Article Text

Abstract
Objectives The aim of this research is to investigate if two additional interventions, test and reflection, after standard cardiopulmonary resuscitation (CPR) training facilitate learning by comparing 13-year-old students’ practical skills and willingness to act.
Settings Seventh grade students in council schools of two municipalities in south-east Sweden.
Design School classes were randomised to CPR training only (O), CPR training with a practical test including feedback (T) or CPR training with reflection and a practical test including feedback (RT). Measures of practical skills and willingness to act in a potential life-threatening situation were studied directly after training and at 6 months using a digital reporting system and a survey. A modified Cardiff test was used to register the practical skills, where scores in each of 12 items resulted in a total score of 12–48 points. The study was conducted in accordance with current European Resuscitation Council guidelines during December 2013 to October 2014.
Participants 29 classes for a total of 587 seventh grade students were included in the study.
Primary and secondary outcome measures The total score of the modified Cardiff test at 6 months was the primary outcome. Secondary outcomes were the total score directly after training, the 12 individual items of the modified Cardiff test and willingness to act.
Results At 6 months, the T and O groups scored 32 (3.9) and 30 (4.0) points, respectively (p<0.001), while the RT group scored 32 (4.2) points (not significant when compared with T). There were no significant differences in willingness to act between the groups after 6 months.
Conclusions A practical test including feedback directly after training improved the students’ acquisition of practical CPR skills. Reflection did not increase further CPR skills. At 6-month follow-up, no intervention effect was found regarding willingness to make a life-saving effort.
- cpr training
- skill test
- reflection
- willingness
- feedback
- students
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The best method to teach cardiopulmonary resuscitation (CPR) in school is unknown, therefore we evaluate key concepts in educational science in a cluster randomised trial.
To study the retention of knowledge and skills after CPR training, assessments were made both directly after intervention and at long-term follow-up.
The study included students from all socioeconomic areas of two major municipalities in south-east Sweden.
The set-up of the trial did not allow us to explain the cause of differences observed between the intervention groups.
Introduction
Sudden unexpected cardiac arrest is one of the most common causes of death in Europe.1 Early identification of the cardiac arrest, call to emergency medical service and prompt initiation of bystander cardiopulmonary resuscitation (CPR) are the cornerstones of resuscitation and crucial for survival in out-of-hospital cardiac arrest (OHCA).2 Early initiation of CPR at least doubles the survival rate in OHCA.3 4 Practical CPR training in school, mandatory to all students, would have the potential to significantly increase basic CPR skills on a populational level. Such a situation could potentially increase the lay resuscitation rate.2 5–8
Education in CPR can be delivered in different formats. There is a knowledge gap regarding what is the optimal method of CPR training to acquire CPR skills.2 Participants’ CPR skills after training are limited and decrease within months after training.2 9 10
Learning is a complex process, influenced by several factors.11 12 Key concepts in educational science are, for example, test, feedback and reflection. Studies show that tests in various formats can increase learning outcomes.13–15 Feedback has a powerful influence on performance.16 According to the Swedish school curriculum, students are expected to reflect on different situations and events and on their learning.11 A core content in CPR training for lay people is practical training; reflection and discussion with the other participants are limited.
The aim of this study was to investigate if two additional interventions, test and reflection, after standard CPR training facilitate learning by comparing 13-year-old students’ practical skills and willingness to act. We hypothesised that both the test and the reflection would provide an additional learning session and contribute to improved knowledge.12 13
Methods
Study population and design
All council schools with seventh grade students (13 years of age) in two Swedish municipalities (Linköping and Norrköping) were invited to participate in the study. In the framework of this study, the intervention methods were applied in 13 schools. Six schools chose for different reasons not to take part in the study.
Seventh grade students in participating schools were eligible for inclusion. Written study information was sent to the students and their guardians. Oral informed consent was obtained from all study participants. Students were excluded if they declined participation or had a physical handicap that limited their physical performance.
A cluster randomised design was applied,17 where each school class was allocated to one of three groups using a randomisation list. The interventions of the groups were based on core concepts in pedagogy: test, feedback and reflection. To evaluate the effect of test including feedback and reflection, the groups were as follows:
CPR training only (O)
CPR training with a practical skill test including feedback (T)
CPR training with reflection and a practical skill test including feedback (RT).
It was important that the design of the interventions facilitated implementation; the education could fit into one lesson, be given in whole-class and be provided by teachers at the school (less costly, facilitates scheduling).6 9 18 19 Outcomes were assessed directly after training and at 6 months. The study was conducted from December 2013 to October 2014.
Standard CPR training applied in all groups
All intervention groups (O, T and RT) received standardised practical CPR training and the participants used an individual training manikin, MiniAnne (manufactured by Laerdal, Stavanger,Norway), during training. The training sessions were conducted in accordance with current European Resuscitation Council guidelines.20 Training was performed in a whole-class set-up with 14–29 students in each class. Teachers at the schools, who all were CPR instructors, were responsible for the CPR training.6 9 18 They received oral and written information to be updated on the present interventions. CPR training was carried out during a 45–60 min lesson. The training was either mobile application or digital video disc based,21 evenly distributed in the intervention groups (table 1). The teachers served as facilitators of the CPR training sessions as previously described.21 After the standardised practical CPR training, the additional interventions, test and reflection, were performed.
Characteristics of the students
Additional intervention with a practical test including feedback
To compare learning outcomes, the students in groups T and RT performed a practical test for 3 min directly after the CPR training. Tests can increase learning outcomes, therefore we chose to investigate if the test contributed to the learning session.13–15 The test was performed individually as previously described.21 In brief, the student was introduced to an OHCA scenario and asked to perform the correct actions. Optimal performance included 30 s to check for responsiveness, respiration and call for help, followed by 2.5 min of CPR. The CPR should include at least five cycles, each consisting of 30 compressions and two ventilations.
The Laerdal PC skill reporting system V.2.4, connected to manikin ResusciAnne, measured the quantitative data, whereas direct observation by the investigator was used to evaluate how well the student checked for responsiveness and respiration and called for help.21 All data were recorded directly into a modified version of the Cardiff test,22 where a score in each of 12 items resulted in a total score of 12–48 points (see online supplementary file 1).
After the test, the investigator gave individual feedback for 2 min. The feedback was partly based on Hattie and Timperley's model, which addresses the following questions: ‘where am I going’ (the goals), ‘how am I going?’ (feedback) and ‘where to next?’ (advice on progress).23
Additional intervention with reflection
After the CPR training, the students in group RT discussed three reflective questions for 15 min. The teacher asked one question at a time. The students discussed and reflected on each question pairwise. The pairs then shared what they had discussed with the whole class. The teacher summarised the answers and asked the next question. In the present study, the aim of the reflection was afterthought.24 25 Reflections were based on the students’ experience, understanding and knowledge and could be enriched with interpretations from a person with more experience.26 The three questions were: (1) Imagine yourself in a situation where you see a person suffering from a cardiac arrest. Reflect on which factors influence if you would intervene in a real situation? Remember that your actions may be the difference between life and death; (2) You are alone when a person suffers from a cardiac arrest. According to the guidelines, you should first call 112 and then start CPR, why this order?; (3) Place your hands on the correct compression position on yourself. Reflect on the compression position. Why should the heel of the hand be placed in the centre of the victims’ chest? The selection of questions were based on the following: we wanted the students to think about performing a life-saving intervention so that during the training they would consider how they would act in a real-life situation; in a prestudy, most students failed to call 112; and previous studies have shown that a large proportion of participants apply an incorrect hand position during chest compression.27–29
Assessment
Directly after training and at 6 months, the students in all intervention groups answered a fixed-response questionnaire, which included questions on previous CPR training experience and their willingness to act if faced to an OHCA situation (see online supplementary file 2).
At the 6 month-follow-up, the participants in all intervention groups individually performed a practical CPR test (retention test). The retention test was carried out without prior notice and was conducted in same way as the ‘additional intervention with a practical test including feedback’. All measurements were carried out by one investigator (AN), who was blinded to the allocated intervention of the participants.
Study outcome measures
The primary endpoint was the total score for the modified Cardiff test at 6 months. Total score directly after training, the scores in the individual test categories and self-reported willingness to make a life-saving intervention were secondary endpoints.
Statistical plan and analyses
Sample size was calculated based on results from a prestudy.28 To detect a two-point difference in the mean of the total score of the modified Cardiff test, with an assumed SD of 2.5 points, a significance level of 0.05 and a power of 80%, an effective total sample size of 75 students was needed.30 At the first measurement point, we included all available classes (more than calculated) since it is difficult to estimate the size of missing at 6-month follow-up. Cluster randomisation implies that the number of participants is not equal in each training method group due to the different size of the classes. Therefore, a higher number needs to be included to ensure a sufficient number of participants for each method. The intraclass correlation coefficient (95% CI) was 0.26 (0.24 to 0.29).17 31 Based on an average cluster size of 20.2, the design effect caused by the cluster randomisation was calculated to be 5.99. A total of 587 and 549 students performed the first and the second test, respectively. This corresponds to an effective sample size of 98 and 92, respectively, which is above the 75 needed to reach a power of 80%.
To evaluate the effect of test including feedback, group O was compared with group T. To assess the effect of reflection, group T was compared with group RT. These comparisons were prespecified and based on separate research questions, and thus no adjustment for multiple testing was performed as this gives no further information about the cause of differences. Data were presented as proportions (per cent) or mean (SD). Differences in proportions were analysed with Pearson's χ2 test. Differences in mean total score between the intervention groups were assessed using unpaired t-test. To account for a potential cluster effect of the school classes, a mixed models linear test was also applied for comparisons of the total score.17 By calculating the (individual total score−12)/(maximum total score−12)×100, we obtained a measure of CPR quality in relation to optimal CPR. p<0.05 was considered statistically significant. Analyses were performed using IBM SPSS V.21 and STATA V.13.1.
Results
Twenty-nine classes involving 587 students were included in the measurements directly after training; 549 (94%) of these students completed the retest at 6 months (figure 1). The students’ characteristics are summarised in table 1.

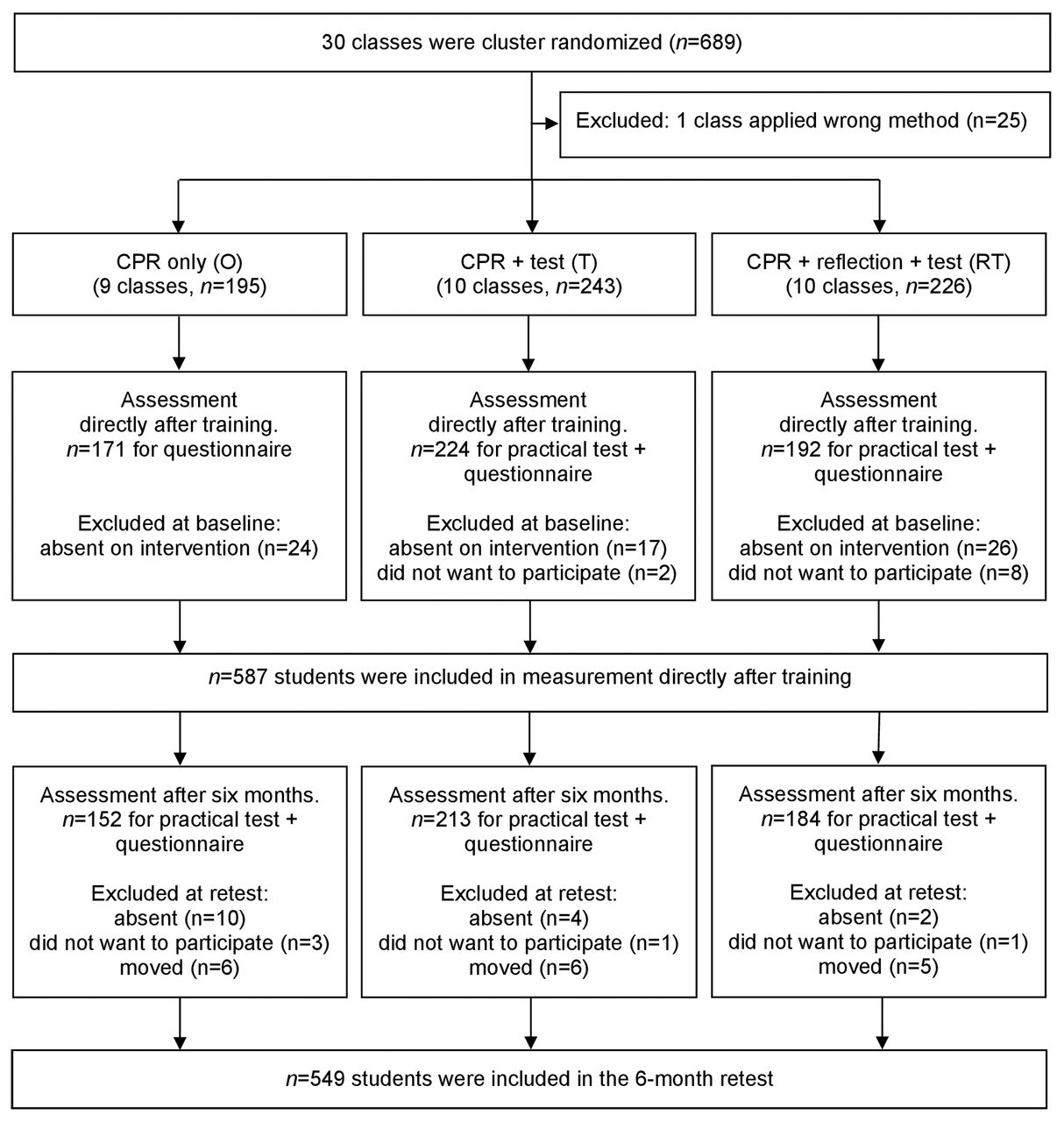{kind=link}
Flow chart on randomisation and inclusion. CPR, cardiopulmonary resuscitation.
Group O versus group T
At 6 months, group T (n=224) performed better than group O (n=171) in terms of total score: 32 (3.9) points (56% of maximum score) versus 30 (4.0) points (50% of maximum score), p<0.001. For the individual variables, group T performed significantly better in 8 of 12 variables. Results of the modified Cardiff test are summarised in table 2.
Assessment of CPR skills at the 6 month follow-up
Group T versus group RT
Directly after training and at the 6-month follow-up, there were no significant differences between group RT (n=192) and group T (n=224) with regard to the total score of the modified Cardiff test, calling 112 or hand position during compressions (table 3). Directly after CPR training, both groups scored 34 points (61% of maximum score); and at the 6-month follow-up, group RT scored 31 (4.2) points (53% of maximum score) and group T scored 32 (3.9) points (56% of maximum score). Table 3 includes the variables of the practical test that are directly linked to the intervention of reflection as well as the total score of the test. All other variables of the test showed no significant differences between the two groups (T vs RT) and have not been included in the table.
Assessment of CPR skills directly after training and at 6 months
Willingness to act
In the questionnaire, students were asked how confident they felt to act in a cardiac arrest situation after participating in the CPR training session compared with prior to training. A lower proportion of the students in group O versus group T stated they felt more confident to act after participating in the training session, when asked directly after training (73% vs 88%; p=0.002) and at 6 months follow-up (73% vs 82%; p=0.025). There were also differences in how the students considered that they had enough knowledge to do chest compressions, 60% (O) versus 81% (T, p<0.001), and to do rescue breathing, 57% vs 75% (p<0.001). At 6 months, 84% (O) versus 91% (T, not significant) considered they had enough knowledge to do chest compressions and 59% (O) versus 74% (T, p=0.007) to do rescue breathing. There were no significant differences between group T and group RT regarding confidence about acting or self-rated knowledge either after training or at 6 months.
Directly after training, most students responded that they would do both compressions and ventilations if a friend suffered OHCA; 72% (O), 80% (T, p=NS when comparing O and T) and 81% (RT, table 3). If a stranger suffered OHCA, there was a significant difference between group T and group RT in how the students would act, with a more positive attitude in group RT (table 3) but there was no significant difference between groups O and T (27% and 32% would do both compressions and ventilations).
At 6-month follow-up, there were no significant differences between the three intervention groups with regard to how they would act in OHCA situations; 76% (O), 73% (T) and 78% (RT) would do both compressions and ventilations if a friend suffered a cardiac arrest. Only 31% (O and T) versus 29% (RT) were prepared to do compressions and ventilations if a stranger suffered a cardiac arrest.
Discussion
The main findings of the present study are threefold. First, adding a practical test with feedback after CPR training resulted in significantly improved practical skills at the 6-month follow-up. Second, reflection added to CPR training did not influence the practical skills. Third, adding a practical test with feedback or reflection to CPR training did not affect long-term willingness to make a life-saving effort. The study was performed in schools of diverse socioeconomic background and each intervention was applied in seven to nine different schools, strengthening the generalisability of our findings.
The group with a practical test including feedback (T) added after CPR training showed superior practical skills at 6 months compared with the group with CPR training only (O). However, the clinical relevance of the two-point difference in the total score for the modified Cardiff test is unclear. We discuss possible reasons for the outcome linked to learning theories. The result may be due to a further 3 min of hands-on training under the supervision of the investigator or due to the individual feedback the students received after the test.14 Previous studies indicate that testing can increase learning outcomes compared with an equal amount of time spent on training.13 15 The test was not only a tool to assess skills but also an opportunity to give the students’ feedback.32 The feedback aimed to reduce discrepancies between present understanding and the goal.23 Li et al 32 indicate that a pretest and feedback can inspire learners to develop strategies to minimise their dependence on feedback from the instructors, which improve skill acquisition and skill retention. At feedback, the question ‘where to next?’ was assumed to be the most important question, while praise for a task seems to be less effective.23 33 A limitation is that the feedback to the students was given when the training was completed. In a prestudy, some students indicated that feedback helped to strengthen their self-esteem.28 According to Bandura,34 and social cognitive theory, an individual's self-efficacy may affect a person's performance. Self-efficacy is about a person's confidence in their own ability (not actual ability) in a given situation. Self-efficacy can be affected by verbal persuasion.35 Further studies are needed to elucidate whether the results were caused by the additional training during supervision or by the feedback given to the students. Use of a feedback device is another form of feedback that may improve skill acquisition.2 A feedback device was not tested in this study.
According to the Swedish school curriculum, knowledge ‘can be expressed in a variety of forms, as facts, understanding, skills, familiarity and accumulated experience’.11 Reflection and practical training are two teaching methods that can contribute to understanding, skills and familiarity. There are many definitions of reflection, which implies that there are many different models.25 26 In this study, the aim of the reflection was afterthought.24 25 Adding reflection to CPR training did not influence the students’ practical skills. In particular, reflection did not improve calling 112 and hand positioning during compressions, despite both being included in the reflective questions. Directly after training, a higher proportion of students in the reflection group were willing to intervene if a stranger suffered a cardiac arrest, but this difference could not be observed at 6 months. This result might, at least in part, be explained by the content and the framing of the reflective questions. The first question, concerning how the students would act in an OHCA situation, is based on ethical considerations, which may provoke emotions and empathy in students.36 These emotions might have affected the participants close to the training but not in the long term. Questions two (calling 112) and three (hand positioning during compressions) were a cognitive complement to the practical training. Thus, the students might have discussed and answered these questions as knowledge questions, rather than questions to reflect on. Perhaps the outcome would have been different if these reflective questions had been asked when the action was practised, so-called reflection on action.26 Mann et al 25 stated that there is no evidence to support or refute the assumption that reflection will enhance competence. Ixer37 stated that we do not know enough about reflection or how it can enhance learning. Further research is needed to clarify whether and how reflection can be used as a successful teaching tool in CPR training.
Practical training increases willingness to intervene in a real situation.2 38 At the 6-month follow-up, the three intervention groups did not differ with regard to willingness to make a life-saving effort. Regardless of the intervention method, we found, in accordance with previous studies, a huge difference in willingness to intervene in an OHCA situation involving a friend compared with a situation involving a stranger.38–41
Study limitations
First, we cannot exclude that students who performed a test directly after training were more familiar with the test manikin at the retention test at 6 months. However, during the test, the participants do not take part of the technical feedback received from the full-body Resusci Anne and should thus not have any advantage. The same design has also been used in other studies.14 27
Second, the characteristics of the CPR instructor may affect the learning process of the students. We have no data on the individual instructors regarding their previous experience of and attitude towards CPR training. However, they were all regular teachers of the participating school classes and prior to the study they all received standardised information on current CPR guidelines and detailed instructions on how to perform their allocated CPR training interventions.
Third, the intervention was carried out in two major municipalities. We do not know how applicable the results are for other locations, but a strength of the present study is that schools from all socioeconomic areas were included.
Conclusions
This study contributes to knowledge on the efficiency of two additional CPR training interventions. A practical test with feedback in connection with CPR training is an efficient strategy to increase learning outcome, both practical skills and self-rated knowledge, when teaching seventh grade students. Further studies are needed to find alternative methods for testing and feedback, and to elucidate how feedback works most effectively in the CPR learning process. Reflective questions, in the format applied in this study, did not increase the participants’ practical CPR skills. Importantly, regardless of the intervention applied, most students indicated they would intervene in an OHCA situation.
Supplementary Material
References
Footnotes
Acknowledgements The authors would like to thank all the students and teachers who participated in the study.
Contributors AN contributed to the study design, developed the modified Cardiff test and the questionnaire, conducted all measurements, analysed results and wrote the initial draft of the manuscript. LS and JH contributed to the study design, developed the modified Cardiff test and revised the manuscript. HH and SKS contributed to the study design and revised the manuscript. LN contributed to the study design, developed the modified Cardiff test and the questionnaire, analysed results and revision of the manuscript.
Funding The study was supported by the Foundation for Cardiopulmonary Resuscitation in Sweden, Swedish Resuscitation Council, Swedish Heart-Lung Foundation (award number 20130629) and the County Council of Östergötland. The funders had no role in study design, data analysis, decision to publish or preparation of manuscript.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval The Regional Ethical Review Board of Linkping, Sweden (2013/358-31).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional unpublished data available.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.