic pain disorder, with a growing acknowledgement that chronic migraine is in fact the end-stage consequence of uncontrolled or poorly controlled episodic migraine.2 3 According to the International Classification of Headache Disorders-Third Edition (beta version) (ICHD-IIIβ) from the International Headache Society, chronic migraine is defined as ‘headache lasting more than four hours each day for more than 15 days per month and for at least three months, with at least eight days of headache meeting diagnostic criteria for episodic migraine’.4 Primary chronic migraine is rare; previous research has suggested that chronic migraine usually evolves from episodic migraine that gradually increases in attack frequency, with an annual progression rate of approximately 3%.5 6 The prevalence of chronic migraine is usually reported to be 1%–2% in the general population,7–9 and approximately 8% among individuals with migraine.7 Compared with episodic migraine, chronic migraine is characterised by a stronger symptom intensity with longer duration and may cause more severe disability. Chronic migraine is also associated with a significantly greater degree of healthcare burden and psychiatric comorbidity, such as depression and anxiety.10–12
The conversion from episodic to chronic migraine is related to the overuse of acute migraine medication,3 13 ineffective treatment of acute migraine,14 obesity,15 depression16 and stressful life events, such as divorce or being recently widowed.5 Among them, the overuse of acute migraine medication is considered to be the most important risk factor. The underlying physiological mechanisms of the transformation into chronic migraine have not been fully discovered, although the roles of atypical pain processing, central sensitisation, cortical hyperexcitability and neurogenic inflammation have been studied. Furthermore, central sensitisation is assumed to be one of the key mechanisms of migraine chronification. Recurrent migraine attacks are considered to lead to sensitisation processes of the trigeminal system, which results in an increased susceptibility to migraine-triggering factors, a reduced threshold for activation of this system and transformation to chronic migraine.17
Once chronic migraine is established, to identify an effective treatment is challenging. The options available for the treatment of chronic migraine include standard pharmacological treatment with migraine prophylactic drugs, injections with botulinum neurotoxin A, as well as invasive and non-invasive neuromodulation and neurostimulation therapies.18 Notably, once a migraine attack has begun, pain killers or specific headache medication should be avoided to be used as the sole treatment since they will not relieve symptoms, and medication- overuse headache may develop due to continuous intake of these medications. Instead, the treatment for chronic migraine should aim for effective prevention of migraine attacks. In this regard, the current standard preventive treatments include topiramate, beta-blockers and valproate. Topiramate has been evaluated by multiple double-blinded randomised controlled trials (RCT) as a preventive medication for migraine attacks.
The use of topiramate can effectively reduce headache days,19 improve patients’ quality of life,20 prevent the progression from episodic to chronic migraine21 and induce remission from chronic to episodic migraine.22 Adverse events (AE) which include paraesthesia, cognitive problems, dyspepsia, fatigue, dizziness, somnolence and nausea have been reported during the titration and maintenance period of using topiramate.23 In addition, some patients with chronic migraine do not respond to preventive medications,17 hence other alternative non-pharmacological therapies are still in need.
Acupuncture has been used for over 2500 years in China as an effective non-pharmacologic management for headache, including migraine,24–32 but clinical evidence on its efficacy in chronic migraine prevention is limited. Upon review of the evidence for the efficacy of acupuncture in chronic migraine, only one published RCT was found, which concluded that acupuncture was more effective than topiramate in reducing the number of monthly moderate/severe headache days.33 However, this study was designed as an open-label clinical trial in which neither the researchers nor the participants were blinded. The effectiveness shown by this study may have been influenced by the lack of blinding. Therefore, we designed an RCT involving a placebo control to ensure participants’ blinding to investigate the efficacy and safety of acupuncture treatment as prophylaxis for chronic migraine.
Methods and analysis
Study design
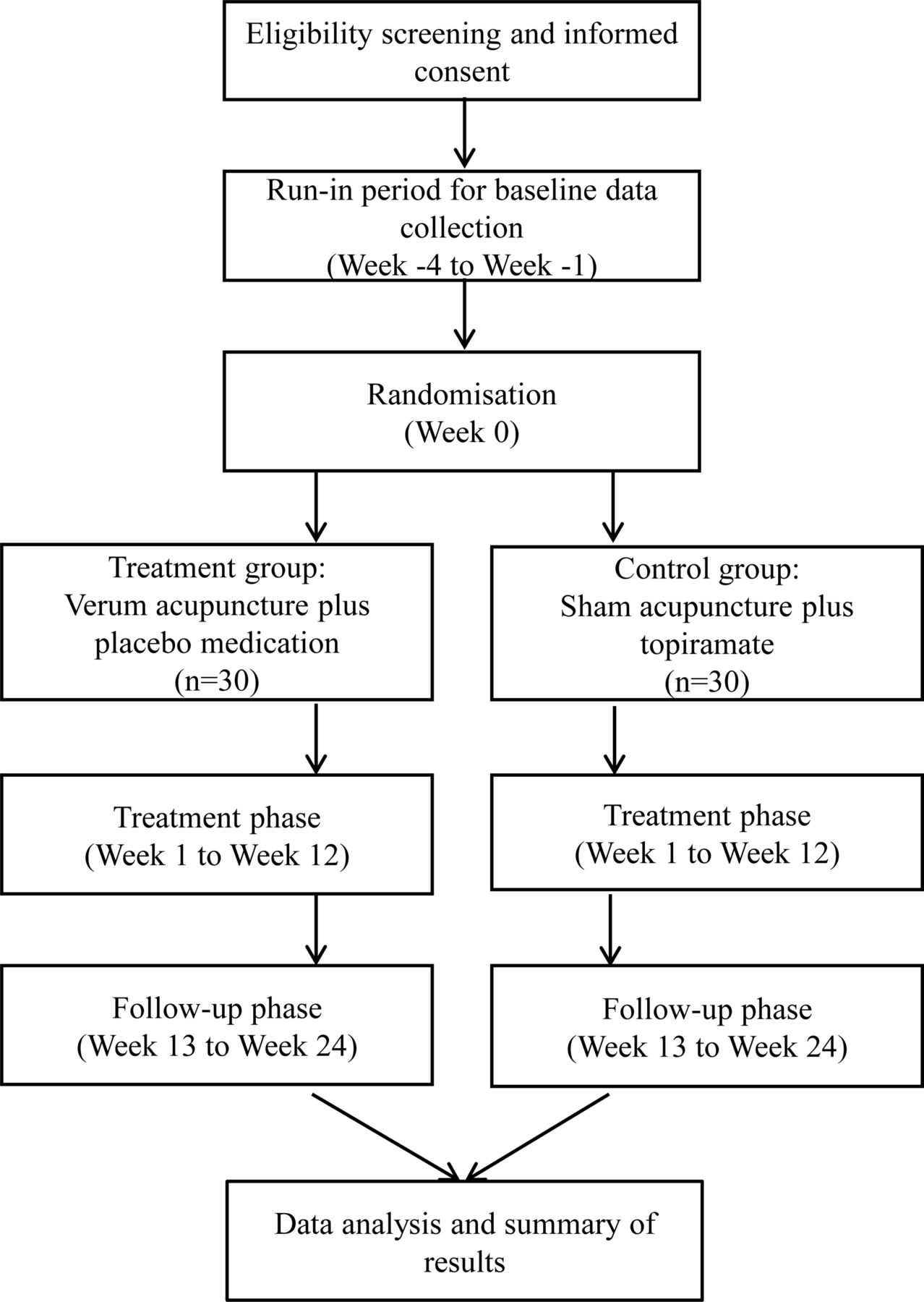
This trial is designed as a single-blinded, double-dummy RCT to evaluate the efficacy of acupuncture compared with topiramate in patients with chronic migraine. Sixty participants with chronic migraine will be randomly assigned to the treatment group and control group at a 1:1 ratio. The schedule of enrolment, interventions and assessments is summarised in table 1 (online supplementary file 1), and the flow diagram of the study procedure is presented in figure 1. Patients’ recruiting is from December 2017.
Supplementary file 1

Flow diagram of the study procedure.
Schedule of enrolment, interventions and assessments
Recruitment
Trial participants with chronic migraine are being recruited by clinicians from outpatient clinics at the Beijing Hospital of Traditional Chinese Medicine Affiliated to Capital Medical University. Meanwhile, information flyers introducing the details of the trial are being posted at the outpatient clinics for greater exposure.
Study procedure
This study consists of three phases including: (1) a 4-week screening phase (week −4 to week 0); (2) a 12-week treatment phase (week 1 to week 12); and (3) a 12-week follow-up phase (week 12 to week 24).
Once potential participants show interest in this trial, they will be requested to continually record their headache symptoms using a headache diary for 4 weeks, as well as their medical history in a screening form. Then they will be invited to attend an eligibility assessment in which their eligibility will be assessed by trial investigators; thereafter, eligible participants will be enrolled and randomly assigned to either the treatment group or the control group and given a 12-week treatment. During the treatment phase, medication dosages will be titrated for 4 weeks, and then followed by a maintenance dosage for 8 weeks.
Participants
Inclusion criteria
Participants who meet all of the following requirements will be considered for inclusion: (1) diagnosed as having chronic migraine according to the diagnostic criteria specified by the ICHD-IIIβ4; (2) aged between 18 and 65 years old; (3) received no prophylactic treatments using acupuncture or pharmacological medicine in the past 3 months; and (4) provided written informed consent.
Exclusion criteria
Patients will be excluded if they have (1) tension-type headache, cluster headache or other primary headaches; (2) relatively severe systemic diseases (cardiovascular disease, acute infectious disease, haematopathy, endocrinopathy, allergy or methysis); (3) headache caused by otorhinolaryngology diseases or intracranial pathological changes; (4) secondary headache or other neurological diseases; or (5) pregnancy, lactation or insufficient contraception.
Randomisation and allocation concealment
The randomisation will be performed by the Research Centre of Clinical Epidemiology, Peking University Third Hospital. A block randomisation method (with a block size of four) will be used to generate the random allocation sequence; predetermined computer-generalised randomisation opaque sealed envelopes will be used to ensure the allocation concealment. The opaque sealed envelopes, with the participant’s screening order printed outside and randomly assigned group printed inside, will be numbered consecutively and connected into a strain. Researchers will enrol the eligible participants after screening, then separate and open each envelope from the strain in the sequence corresponding to the participant’s screening order, and assign the eligible participant into either the treatment group or control group.
Blinding and informed consent
In this study, the participants will be informed that they will have a 50% chance of being allocated to receive either of the two treatments: verum acupuncture plus placebo medication in the treatment group, or sham acupuncture plus real medication (topiramate) in the control group. The placebo medication will be identical to the real medication (topiramate) and sham acupuncture will produce the same stimulation as the verum acupuncture. Hence, participants will be blinded to their group allocation. The credibility of blinding will be tested at the beginning and end of the treatment phase (week 1 and week 12). Furthermore, outcome assessors and personnel involved in data collection and data analysis will be blinded to participants’ group allocation throughout the entire trial. The acupuncturist cannot be blinded due to the nature of the intervention, but they will be trained not to communicate with participants or outcome assessors regarding treatment procedures and responses.
Intervention
The acupuncture treatment protocol was determined according to records in ancient and modern books and results of previous research on acupuncture treatment for chronic migraine.26 All participants will go through a standardised interview and be provided with details of the study. The acupuncturists who deliver treatments for both groups are registered with the Ministry of Health of the People’s Republic of China as Chinese medicine practitioners, and have more than 20 years of clinical experience. Before the trial begins, all acupuncturists will receive special training regarding the purpose and standard procedure of the trial, treatment strategies and quality control. The treatment details will be fully documented in accordance with the Standard Protocol Items for Randomized Trials Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA)34 and good clinical practice guidelines.
All participants will receive treatment for 12 weeks. In the treatment group, participants will receive three acupuncture sessions each week, together with placebo medication. In the control group, participants will be given medicine (topiramate) and three sessions of sham acupuncture each week.
Each acupuncture session (both verum and sham acupuncture) will last for 30 min. Sterilised, single-use needles (Hwato Needles, made in Suzhou, China) will be used for acupuncture in this trial. The number of needles will be no more than 10 in each session for both groups. Thirty-gauge (0.3 mm in diameter) needles with 40 mm in length will be used for limb points and 32-gauge (0.25 mm in diameter) needles with 25 mm in length will be used for head points. All needles will be inserted 10–15 mm in depth and manually manipulated with rotation methods to produce a characteristic sensation known as De Qi (feeling of needle sensation that refers to the tenseness around the needle felt by the practitioner and numbness, distension, soreness and heaviness around the point felt by the participant).
The placebo medication will be made by Xi’an Janssen Pharmaceutical and will have the exact same appearance as the real medicine (topiramate). During the titration period, participants will receive topiramate 25 mg/day at bedtime for 1 week, followed by a weekly increase of 25 mg up to either 100 mg/day of topiramate or to the maximal tolerated dose. Starting in week 2, topiramate will be given daily in equally divided twice daily doses. During the maintenance period, a stable topiramate dose of at least 50 mg/day will be required. All participants will be permitted to treat acute headaches as required; ibuprofen will be recommended to all participants as their first choice for acute medication. The name and dosage of these medications will be recorded in the headache diaries.
The points used in the treatment group
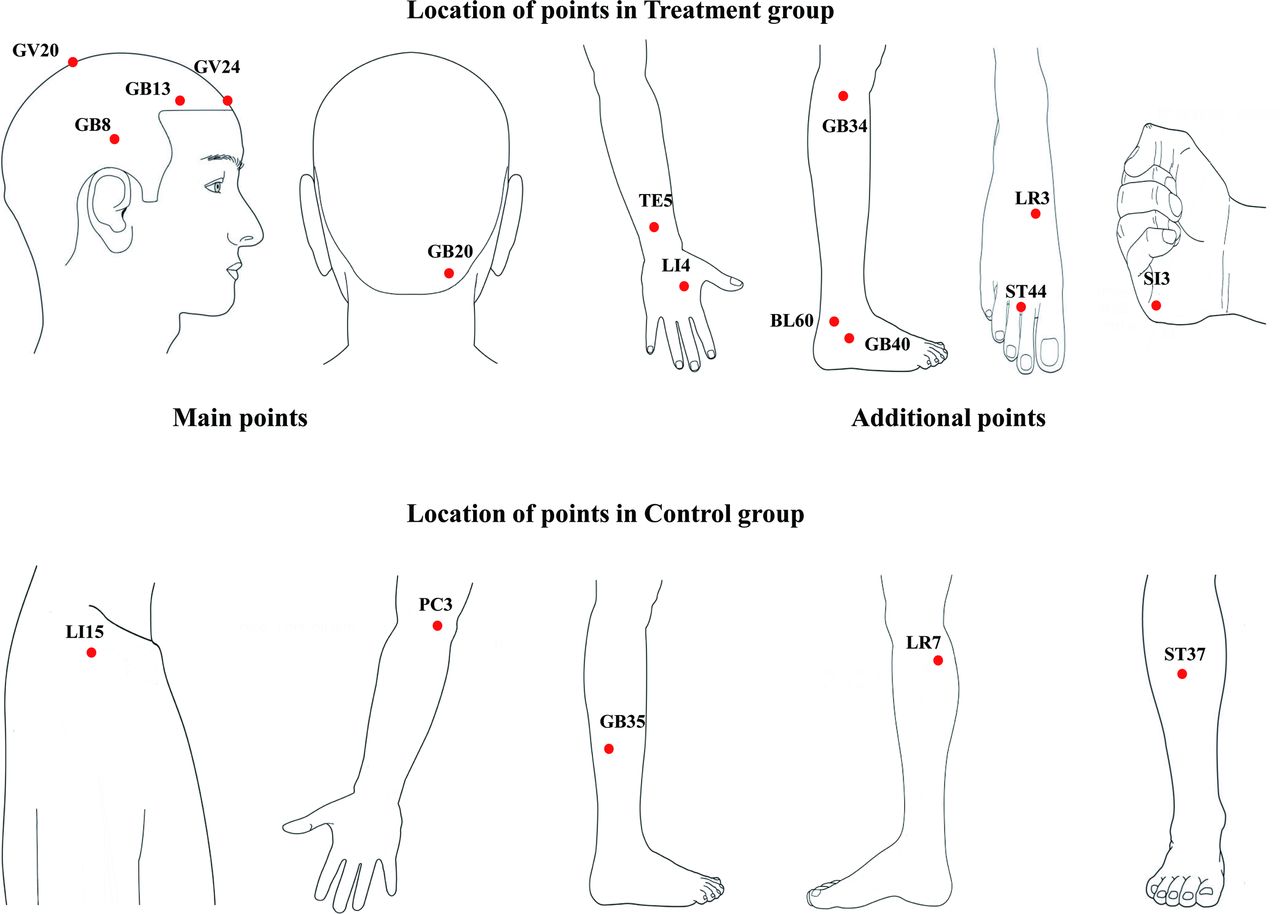
The main points used for all participants in the treatment group are: GV20 (Baihui), GV24 (Shenting), bilateral GB13 (Benshen), bilateral GB8 (Shuaigu) and bilateral GB20 (Fengchi).
Additional two points may be chosen according to syndrome differentiation of meridians: Shaoyang headache (TE-GB): TE5 (Waiguan) and GB34 (Yanglingquan); Yangming headache (LI-ST): LI4 (Hegu) and ST44 (Neiting); Taiyang headache (SI-BL): BL60 (Kunlun) and SI3 (Houxi); Jueyin headache (PC-LR): LR3 (Taichong) and GB40 (Qiuxu) (see figure 2).
{kind=link}
{kind=link}
Schematic sites of acupuncture points in treatment group and control group.
The points used in the control group
The sham acupuncture will be conducted using the same methods as verum acupuncture but on different points, including two points on the arms and three points on the legs. These points were defined as unrelated to headache based on a vast amount of Chinese medicine reference books and the consensus of clinical experiences of acupuncture experts. The sham points are bilateral LI15 (Jianyu), bilateral PC3 (Quze), bilateral GB35 (Yangjiao), bilateral LR7 (Xiguan) and bilateral ST37 (Shangjuxu) (see figure 2).
Outcome measures
The primary outcome measure will be the reduction of monthly headache days, which will be calculated using the data collected from the second to the fourth headache diaries (treatment phase) compared with the first diary (collected in the screening period, 4 weeks before the beginning of the trial). Headache diaries are designed to record the details of migraine attacks, including duration, frequency, location, intensity, presence of aura, causality of the headache and concomitant symptoms in each migraine attack. The participants will also document the number of days with acute headache medication intake (including name, dosage, time of taking medicine, time of pain relief and side effects of analgesic drugs) for each migraine attack and study medication received in the headache diaries.
The secondary outcome measures include (1) reduction of the number of days with acute headache medications, from the second to the fourth diaries compared with that from the first diary (screening period); (2) change of Migraine Disability Assessment (MIDAS)35 scores from baseline to endpoints (week 12 and week 24); (3) change of Migraine-Specific Quality of Life Questionnaire (MSQ)36 scores from baseline to endpoints; (4) change of Headache Impact Test (HIT-6)37 scores from baseline to endpoints; (5) change of State-Trait Anxiety Inventory-trait (STAI-T)38 scores from baseline to endpoints; and (6) change of Beck Depression Inventory-II (BDI-II)39 scores from baseline to endpoints.
These five questionnaires will be repeatedly assessed at week 0, week 12 and week 24 by one physician who is blinded to group allocation to ensure consistency.
Detailed time points of each outcome assessment are provided in table 1.
Safety assessments
Safety assessments will include the incidence of AEs, clinical laboratory tests (including urine pregnancy test), vital sign measurements and physical examination findings. The clinical laboratory tests will include haematology, chemistry and urinalysis tests. Vital sign measurements will include sitting blood pressure, heart and respiration rate, and body temperature. AEs are defined as negative or unintended clinical manifestations following the treatment. Our investigators will collect information regarding AEs throughout the treatment and follow-up phases. Participants will be instructed to report any abnormal reactions or uncomfortable feelings experienced to any researcher. All unexpected AEs will be recorded with details in the Case Report Forms (CRF), including time of occurrence, degree of AE and possible causes. Participants with mild and moderate AEs will be treated for their symptoms and closely monitored as necessary by the researcher. Severe AEs will be reported to the Research Ethics Committee, which will provide medical advice to the research team within 48 hours, and the Research Ethics Committee will determine whether a termination of the trial is required.
Data management
All researchers including the acupuncturists, outcome assessors, data collector, data manager, data entry personnel and statistician will receive special training regarding the standard procedure and data management. During the recruitment period, our data collector will record the baseline characteristics of participants in CRFs, and all data will be checked by the data manager.
Upon the completion of the treatment and follow-up phases, all participants’ data will be completed and recorded on the original CRFs and then entered into Excel spreadsheets by two data entry personnel independently, following which the data manager will cross-check two data sets to ensure accuracy. If any inconsistencies are noted, corrections will be made according to, and marked on, the original CRFs. All data will be managed in accordance with the Data Protection Act of 1998.40 All hard copy documents related to the research will be saved in a locked filing cabinet, while electronic documents will be stored in a special computer that will remain password protected and accessible only to the principal investigators. All research documents, including both the hard copy documents and electronic files, will be saved for at least 5 years after publication. If readers have any questions regarding our published data, they will be permitted to contact our first author or corresponding author to obtain the original data.
Sample size calculation
In a previous study,33 the reduced number of chronic migraine days after treatment was 10.5±2.8 days in the acupuncture group and 7.8±3.6 days in the control group. PASS V.11 software (NCSS, Kaysville, Utah, USA) was used to calculate that, based on 80% power to detect a significant difference (α=0.05, two sided), 26 participants will be required for each group. Allowing for a 10% withdrawal rate, we plan to include a total of 60 participants with 30 participants in each group.
Statistical analysis
Data analysis will be performed by statisticians who are blinded to the entire allocation and intervention process. The statisticians are affiliated with the Research Centre of Clinical Epidemiology, Peking University Third Hospital, which is one of the most authoritative statistics centres in the country. All data in this trial will be assessed using the SPSS statistical software package (V.22.0) (International Business Machines). The intention-to-treat population will be the main set used for all efficacy analyses. The per-protocol set will be used for the sensitivity and consistency analysis to compare the results from the intention-to-treat set. The per-protocol set will consist of the participants who have completed the trial without major protocol violations and will finally provide all outcome measures. The last observation carried forward method will be used to process the missing data for the primary outcome. Two-tailed analyses will be conducted, with the level of statistical significance defined as p<0.05.
Demographic characteristics and baseline measurements of the variables of each group will be summarised. Continuous variables will be shown as the means±SDs with a 95% CI. Independent two-sample t-tests or the Mann-Whitney U test will be performed to compare the continuous data from each group. For dichotomous or categorical data, frequency and percentage will be presented, and the difference between groups will be compared using the Χ2 test or the Fisher’s exact test.
The mean change of the monthly headache days is the primary outcome measure of this study. One sample of the Kolmogorov-Smirnov test will be used to test the normal distribution of continuous variables. Continuous variables will be shown as the means±SDs if they are normally distributed or as medians with IQRs if they are not normally distributed. If the measurement data are normally distributed, independent two-sample t-tests will be used for comparisons among the groups, while paired t-tests will be used for within-group comparisons. If the measurement data have a non-normal distribution, the Mann-Whitney U test will be used for comparisons among the groups, while Wilcoxon signed-ranks test will be used for within-group comparisons.
The secondary outcome measures include the mean change of days with acute headache medications, and the changes of MIDAS, MSQ, HIT-6, STAI-T and BDI-II scores from baseline to endpoints in the study. The secondary outcome measures will be analysed following the same methods used for the primary outcome measure analysis.
AEs will be analysed in the safety set, which consists of all participants who received at least one treatment in this trial. AEs will be pooled for each organ system class and preferred term, and then the percentage of patients with AEs and percentage of patients with laboratory AEs will be summarised with descriptive statistics.
Patient and public involvement
This trial was designed to evaluate the add-on effects of acupuncture for migraine prevention. In clinical practice, the prevention of episodic migraine is considered more important than the treatment for acute attacks for patients with chronic migraine. Adding acupuncture to conventional therapy may increase the effectiveness in terms of preventing episodic migraine, hence significantly improve patients’ quality of life. The outcome measures used in this study were commonly used in clinical trials of chronic migraine, and considered as important endpoints in our clinical practice. Patients with chronic migraine in our clinical department were consulted prior to the trial design, in particular, the treatment frequency and duration of this trial were summarised from our clinical experience and patients’ feedback. The participants of this trial will be recruited from our clinical department. However, those who were involved in the consultation related to the trial design will not be included as trial participants. Upon the completion of this trial, a journal article manuscript will be prepared to present the trial results. Once this manuscript is published, a brief summary of results using plain language will be sent to all trial participants. The burden of intervention will not be assessed by trial participants.
Ethics and dissemination
The trial protocol is in accordance with the principles of the Declaration of Helsinki41 and was approved by the Research Ethical Committee of Beijing Hospital of Traditional Chinese Medicine Affiliated to Capital Medical University on 21 July 2017 (Ethics Reference No: 2017BL-045-01) (online supplementary file 2). This trial was registered at ISRCTN (ID: ISRCTN13563102). Each participant will be provided information regarding the study protocol. Written informed consent will be obtained from every participant.
Supplementary file 2
Discussion
This trial is designed as a single-blinded, double-dummy RCT. The completion of this trial will provide detailed and accurate evidence of the efficacy and safety of acupuncture for chronic migraine prophylaxis. The advantages of the trial design are shown in the following three aspects.
Double-dummy design and blinding
To determine an appropriate control method is crucial for the assurance of the methodological quality of an RCT. Considering that acupuncture is a physical intervention, to design an inert placebo control for acupuncture is challenging. Although using placebo needles on effective acupuncture points has been applied in previous clinical trials, it was found that this approach may induce a wide range of peripheral, segmental and central physiological responses to an unpredictable degree.42–44
The method of needling non-acupuncture points with minimal acupuncture (using fine needles to penetrate the skin superficially) has been employed as a sham control in previous studies of migraine.29 45 However, some researchers have advised that involving sham acupuncture as the control tends to have more ‘negative’ results compared with the design of verum acupuncture versus other types of control, such as placebo acupuncture (non-insertion) and non-acupuncture treatment.46 47 In addition, sham acupuncture produced a larger effect size than the pharmacological placebo compared with non-treatment.48 49 It has been suggested that sham acupuncture appears to comprise a true placebo effect and other physiological effects from needle insertion.50 Therefore, RCTs utilising sham acupuncture as a control can only answer the question of acupuncture point specificities or stimulation technique specificities, but not efficacy.51 52
Further, the methods of using non-penetrating placebo needles or superficial needling may not be practical among the Chinese population, considering that Chinese people generally expect that certain sensations should be achieved in acupuncture treatment. Therefore, we chose the method of needling ineffective acupuncture points as the sham acupuncture intervention. This method has been used in previous clinical trials of migraine with the advantage of minimising bias caused by unblinding of patients.28 53
Based on careful consideration of control methods’ selection, we determined a double-dummy type design in this study. Both groups in this trial will receive real treatments (either real acupuncture or real medication). This approach will encourage a better compliance of participants. A medication proven effective for chronic migraine and sham acupuncture (ineffective acupuncture points) were chosen as the treatments given to the control group in our study. Compared with the design in which a positive drug is given without sham acupuncture as a control, our design may rule out the possibility of a placebo effect caused by the strong belief in acupuncture among Chinese population.
Genuine double-blinding is difficult in acupuncture trials since the acupuncturists must be aware of the participant’s group allocation to deliver the treatment. Although some efforts have been made to design a double-blinding placebo acupuncture device, there has not been enough evidence to support the use of such a device.54
In this trial, all participants will be blinded through the double-dummy design, and all outcome assessors and statisticians will be kept unaware of group allocation throughout the whole process. Only the acupuncturists will not be blinded but they will be required to minimise conversation about the treatment details.
Selection of medication and acupuncture points
Topiramate, as an antiepileptic medication (AED), is Food and Drug Administration approved and widely accepted as a treatment for chronic migraine prevention. Several placebo-controlled randomised clinical trials have shown that topiramate significantly reduced the number of migraine headache days in patients with chronic migraine.19 55 56 Topiramate is considered safe, effective and generally well tolerated for the prophylactic treatment of chronic migraine. Therefore, we will compare the efficacy of acupuncture with topiramate, which was chosen as the standard drug therapy. Migraineurs are more sensitive to topiramate-related AEs than patients with epilepsy. The most common AEs associated with topiramate are paraesthesia and cognitive problems. Paraesthesia commonly occurs in early topiramate treatment but is rarely a cause for treatment discontinuation. Cognitive syndromes occur much less frequently than paraesthesia but are more troublesome and may cause termination treatment. AEs of topiramate are generally of mild or moderate severity and tend to be dose dependent.57
Thus far, the particular mechanism by which acupuncture affects migraine has not been fully revealed. According to the gate control theory, once fine acupuncture needles have been inserted into body points, A delta fibres may be stimulated to close the pain gates in the central nervous system, therefore the sensation of pain will not be perceived due to failure of reaching the thalamus.58 In addition, many researchers have held the view that acupuncture may influence calcium signalling and the opioid system. The acupuncture stimulations may produce and release endogenous opioids, which bind to opiate receptors in the brain and mediate analgesia through the descending pain inhibitory system.59
Furthermore, the positive effect of acupuncture on migraine may not be owing to penetration of the tissues per se, but also due to the local stimulations on effective acupuncture points (perforation or touch).60 According to traditional Chinese medicine theory, an acupuncture point refers to a specific point on the body surface that is inactive when the body is in a healthy condition, but can be further activated by certain stimuli. Well-defined acupuncture point selection principles for practitioners to consider in clinical situations have been developed and used under the umbrella of the existence of acupoint specificity.61
Traditional acupuncture has its own diagnostic system for headaches, in which treatment should be individualised (acupuncture points vary from person to person or from treatment to treatment). However, the absence of standardised approaches to acupuncture treatments obstructs data reproducibility across the discipline. With this in mind, we will use fixed and classic acupuncture points (standardised acupuncture with eight main points) in patients in the treatment group during every therapeutic session. A standardised acupuncture treatment protocol was obtained by the consensus of our acupuncture expert panel. This standardisation makes our study replicable, consistent and as scientifically rigorous as possible. In addition, all patients will be classified into four subtype syndromes according to syndrome differentiation of meridians,62 and two additional points will be chosen according to the syndrome type to fulfil the need for individualised treatment.
Comprehensive outcome measures
The monthly paper-and-pencil prospective headache diary includes (1) the use of any headache abortive medication; (2) headache occurrence; (3) headache intensity rated as average pain intensity for that day using a 0 to 10-point scale; (4) headache duration; and (5) associated symptoms for migraine. The number of monthly headache days will be the primary outcome measure in our study and has often been used as the primary outcome in previous studies of the chronic migraine population.33 63–65
With respect to secondary outcomes, we will measure acute headache medications, migraine-related disability, quality of life measures and psychological distress. The MIDAS scale is an ordinary rating scale to assess the migraine-related disability of a patient.35 Previous studies66 67 have illustrated that the MIDAS questionnaire is a valid, effective and sensitive tool to assess the migraine disability in a patient with chronic migraine. The HIT-6 will be used to assess headache impact,37 68 which is a validated 6-item questionnaire covering content categories in pain, role functioning, social functioning, vitality, cognitive functioning and psychological distress. This questionnaire has been proven reliable and valid for use in the chronic migraine population.69 70 Quality of life in those with chronic migraine will be assessed using the MSQ, a 14-item questionnaire designed to measure how migraines affect or limit patients’ daily performance over the preceding 4 weeks across three domains36 71: role restrictive (RR), role preventive (RP) and emotional functioning (EF). Specifically, the RR domain assesses how migraines limit a sufferer’s daily social and work-related activities, the RP domain measures how migraines prevent such activities and the EF domain gauges the emotions associated with migraine. In addition, the chronic migraine population is often associated with significant psychological distress.72 Therefore, we will also apply the STAI-T39 73 and BDI-II38 to assess participants’ likely depression and distress symptoms.
It should be noted that our study has certain methodological limitation. To blind the patients, we will use a double-dummy design of verum acupuncture and placebo drug compared with topiramate and sham acupuncture. However, different types of placebos may have different non-specific effects. Higher placebo response rates are consistently reported with physical intervention such as acupuncture than those seen in trials using oral drugs.74 75 Therefore, the placebo effects on patients produced by the placebo drug and sham acupuncture may differ, which could potentially affect the therapeutic outcomes.
Acknowledgments
The authors are grateful to Yanhua Zhou and Yaoyuan Tang, patient representatives, for providing their experience as patients with chronic migraine to the design and detail of this study and to other members of the patient advisers group.
References
Footnotes
LL and L-Z contributed equally.
Contributors BL, XGJ, LL and LPZ conducted the study. LL and LPZ drafted the protocol. CSZ, KLW and JXZ participated in the design of the study and contributed to the revising the protocol manuscript. LZ was responsible for the statistical design of the study. LPW provided clinical advice and made critical revisions. BL is a principal investigator of the study and is responsible for making final decisions on the trial design and manuscript preparation. All authors approved the final manuscript.
Funding This study was supported by Beijing Municipal Science and Technology Commission (grant number Z171100001017033), China National Natural Science Foundation (grant number 81603683) , China Postdoctoral Science Foundation Funded Project (grant number 2018M630261) and National Basic Research Program of China (grant number 2014CB543203).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical approval was granted on 21 July 2017 by the Research Ethical Committee of Beijing Hospital of Traditional Chinese Medicine Affiliated to Capital Medical University (Ethics Reference No: 2017BL-045-01).
Provenance and peer review Not commissioned; externally peer reviewed.