Article Text

Abstract
Introduction Elderly patients who have solid organ cancer often receive surgery. Some of them may develop delirium after surgery and delirium development is associated with worse outcomes. Furthermore, despite all of the advances in medical care, the long-term survival in cancer patients is far from optimal. Evidences suggest that choice of anaesthetics during surgery, that is, either inhalational or intravenous anaesthetics, may influence outcomes. However, the impact of general anaesthesia type on the occurrence of postoperative delirium is inconclusive. Although retrospective studies suggest that propofol-based intravenous anaesthesia was associated with longer survival after cancer surgery when compared with inhalational anaesthesia, prospective studies as such are still lacking. The purposes of this randomised controlled trial are to test the hypotheses that when compared with sevoflurane-based inhalational anaesthesia, propofol-based intravenous anaesthesia may reduce the incidence of early delirium and prolong long-term survival in elderly patients after major cancer surgery.
Methods and analysis This is a multicentre, open-label, randomised controlled trial with two parallel arms. 1200 elderly patients (≥65 years but <90 years) who are scheduled to undergo major cancer surgery (with predicted duration ≥2 hours) are randomised to receive either sevoflurane-based inhalational anaesthesia or propofol-based intravenous anaesthesia. Other anaesthetics and supplemental drugs including sedatives, opioids and muscle relaxants are administered in both arms according to routine practice. The primary early outcome is the incidence of 7-day delirium after surgery and the primary long-term outcome is the duration of 3-year survival after surgery.
Ethics and dissemination The study protocol has been approved by the Clinical Research Ethics Committees of Peking University First Hospital (2015[869]) and all participating centres. The results of early and long-term outcomes will be analysed and reported separately.
Trial registration number ChiCTR-IPR-15006209; NCT02662257; NCT02660411.
- cancer
- surgery
- survival
- anaesthesia in oncology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The trial design is prospective, multicentre and randomised controlled, with a relative large sample size.
The study will investigate the impact of two general anaesthesia techniques, that is, propofol-based intravenous anaesthesia versus sevoflurane-based inhalational anaesthesia, on the outcomes of elderly patients after cancer surgery.
Both early (incidence of 7-day delirium as primary endpoint) and long-term (3-year survival as primary endpoint) outcomes will be explored. These two endpoints are both timely and important.
All study personnel will be trained to follow a standard procedure for the preoperative visit as well as postoperative follow-up assessment. Hence, data will be robust.
A limitation is that the study design is not double-blinded because the differences of anaesthesia management cannot be masked. To decrease the potential bias produced by the open-label design, investigators performing postoperative follow-up are not involved in both anaesthesia implementation and postoperative care.
Introduction
With ageing population together with increasing risk factors, cancer occurrence is increasing both in China and globally.1 2 Surgical resection is the first-line treatment for solid organ cancer and indeed, it is estimated that >234 million major surgical procedures are performed every year worldwide3; of which neoplasm is one of the major reasons of surgery in a global survey.4 Recently, evidences emerge that choice of anaesthetics, that is, either inhalational or intravenous anaesthetics, may influence the outcomes of elderly patients after cancer surgery.
Choice of anaesthetics and early postoperative delirium
Delirium, a state of acute and fluctuating disturbance of consciousness, attention, cognition and perception,5 is a common complication in elderly after surgery. Systematic reviews showed that up to 54% patients develop delirium after non-cardiac surgery, and its occurrence increases with age.6–8 The occurrence of delirium is associated with worse early outcomes, including prolonged hospital stay and increased complications and in-hospital mortality; it is also associated with worse long-term outcomes, including declined cognitive function, decreased quality of life and increased postdischarge mortality.9–15
Underlying mechanisms of delirium development are unknown but it is certainly related to multiple risk factors.16–18 Evidence suggests that choice of anaesthetics may also have an influence. In a study of 2000 patients undergoing general anaesthesia, those carrying ApoE4 epsilon 4 allele were more likely to develop early postoperative cognitive decline after inhalational anaesthesia but not after intravenous anaesthesia.19 In a small trial of 44 patients undergoing carotid endarterectomy, the mini-mental state examination (MMSE) score was higher, whereas blood S100B concentration was lower in the propofol group than in the sevoflurane group at 24 hours after surgery.20 In the study of Tang et al,21 200 elderly (≥60 years) patients with mild cognitive impairment randomly received either sevoflurane or propofol anaesthesia for radical rectal resection. The negative cognitive effects were more severe after sevoflurane anaesthesia than after propofol anaesthesia. Conversely, in a randomised trial of 50 elderly (≥65 years) patients undergoing long-duration laparoscopic surgery, the score of delirium rating scale was lower in the sevoflurane group than in the propofol group on the postoperative days 2 and 3.22 In another trial of 128 patients undergoing on-pump cardiac surgery, postoperative cognitive function was better in the sevoflurane group than in the propofol group in patients who experienced intraoperative cerebral desaturation.23
Caution must be taken when interpreting these findings because: (1) target patient populations are different, (2) the diagnostic criteria of cognitive complications are inconsistent and (3) conclusions of large sample size studies are drawn from exploratory analyses rather than primary endpoints. Therefore, current data are inconclusive and further studies are warranted.
Choice of anaesthetics and long-term outcomes after cancer surgery
Despite all of the advances in oncological science, the long-term outcomes of cancer patients are far from optimal. For example, the 5-year survival rate of Chinese cancer patients is only 36.9%.1 For patients after surgery, cancer recurrence and metastasis are the main factors that worsen the quality of life and shorten the duration of survival. The balance between immune function and cancer invasiveness is a key element that influences the occurrence of cancer recurrence and metastasis after surgery.
The choice of general anaesthetics may influence patient’s immune function. An international multicentre team investigated the effects of propofol–paravertebral anaesthesia versus sevoflurane–opioid anaesthesia on the immune function in patients undergoing breast cancer surgery (NCT00418457). The preliminary data published by this team so far indicated that propofol anaesthesia may be better than sevoflurane anaesthesia in preserving immune function after surgery.24–26 Similar findings were also reported in patients undergoing surgery for non-small-cell lung cancer27 and tongue cancer.28 Taken together, it seems that propofol anaesthesia may have favourable effects on postoperative immune function when compared with inhalational anaesthesia. However, conclusions cannot be made because (1) the sample sizes of those studies are small and (2) the casual relationship between immune function and long-term outcomes has not been established yet.
The effects of general anaesthetics on cancer invasiveness are mainly tested in cultured cancer cells. Propofol decreases cancer cell invasion and migration.29–31 On the other hand, inhalational anaesthetics in this regard is controversial. Isoflurane was found to increase cancer cell proliferation and migration,32 33 whereas sevoflurane and desflurane were found to decrease proliferation and migration.34–37 The reasons for this discrepancy are unknown but the duration and concentration of exposure used in those studies are likely responsible.
Clinical studies in this aspect are very limited. In a retrospective study of 2838 patients who underwent breast or colorectal cancer surgery, 1935 received sevoflurane anaesthesia and 903 propofol anaesthesia. The 1- and 5 year survival rates were higher in propofol-anaesthesised patients. However, the differences were not statistically significant after adjustment with confounding factors.38 In another study, 11 395 patients after cancer surgery were retrospectively analysed. After exclusions and propensity matching, 2607 patients remained in each of the inhalational anaesthesia group or total intravenous anaesthesia group. The results showed that, after a median follow-up duration of 2.66 years, volatile inhalational anaesthesia was associated with a higher risk of death.39
We hypothesise that, when compared with sevoflurane-based inhalational anaesthesia, propofol-based intravenous anaesthesia may be beneficial on long-term survival in elderly after cancer surgery. However, due to the retrospective natures of previous publications, properly designed randomised controlled trials are urgently needed to figure out the better anaesthetic regimen for cancer patients.
Study objectives
The objectives are to investigate the impact of inhalational versus intravenous anaesthesia on the occurrence of delirium and long-term survival in elderly after major cancer surgery.
Methods and analysis
The protocol is developed in accordance with the Recommendations for Interventional Trials (SPIRIT).40 The SPIRIT Checklist for this protocol is available as ‘supplement’. The trial is registered at Chinese Clinical Trial Registry (www.chictr.org.cn) with identifier ChiCTR-IPR-15006209; and at clinicaltrials.gov with identifier NCT02662257 for early outcomes and identifier NCT02660411 for long-term outcomes. The latest V.3.5 of the trial protocol was approved on 19 April 2017.
Trial design and setting
This multicentre, open-label, randomised controlled trial with two parallel-arms is designed to compare the difference of two interventions. Eligible patients will be enrolled and randomly assigned to receive either sevoflurane-based inhalational anaesthesia or propofol-based intravenous anaesthesia (figure 1). The study will be coordinated by the Department of Anesthesiology and Critical Care Medicine of Peking University First Hospital, and will be conducted in the Departments of Anesthesiology of 17 tertiary hospitals in China.

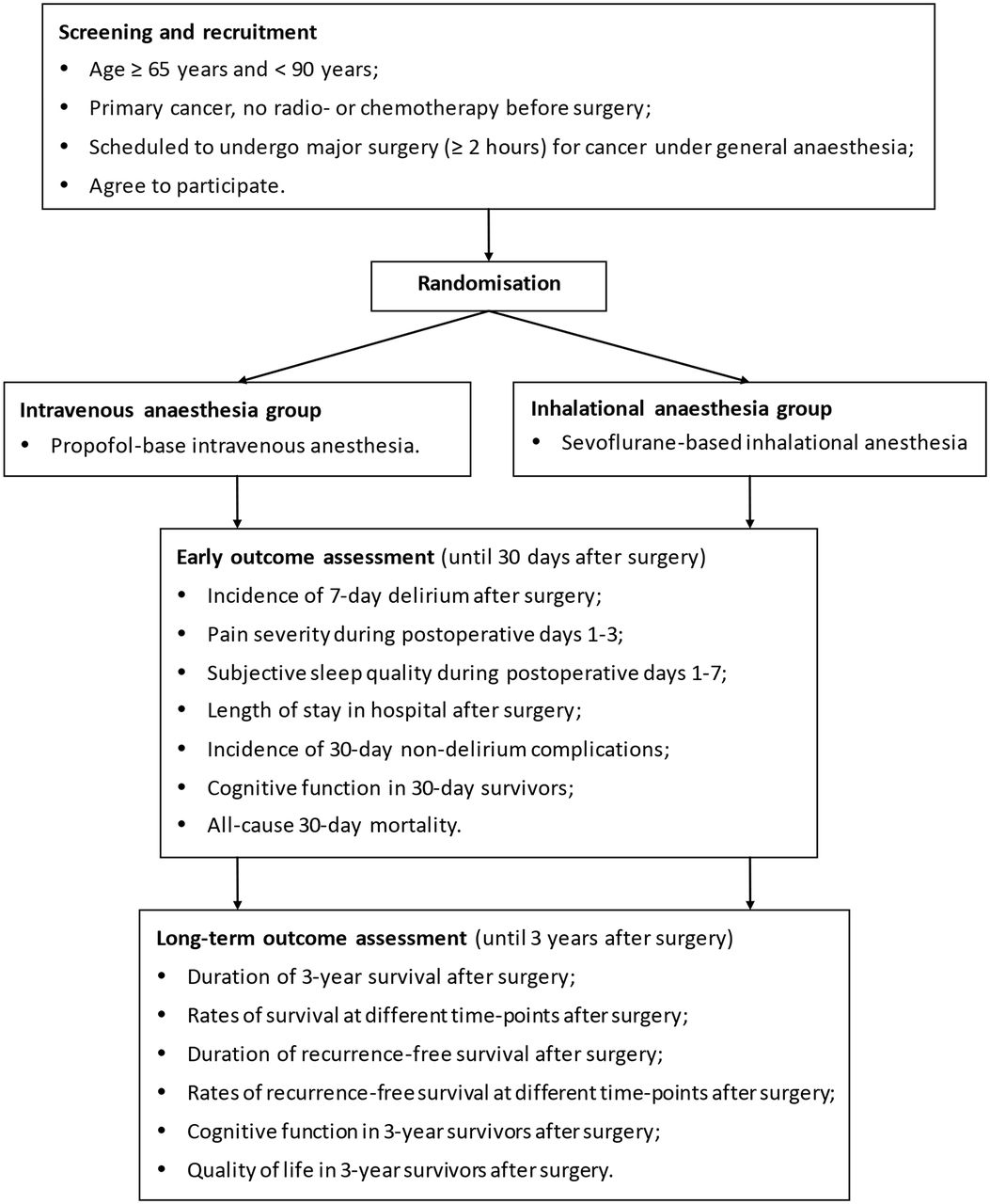{kind=link}
Flowchart of the study.
Participant selection
Inclusion criteria
Participants will be included if they meet all of the following criteria: (1) age ≥65 years and <90 years; (2) diagnosed as primary cancer, do not receive radiotherapy or chemotherapy before surgery; (3) scheduled to undergo surgery for cancer, with an expected duration of 2 hours or more, under general anaesthesia; (4) agree to participate, and give signed written informed consents.
Exclusion criteria
Patients will be excluded if they meet any of the following criteria: (1) preoperative history of schizophrenia, epilepsy, parkinsonism or myasthenia gravis; (2) inability to communicate in the preoperative period because of coma, profound dementia, language barrier or end-stage disease; (3) critical illness (preoperative American Society of Anesthesiologists physical status classification ≥IV), severe hepatic dysfunction (Child-Pugh class C) or severe renal dysfunction (undergoing dialysis before surgery); (4) neurosurgery; (5) refuse to participate in the study or (6) other reasons that are considered to be unsuitable for study participation by the responsible surgeons or investigators (reasons must be recorded in the case report form).
Sample size calculation
For the purpose of delirium reduction
In our recent study, the incidence of postoperative delirium in a comparable patient population was 8%. In a small sample size study comparing the effects of propofol-based versus sevoflurane-based anaesthesia, the incidence of delirium during the first three postoperative days was 16% (4/25) versus 0% (0/25).22 In another study, comparing the effect of sevoflurane versus propofol general anaesthesia, the incidence of severe cognitive dysfunction at 7 days after surgery was 16.1% (16/99) versus 5.9% (6/101).21 We propose that the incidence of delirium will be reduced from 8% in the sevoflurane group to 4% in the propofol group (ie, a 50% reduction). With significance and power set at 0.05% and 80%, respectively, the sample size required to detect difference was 1106 patients. Taking into account a loss-to-follow-up rate of about 6%, we need to enrol 1177 patients.
For the purpose of long-term survival improvement
In our previous study, the 3-year mortality rate of elderly patients after cancer surgery was 30%. In a retrospective study of Wigmore et al,39 the mortality rate at a median 2.66 years after cancer surgery was 13.6% in patients after total intravenous anaesthesia and 24% in those after inhalational anaesthesia (ie, a 43.3% decrease with total intravenous anaesthesia). We propose that the 3-year mortality rate will be reduced from 30% in the sevoflurane group to 20% in the propofol group (ie, a 33% reduction). With significance and power set at 0.05% and 80%, respectively, the sample size required to detect difference was 588 patients. Taking into account a loss-to-follow-up rate of about 20%, we need to enrol 735 patients.
Final sample size of the study
After considering the two calculated sample size, we plan to enrol 1200 patients in the present study.
Patient recruitment and baseline data collection
The day before surgery (or Friday for patients who will undergo surgery the next Monday), investigators who have been trained for the study conduct process and delirium assessment and are authorised by the principal investigator will screen potential participants according to the inclusion and exclusion criteria. Written informed consents (see online Supplementary file 1) will be obtained from eligible patients, their next of kin or their legal representatives. To promote participant retention and complete follow-up, the addresses and telephone numbers of both patients and their relatives are collected after obtaining consents.
Supplementary Material
For recruited patients, baseline data will be collected. These include demographic data (age, gender, education level and body mass index), current and previous histories of diseases (surgical diagnosis, comorbidity, medical treatment and surgical history), as well as main results of physical, laboratory and instrumental examinations. Severity of comorbid disorders (assessed with Charlson comorbidity index and New York Heart Association cardiac function classification) and evaluation of physical status (assessed with American Society of Anesthesiologists physical status classification and Barthel Index) will be recorded. Cognitive function (assessed with MMSE), delirium status (assessed with confusion assessment method (CAM)) and pain severity (assessed with numerical rating scale (NRS), an 11-point scale where 0=no pain and 10=the most severe pain) will also be collected.
Randomisation
A biostatistician who does not participate in data management and statistical analysis generate random numbers in a 1:1 ratio, with a block size of 4, using the SAS V.9.2 software package (SAS Institute, Cary, North Carolina, USA). Randomisation is stratified by centres. The results of randomisation are sealed in the envelopes and stored at the site of investigation until the end of the study.
For each study centre, a study coordinator is assigned to preserve and distribute randomisation results according to the sequence of recruited patients, and to coordinate between investigators. For each recruited patient, group assignment will be clarified in the operating room on the day of surgery; an anaesthesiologist will be assigned for anaesthesia management and intraoperative data collection. Postoperative follow-up will be performed by investigators who do not participate in patient care and have been trained to follow-up patients prior to the study. Both anaesthesiologist(s) and investigator(s) do not communicate with each other while collecting data.
Anaesthesia management and study intervention
No preanaesthesia medication will be given. Intraoperative monitoring include ECG, non-invasive blood pressure, pulse oxygen saturation, bispectral index (BIS), end-tidal partial pressure of carbon dioxide, end-tidal concentration of inhalational anaesthetics, nasopharyngeal temperature and urine output. Intra-arterial blood pressure (including parameters derived from arterial pressure waveform, such as stroke volume variation (SVV) from a FloTrac system), central venous pressure and thermodilution cardiac output (measured through a pulmonary artery catheter or a PiCCO system) may be monitored when necessary.
Anaesthesia will be induced intravenously with midazolam, opiates (remifentanil, sufentanil and/or fentanyl), propofol and muscle relaxants (rocuronium or cisatracurium). For patients with predicted difficult airway, succinylcholine may be used for rapid sequence intubation or awake intubation may be performed. Dexamethasone (4–5 mg) may be administered before anaesthesia induction for the prevention of postoperative nausea and vomiting.
For patients in the sevoflurane group, anaesthesia will be maintained with sevoflurane inhalation, of which the concentration will be adjusted to maintain the BIS value between 40 and 60. For patients in the propofol group, anaesthesia will be maintained with propofol infusion, of which the infusion rate will be adjusted to maintain the BIS value between 40 and 60. For patients of both groups, analgesia will be maintained with remifentanil, sufentanil and/or fentanyl; muscle relaxation will be maintained with rocuronium or cisatracurium.
Intraoperative mechanical ventilation will be established with a tidal volume between 6 and 8 mL/kg, a positive end-expiratory pressure of 5 cm H2O, a plateau pressure of <30 cm H2O, a frequency between 12 and 16 per minute and a 1:1 air–oxygen mixture. Intraoperative fluid therapy will be managed according to routine practice. Packed red blood cells will be transfused when necessary in order to maintain haemoglobin levels within the target range of 7–10 g/dL. Vasopressors and/or inotropics will be administered when necessary in order to maintain systolic blood pressure within 20% of baseline.
Postoperative analgesia during the first 3 days will be provided by a patient-controlled analgesia pump, which is established with morphine (0.5 mg/mL) or sufentanil (1–2 µg/mL), programmed to deliver a 2 mL bolus with a lockout interval of 6–10 min and a background infusion of 1 mL/h. The pump setting may be adjusted according to patients’ condition. Other opiates and non-steroid anti-inflammatory drugs can also be used for postoperative analgesia. Postoperative analgesia after that period will be provided by intravenous injection or oral intake.
Intraoperative data including the type of surgery, durations of anaesthesia and surgery, doses of anaesthetics, analgesics and other drugs used during anaesthesia, fluid balance and transfusion of blood products, as well as fluctuation of monitoring variables will be collected by the anaesthesiologists. For all enrolled patients, dexmedetomidine is not allowed; scopolamine and penehyclidine are prohibited; atropine is used only for the purpose of reversing bradycardia. For patients who deviate from the study protocol, deviations will be corrected whenever possible and follow-up will be completed. The results of these patients will be included in the intention-to-treat analysis.
Patient follow-up and outcome assessment
Early postoperative outcomes
Patients will be followed up two times per day during the first 7 days after surgery, and then weekly until the 30th day after surgery (by telephone for those who are discharged from the hospital) by the investigators.
Delirium will be assessed two times per day, that is, between 8–10 am and 6–8 pm, during postoperative days 1–7. Intubated patients will be assessed with the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU), and non-intubated patients will be assessed with the CAM. For patients who are discharged from hospital, withdraw consents or die within 7 days after surgery, the last follow-up results will be regarded as the final results.
Pain severity, both at rest and with movement (such as during coughing), will be evaluated with the NRS two times per day during postoperative days 1–3. Subjective sleep quality will be evaluated with the NRS (an 11-point scale where 0=the worst sleep, and 10=the best sleep) once daily, that is, between 8 and 10 am, during postoperative days 1–7. Medications (including sedatives, analgesics, anticholinergics and glucocorticoids) used during postoperative days 1–7 will be recorded.
The occurrence of non-delirium complications, which are defined as newly occur medical conditions that are harmful for patients’ recovery and require therapeutic intervention, will be monitored during postoperative days 1–30. Other postoperative data including admission to the intensive care unit (ICU), the lengths of both ICU and hospital stay after surgery, and readmissions after hospital discharge within 30 days will be recorded. For patients who die within 30 days after surgery, the exact date of death will be recorded. For 30-day survivors, cognitive function will be assessed with Telephone Interview for Cognitive Status-Modified (TICS-m, Chinese version).
For early postoperative outcomes, the primary endpoint is the incidence of delirium during the first 7 days after surgery. Secondary endpoints include ICU admission after surgery, length of stay in hospital after surgery, the incidence of non-delirium complications (including readmission after hospital discharge) during the first 30 days after surgery, cognitive function of 30-day survivors and all-cause 30 day mortality. Other endpoints include pain severity during postoperative days 1–3 and subjective sleep quality during postoperative days 1–7.
Long-term postoperative outcomes
Patients will be followed up (by telephone) one time yearly until the third year after surgery by the investigators. The results of pathological diagnosis and the final cancer stage at hospital discharge will be documented. The performance of postoperative re-examinations and therapies for the primary cancer will be recorded. The results of re-examination will be judged by surgeons (and radiologists when necessary) for cancer recurrence and metastasis; the date of confirmed recurrence and/or metastasis will be documented. Postoperative therapies including radiotherapy, chemotherapy, reoperation and other therapies will be collected. Other data including newly diagnosed tumour (ie, tumour that is definitely different from the primary one) and disease (ie, disease that is different from the recorded preoperative comorbidity) will be recorded.
For patients who die within 3 years after surgery, the exact date of death will be recorded. For 3- year survivors, quality of life will be assessed with the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30); cognitive function will be assessed with the TICS-m (Chinese version).
For long-term postoperative outcomes, the primary endpoint is the duration of 3-year survival after surgery. Secondary endpoints include rates of survival at different time points after surgery, duration of recurrence-free survival after surgery, rates of recurrence-free survival at different time points after surgery, as well as quality of life and cognitive function in 3-year survivors after surgery.
Safety consideration
In the present study, the intervention measures administered for patients of both groups are anaesthesia methods currently being used during daily practice. Therefore, our study will not produce additional risk on participants. However, adverse events may occur even during a normal anaesthesia. In such case, anaesthesiologists will manage patients according to routine practice. The occurrence of adverse events will be monitored from the beginning of anaesthesia until 24 hours after surgery.
An adverse event means any unpredictable, unfavourable medical event that is associated with any medical intervention and occurs during the study period. It can be related to the study intervention or otherwise. It can manifest as any uncomfortable signs (including abnormal laboratory findings), symptoms or transient morbidity. A severe adverse event indicates any unpredictable medical events that lead to death, threat of life, prolonged length of hospital stay, persistent disability or dysfunction, or other severe event.
Any adverse events will be treated promptly according to routine practice, followed up until it is completely resolved or therapy is terminated, and documented. Documentation of adverse events include the following, that is, time of occurrence, diagnosis, time of diagnosis, management, duration of persistence, sequelae and severity. The occurrence of severe adverse events will be reported to the local ethics committee as soon as possible.
Data management and monitoring
All original data will be recorded in the Case Report Forms accordingly. The completed Case Report Forms, after signed by the supervisors, will be sent to the Clinical Research Institute of Peking University. Data entry will be doubly performed by two persons using the EpiData3.10 database system. A data manager will perform database check out using SAS V.9.2 software. Data queries will be answered by investigators. After data entry and database check out are completed and all problems encountered during the procedure solved, the database will be locked. The decision to lock database will be made by the principle investigator, the database manager and a statistician who is responsible for statistical analysis. Investigators and a statistician who are authorised by the principal investigator have access to the final trial dataset.
Considering the fact that both inhalational and intravenous general anaesthesia are routinely performed in daily practice and no additional risk is produced to participants, no interim analysis will be performed and the trial will continue until the target sample size is achieved.
The conduct of the study will be monitored by study coordinator(s) and supervisor(s) in each centre. Auditing for the trial conduct will be carried out eight times by an independent auditor (MRW) from Peking University Clinical Research Institute. Data management and statistical analysis will be performed by the Peking University Clinical Research Institute.
Statistical analysis
Analyses will be performed on an intention-to-treat basis, that all subjects will be analysed in the group which they are assigned to. Per-protocol analyses will also be performed for the primary endpoints. All statistical analyses will be performed with SAS V.9.2 software (SAS Institute, Cary, North Carolina, USA).
Numeric variables will be presented as mean (SD) or median (minimum, maximum; or IQR) and analysed with independent sample t test or Wilcoxon rank sum test. Categorical variables (including the incidence of 7 day delirium after surgery) will be presented as number of cases (percentage) and analysed with Χ2 test, continuity correction Χ2 test or Fisher exact test. Time-to-event variables (including the duration of 3-year survival after surgery) will be analysed with Kaplan-Meier survival analysis, with difference between groups assessed with log-rank test. A Cox proportional hazard model will be used to calculated hazard ratio (HR) and the 95% CI to estimate the between group difference. Subgroup analyses will be performed according to the locations and the final pathological diagnoses of cancers.
Two-tailed tests will be used in all statistical analyses, and p values of <0.05 will be considered to be of statistical significance (unless otherwise specified).
Participant timeline
Participant recruitment and data collection were started in April 2015. The recruitment will continue until sufficient participants (1200 patients) are enrolled, which is scheduled at the end of September 2017. Early postoperative follow-up will be completed in October 2017. Long-term postoperative follow-up will be completed in October 2020. Data analysis and evaluation for early and long-term outcomes will be performed separately for publications.
Ethics and dissemination
The study protocol has been approved by the Clinical Research Ethics Committee of the Peking University First Hospital (first version protocol approved on 13 April 2015 with number 2015[869]) and the Ethics Committees of all participating centres. Any revision of the study protocol must be approved by the Ethics Committee before it can be executed in the study. During the study period, Declaration of Helsinki and Chinese guidelines of Good Clinical Practice are strictly followed in order to guarantee the right of the participants. The principle investigator (DXW) will submit report of the study progress to the local Ethics Committee regularly.
For every potential participant, the investigators will explain in detail the study purposes, procedures, as well as potential benefits and risks from the study in a written informed manner. The investigators must let every potential participant know that he/she has the right to withdraw consent at any time during the study period. Every potential participant must be given sufficient time for careful consideration before making decision. Every participant or the authorised surrogate of the participant must sign the consent before he/she can be enrolled in the study. Written informed consents will be kept as a part of the clinical trial documents.
Personal information of all participants will be confidentially kept. All related documents will be locked up and preserved according to the Chinese guidelines of Good Clinical Practice. For each participant, all data collected during the study period will be identified by a serial number and a name acronym in the Case Report Forms. Results of the study will be presented at academic conferences and submitted to peer-reviewed journals.
Acknowledgments
The authors thank Professor Xin-Yu Sun (Department of Psychiatry, Peking University Sixth Hospital, Beijing, China) for her help in psychiatric consultation and investigator training, and Drs Dong-Liang Mu, Xian Su, Ya-Wei Li and nurses Cui Yuan, Xiao-Jing Liu and Bin Wei (Department of Anesthesiology and Critical Care Medicine) for their help in investigator training.
References
Footnotes
Contributors D-XW: conceived the study and is the principal investigator and has overall responsibility for the trial. YZ and D-XW: drafted the protocol. H-JL: revised the parts of data management and statistical analysis. H-QJ, Q-SY, L-HP, WO, ZJ, X-DS, F-XZ, Y-QG, Q-GZ, X-DY, H-YT, B-JZ, Y-QA, NY, Z-HL, J-BY and DM: participated in the study design and coordination of the study. All authors: read and approved the final manuscript.
Funding This study is supported by grants from the Wu Jieping Medical Foundation, Beijing, China (320.6750.15175) and the Chinese Society of Cardiothoracic and Vascular Anesthesiology, Beijing, China. The study sponsors have no role in study design, in the collection, analysis, and interpretation of data, in the writing of the report, or in the decision to submit the report for publication. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Wu Jieping Medical Foundation or the Chinese Society of Cardiothoracic and Vascular Anesthesiology.
Competing interests DXW is supported by grants from the Wu Jieping Medical Foundation(320.6750.15175), China and the Chinese Society of Cardiothoracic and Vascular Anesthesiology, China; he reports lecture fees and travel expenses for lectures from Jiangsu Hengrui Medicine Co Ltd, China, Yichang Humanwell Pharmaceutical Co Ltd, China, and Jiangsu Nhwa Pharmaceutical Co Ltd, China. DM is supported by grants from the British Oxygen Chair, and British Journal of Anaesthesia Fellowship, London, UK.
Patient consent Obtained.
Ethics approval The study protocol has been approved by the Clinical Research Ethics Committee of the Peking University First Hospital (first version protocol approved on 13 April 2015 with number 2015[869]) and the Ethics Committees of all participating centers. Any revision of the study protocol must be approved by the Ethics Committee before it can be executed in the study.
Provenance and peer review Not commissioned; externally peer reviewed.