Article Text

Abstract
Objectives This study evaluated the uptake of Western Australian (WA) pharmacist vaccination services, the profiles of consumers being vaccinated and the facilitators and challenges experienced by pharmacy staff in the preparation, implementation and delivery of services.
Design Mixed-methods methodology with both quantitative and qualitative data through surveys, pharmacy computer records and immuniser pharmacist interviews.
Setting Community pharmacies in WA that provided pharmacist vaccination services between March and October 2015.
Participants Immuniser pharmacists from 86 pharmacies completed baseline surveys and 78 completed exit surveys; computer records from 57 pharmacies; 25 immuniser pharmacists were interviewed.
Main outcome measures Pharmacy and immuniser pharmacist profiles; pharmacist vaccination services provided and consumer profiles who accessed services.
Results 15 621 influenza vaccinations were administered by immuniser pharmacists at 76 WA community pharmacies between March and October 2015. There were no major adverse events, and <1% of consumers experienced minor events which were appropriately managed. Between 12% and 17% of consumers were eligible to receive free influenza vaccinations under the National Immunisation Program but chose to have it at a pharmacy. A high percentage of vaccinations was delivered in rural and regional areas indicating that provision of pharmacist vaccination services facilitated access for rural and remote consumers. Immuniser pharmacists reported feeling confident in providing vaccination services and were of the opinion that services should be expanded to other vaccinations. Pharmacists also reported significant professional satisfaction in providing the service. All participating pharmacies intended to continue providing influenza vaccinations in 2016.
Conclusions This initial evaluation of WA pharmacist vaccination services showed that vaccine delivery was safe. Convenience and accessibility were important aspects in usage of services. There is scope to expand pharmacist vaccination services to other vaccines and younger children; however, government funding to pharmacists needs to be considered.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study that comprehensively evaluated the implementation of pharmacist immunisation services in Australia and the uptake of the services.
Mixed methodology was employed to obtain quantitative and qualitative data through surveys, pharmacy computer records and interviews.
The various data sources enabled contextualising and triangulation of information and hence enriched the exploration of the research topic.
Voluntary self-administered baseline and exit surveys to pharmacists who chose to provide pharmacist immunisation services and interviews with immuniser pharmacists could have caused participant bias.
This study was conducted in Western Australia and findings might differ in other Australian jurisdictions due to slight differences in legislative provisions.
Background
Immunisation is one of the most significant public health interventions of the past 200 years, preventing the spread of many diseases that result in serious ongoing health outcomes, hospitalisations and sometimes death.1 It has been estimated that vaccines prevent more than 2.5 million deaths annually.2 The underusage of immunisation programmes, however, continues to be a significant public health concern.3 ,4 Factors that contribute to low immunisation rates have been reported in various studies5–7 and include misconceptions, inconvenience, cost and general public apathy.8
Community pharmacists are accessible healthcare professionals who provide health advice and expertise across a wide range of health-related areas.9 Adding pharmacists to the list of health professionals who may administer vaccines has the potential to increase vaccine uptake. Pharmacists have been providing vaccination services over the last decade in countries such as the USA,10 the UK,11 Canada,4 Portugal12 and New Zealand (NZ).13 The easy access to community pharmacists is one of the major benefits of pharmacist immunisations and these programmes have been shown to lead to increased vaccination rates, low adverse effects and high consumer satisfaction.9 ,14–21
In the USA, the types of immunisations and the age groups to which they can be delivered vary between states and include seasonal influenza and travel vaccines, human papilloma virus (HPV), hepatitis A and B, meningococcal and pneumococcal vaccines. In some states, certain vaccines can be administered by pharmacists to children as young as 6 years of age.15 Pharmacists in Canada have been administering seasonal influenza vaccinations for people 5 years and over since 2012.17 ,18 Similar programmes have been trialled through some community pharmacies for several years in the UK for seasonal influenza while others include travel vaccinations and HPV.20–22 In 2015, a national England-wide programme was introduced for community pharmacy influenza vaccinations.23 In NZ, pharmacists have been able to vaccinate consumers over 18 years of age since 2011.24 Apart from influenza vaccinations, suitably qualified pharmacists are able to administer the combined diphtheria, tetanus and acellular pertussis vaccine, meningococcal and zoster vaccines to adults with expectations of expansions in the near future.24
In December 2013 the Pharmacy Board of Australia (PBA) announced that vaccination was within the scope of practice of pharmacists.25 The Australian Pharmacy Council subsequently developed training accreditation standards26 and professional organisations developed practice guidelines.27 ,28 As the administration of medicines, including vaccinations, is regulated under jurisdictional medicines and poisons legislation29 individual jurisdictions had to amend legislation to allow pharmacists to administer vaccines.30 In early 2014, the Queensland Pharmacist Immunisation Pilot (QPIP) was introduced and resulted in 11 475 adults (individuals aged 18 years and over) being vaccinated against influenza. More than 8000 consumers completed a postvaccination survey showing 93% satisfaction with the service.31 The pilot was broadened to the Northern Territory in July 2014 and expanded to vaccinations for measles and whooping cough.32
In December 2014, Western Australia (WA) was the first state to make legislative changes allowing state-based implementation of pharmacists to administer influenza vaccines to adults (defined as over the age of 18 in WA) without a prescription, in a pharmacy, under the WA Pharmacist Vaccination Code.33 ,34 The Code specifies that WA pharmacists should refer individuals who qualify for the National Immunisation Program (NIP) to participating NIP service providers such as a medical practitioner. In other words, there has been no specific government funding arrangement in WA and individuals who decide to receive pharmacist-administered influenza vaccinations have to pay at a price determined by the individual pharmacies or be reimbursed by their private health insurance providers. In Australia, those who qualify to receive free influenza vaccinations under the NIP include:35
Individuals aged 65 years and over;
Aboriginal and Torres Strait individuals aged 6 months to <5 years;
Aboriginal and Torres Strait individuals aged 15 years and over;
Pregnant women;
Individuals aged 6 months and over with chronic medical conditions which can lead to influenza complications, for example, severe asthma, low immunity, heart or lung disease or diabetes.
Other jurisdictions namely South Australia, New South Wales, Tasmania and the Australian Capital Territory subsequently introduced similar legislative changes.36 In May 2016, the Victorian Government announced its approval of pharmacist-delivered vaccinations, enabling pharmacists in Victoria to administer influenza and pertussis-containing vaccinations to adults (over the age of 17) on successful completion of relevant training. This includes vaccinations provided to individuals who qualify for free vaccinations under the NIP and the Victorian Government Parent's Whooping Cough Vaccination programme.37
The structured evaluation of WA pharmacist vaccination services from pharmacists' perspectives as well as the potential public health impact was vital to assess the initial implementation and sustainability of this new initiative. This paper reports on the evaluation of pharmacist vaccination services provided in 2015.
Objectives:
Explore the uptake of pharmacist-administered vaccination services;
Evaluate the profiles of consumers who received pharmacist-administered influenza vaccinations in 2015;
Evaluate the facilitators and challenges experienced by pharmacy staff in the preparation, implementation and delivery of services.
Methods
Mixed methodology was employed involving quantitative as well as qualitative approaches to obtain data from a number of sources:
Pharmacy baseline survey completed by pharmacy staff at the initiation of the project to gather information about pharmacy profiles;
End-of-project pharmacy exit survey completed by pharmacy staff to obtain information about services provided, adverse events, facilitators and challenges;
Audit of pharmacy vaccination service records to evaluate services provided and consumer profiles;
Exit interviews with immuniser pharmacists to explore immuniser pharmacists' perspectives on their training, services provided, adverse events and broader impacts.
Surveys and the exit interview tool were developed considering the literature and were validated by the Project Evaluation Team, four pharmacy academics and two independent pharmacists, and were subsequently amended to incorporate suggestions.
Recruitment
A total of 309 WA pharmacists successfully completed pharmacist immunisation training between March and June 2015, and were employed at 158 WA community pharmacies. Of the pharmacies, 133 offered pharmacist vaccination services in 2015 and were eligible to participate in the study. Purposive sampling was used to invite these pharmacies to participate. The pharmacies received a study information sheet and pharmacy owner/manager and pharmacist consent forms during visits by representatives of pharmacy professional organisations. The representatives provided assistance with the implementation of pharmacist vaccination services.
Pharmacy baseline survey
Surveys were subsequently sent by mail to participating pharmacies in April 2015 to collect data about the profile of the pharmacy, previous and intended provision of vaccination services, staff profiles including details about the immuniser pharmacist(s), reasons for providing vaccination services, how appointments would be managed and price to be charged. Follow-up emails and phone calls were made to increase response rates.
Pharmacy exit survey
During August 2015, participating pharmacies were invited to complete another survey to collect information about the vaccination services provided, whether there were any consumers who experienced an adverse event (mild local reaction, mild systemic reaction, severe reaction, epinephrine required), the impact of the service on professional relationships (ie, with general practices) and planned provision of future vaccination services. Surveys were mailed to the pharmacies and follow-up emails and phone calls made to increase response rates.
Pharmacy computer records
Data from some participating pharmacy computer records were collected and compiled mid-October 2015, several weeks after the end of the influenza season. De-identified data from consumers who received pharmacist vaccination services provided information about service dates (peaks and troughs), the number of consumers who received services and consumers' demographics.
Pharmacist exit interviews
Immuniser pharmacists were invited to participate in a semistructured telephone interview to explore opinions about immunisation training, implementation of the service, experiences with consumers including the management of adverse effects, facilitators and challenges experienced in the implementation of the service and the impact of the service.
Immuniser pharmacists who agreed to be interviewed were categorised based on the number of vaccinations delivered, the type of pharmacy where the vaccination service was delivered and the Pharmacy Access/Remoteness Index of Australia (PhARIA)38 category. Of the 44 pharmacists that agreed to be interviewed, 25 were chosen as this number was estimated to be sufficient to reach thematic saturation.39 ,40 Interviewees were selected according to the range, type of pharmacy and PhARIA category to reflect a representative sample. Interviews were conducted in October 2015. Each participant received a $50 gift card as a token of appreciation.
Data analysis
Simple descriptive statistics (frequencies and percentages for categorical variables, medians and ranges for variables measured on a continuous scale) were used to summarise the baseline and exit survey responses. Similar descriptive statistics were used to summarise the pharmacy computer records or vaccinations provided. A Poisson regression model was used to explore any factors associated with the proportion of pharmacists employed at each pharmacy who were immunisers. The dependent variable for this model was the number of immuniser pharmacists, with the total number of pharmacists at the pharmacy identified as the ‘offset’ variable. The results are expressed as rate ratios, their 95% CIs and p values. A general linear model was used to explore factors associated with the number of vaccinations performed. As this dependent variable was skewed, analysis was performed on its logarithm. In the results, means are quoted on the original scale (for ease of interpretation) and the p values are quoted from analysis of the log-transformed data. The Statistical Package for the Social Sciences (SPSS; IBM Corporation. IBM SPSS Statistics for Windows, Version 22.0. Armonk, New York: IBM Corp, Released 2013) V.22 software was used for quantitative data analysis, and a p value <0.05 was taken to indicate a statistically significant association in all tests.
Interviews were audio-recorded, then de-identified and transcribed verbatim. NVivo V.10 was used to organise qualitative data and thematic analysis of the data were informed by the general inductive approach.41 The transcripts were read repeatedly to gain an in-depth understanding of the topics that had emerged from the interviews. Initial codes or ‘ideas’ were generated and then grouped into categories to form the subthemes. These subthemes were then rearranged to form the six main themes.
Results
Pharmacy baseline and exit surveys as well as pharmacy computer records provided quantitative data. Qualitative results reflected immuniser pharmacist interviews.
Pharmacy baseline survey
Of the 133 pharmacies that provided pharmacist vaccination services in 2015, 86 (64.7%) pharmacy owners/managers agreed to take part in the study and returned baseline surveys.
Table 1 summarises the profiles of the participating pharmacies. The majority of pharmacies were in neighbourhood shopping centres (36.0%) or city/suburb/town centre locations (24.4%). The overall percentage of pharmacists working at each pharmacy who were trained immunisers varied from 20% to 100%. The proportion of pharmacists who were immunisers varied from 45% in city/suburb/town locations to 58% in standalone pharmacies, and 70% in regional pharmacies. However, these proportions were found not to be statistically significantly different using the Poisson regression model (p=0.118). When comparing the proportions between urban (47%) and regional pharmacies, the higher proportion in the regional areas did appear to be marginally statistically significant (rate ratio 1.5; 95% CI 1.0 to 2.2; p=0.048).The majority of pharmacies (73%) typically had at least two pharmacists in the pharmacy at any specific time. The number of vaccinations performed during 2015 in pharmacies where only one pharmacist was generally working was lower than others (raw means 129 vs 224; mean difference on log scale 0.65; 95% CI 0.00 to 1.29; p=0.049). While the difference on the original scale appears large (partly due to skewness), the analysis of the log-transformed data showed the difference was of borderline statistical significance. In this situation, the pharmacist may have insufficient time to provide vaccinations and deal with other job demands. However, pharmacies with only one pharmacist on duty are also more likely to be smaller pharmacies dealing with a smaller number of customers, so no particular conclusion can be drawn on this association.
Pharmacy categories, profiles and 2015 vaccination services provided
A large number of pharmacies had 1 (45.3%) or 2 immuniser pharmacists (33.7%). There were a total of 346 pharmacists (123 owners/managers, 223 other employed pharmacists) at the 86 pharmacies with 272 (78.6%) having current first aid certificates (98 owners/managers, 174 other pharmacists). Most pharmacies (90.7%) already had consultation areas and the majority of these areas were suitable for vaccination services (89.7%). Overall 93.0% provided MedsCheck (in-pharmacy medication review) services and 90.7% provided Diabetes MedsCheck services. Forty-two of the 86 pharmacies (48.8%) provided vaccination services in the previous 12 months, delivered by another healthcare professional (nurse or nurse practitioner). These health professionals provided ∼4023 vaccinations (2–400 per pharmacy) over the previous 12-month period.
Using a five-point Likert scale, 72.1% either agreed or strongly agreed that their relationship with local general practices extended beyond sorting out dispensing issues. However, only 29.1% indicated that they regularly met to discuss patient care issues.
The main reasons for providing pharmacist vaccination services were identified using a five-point Likert-scale (table 2). All pharmacies either strongly agreed or agreed that it was to provide health promotion opportunities and to enhance the role of pharmacists, 96.5% indicated that it was to increase consumer immunisation rates, 90.7% that it was to provide holistic patient care opportunities and 89.5% for professional satisfaction of pharmacists. The lowest score was 66.3% which was for financial gain. Many participants (72.3%) indicated that they would either all of the time or most of the time offer the service through an appointment system during specific pharmacy trading hours, 57.0% indicated that they would manage through walk-in without appointments and only 27.3% would use an appointment system during all pharmacy trading hours.
Reasons for providing pharmacist vaccination services and planned future services
Pharmacy exit survey
Of the 86 pharmacies that completed baseline surveys, 78 (90.7%) completed exit surveys. A total number of 15 621 influenza vaccinations were provided during the 2015 influenza season by 76 of the pharmacies (2 pharmacies did not provide services). Of these, 1855 (11.9%) were delivered to consumers who were eligible to receive influenza vaccinations under the NIP but chose to have it at the pharmacy. A total of 379 consumers (2.4%) were deemed not suitable for pharmacist vaccinations and were referred to a medical practitioner. Overall, 119 (0.76%) consumers experienced a mild local reaction and 19 (0.12%) experienced a mild systemic reaction (eg, headache) within 15 min postvaccination. None of the consumers experienced a severe reaction and none required the use of epinephrine.
Almost all of the pharmacist participants (98.7%; n=77/78) either strongly agreed or agreed that they intended to continue providing influenza vaccinations in 2016 and 97.4% (n=76/78) indicated it appropriate to expand the service to other vaccinations (table 2).
Overall, 32.1% (n=25/78) of participants strongly agreed or agreed that it improved relationships with other local area health professionals and 26.9% (n=21/78) either strongly agreed or agreed that they experienced support from the local general practices.
Regional shopping centre pharmacies, on average, provided the highest number of vaccinations compared with other pharmacy types (table 1). This may be related to the higher proportion of immuniser pharmacists available in the regional areas.
Pharmacy computer records
Of the participating pharmacies, 57 used a software program called GuildCare42 to record the vaccination services provided. The other pharmacies used paper-based systems or alternative software and their computer records were not available for analysis. The GuildCare data were extracted from the GuildLink Tableau platform.
The 57 pharmacies provided a total of 5588 pharmacist vaccination services during January to September 2015. The peak period was mid-25 April with a second peak during 3–9 May 2015. In terms of time of day when the vaccination services were provided, 11:00–12:00 was the most popular followed by 10:00–11:00. Overall, most of the services were provided during afternoons. A total of 264 services were provided between 18:00 and 23:00. The majority of consumers were 50 years and older (56.8%; n=2914/5126) with 50.6% between 50 and 65 years old. A total of 932 consumers (16.7%) were identified as qualifying under the NIP. Most of them (91.0%; n=848/932) were aged 65 years and over and some (7.1%; n=66/932) had a chronic illness, were pregnant (1.4%; n=13/932) or were classified as Aboriginal and Torres Strait Islanders (ATSIs; 0.5%; n=5/932).
A cross-match of pharmacy postcodes with the postcodes of consumers that were vaccinated showed that the majority of patients lived in the postcode where the pharmacy was located. Pharmacist vaccination services were spread over a wide geographical area. Of specific interest was the high percentages of vaccinations delivered in a regional (Kalgoorlie, PhARIA category 3) and rural area (Esperance, PhARIA category 5; 23.1%; n=1010/4376).
Pharmacist exit interviews
Of the 25 pharmacists who were interviewed, 10 were males and 15 were females. Saturation of data occurred after ∼15 interviews; however, the process continued to ensure representation from a range of pharmacies.
The median number of vaccinations given per pharmacy was 84 (range 5–1252, total vaccinations by 25 participants=5391). Service charges (inclusive of vaccine) ranged between $19.95 and $30.00 for the trivalent vaccines and between $30.00 and $39.95 for the quadrivalent vaccines. Charges for some consumers were partially or fully subsidised by a private health insurance company. The demand for vaccination services was reported to exceed pharmacists' expectations:We had quite a very big demand on it. People, as soon as they heard about, [that] they could do it in the pharmacy, no appointment, no script required—we had a great response from consumers. (P139)
Adverse events reported by the pharmacists included mild local injection site reactions, light headedness, fainting and slight fever several days postvaccination. In all of these cases, pharmacists appeared to be well informed of the possible adverse effects of the vaccine, and protocols were in place and followed when managing these situations, which included appropriate consumer follow-up.
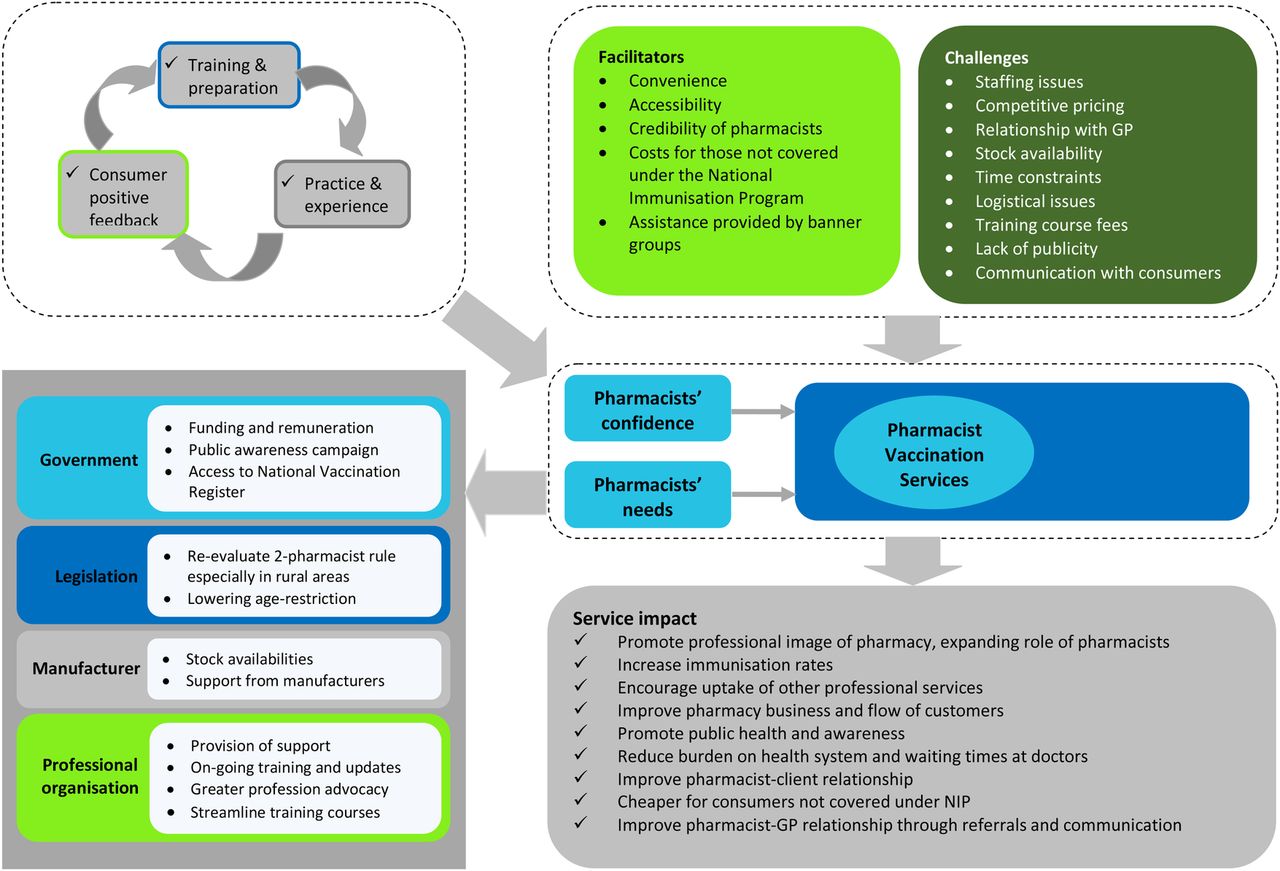
Six main themes emerged through the thematic analysis of the interview data (figure 1):
Facilitators,
Challenges,
Pharmacists' needs,
Pharmacists' confidence,
Community pharmacists' role,
Positive service impact.

Schematic representations of the relationships between interview themes. GP, general practitioner; NIP, National Immunisation Program.
Facilitators and challenges
Table 3 provides selected quotations related to facilitators and challenges. Convenience and accessibility of community pharmacies were identified as major factors facilitating the demand and uptake of vaccination services by consumers. Pharmacists believed that offering the service via both appointment-booking and walk-in (no waiting time) systems provided convenience and flexibility to the consumers and encouraged uptake of the service. It was also reported that some consumers who would qualify under the NIP for free vaccinations were willing to pay for the vaccination service in the pharmacy due to convenience. Participants who did not qualify under the NIP mentioned that being vaccinated at the pharmacy was preferential to be vaccinated at their general practitioner (GP) because, as consumers, they saved time and GP fees. Credibility of pharmacists and pharmacist–client relationships were identified as important facilitators as some pharmacists had longstanding relationships with consumers.
Facilitators and challenges to provision of pharmacist vaccination services
Challenges experienced included workforce issues, fear of jeopardising relationships with GPs, competitive pricing, unavailability of stock, pharmacy physical layout issues, training fees and promotion of the service to consumers.
Pharmacists' needs
Several needs were identified as participants described what was considered necessary to ensure efficiency and improvement of pharmacist vaccination services. These included a government funding model or government subsidy of pharmacist vaccination services (such as adding pharmacists as NIP providers with remuneration for service provision) and entry and access to the National Vaccination Register. Participants also expressed a need for the re-evaluation of the requirement for two pharmacists to be at the pharmacy, specifically in rural areas. Support from manufacturers and professional organisations were also highlighted.
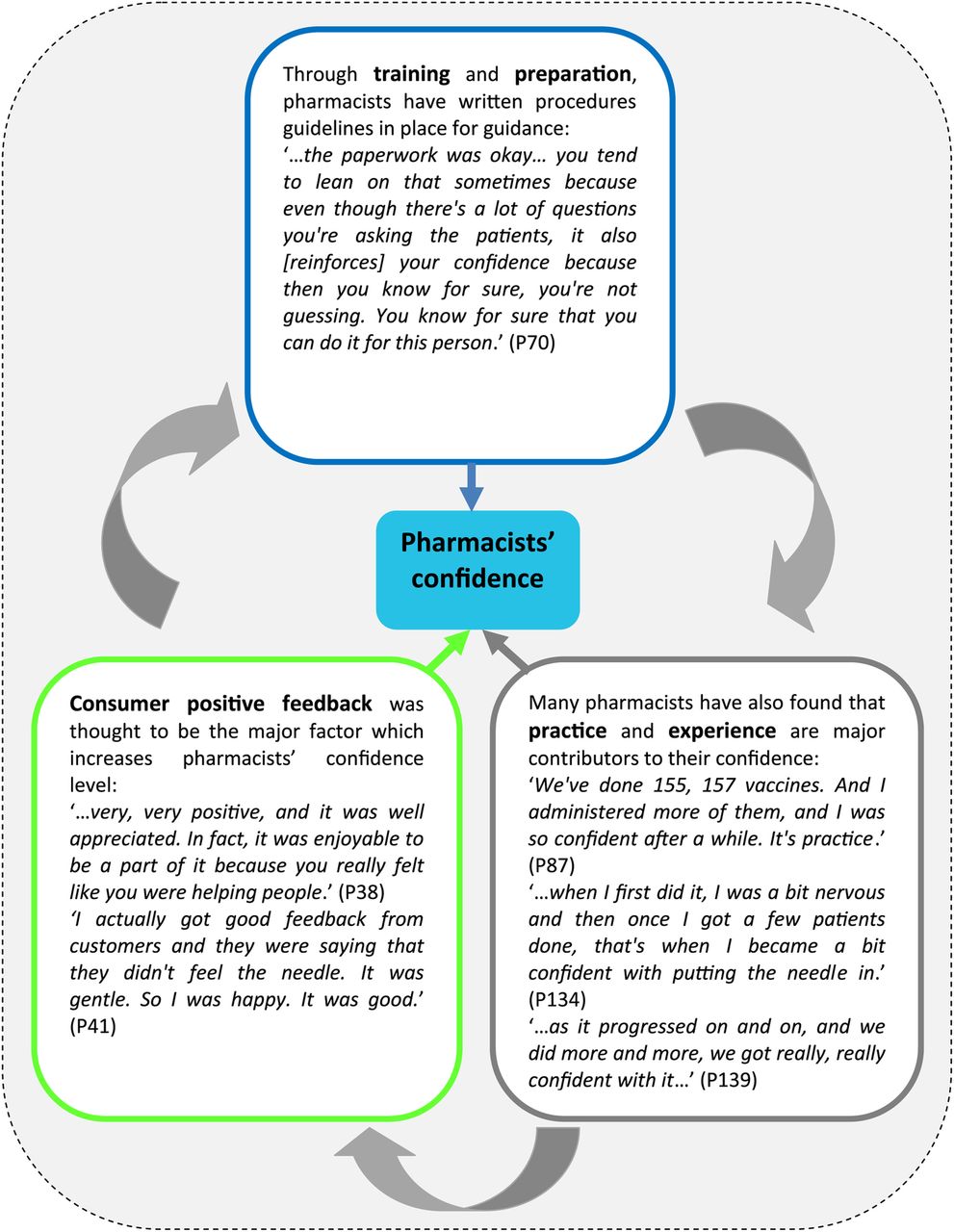
Pharmacists' confidence
Overall, the immuniser pharmacists were confident in providing vaccination services. Positive feedback from consumers, practice and experience in administering vaccines, and the presence of procedures and guidelines were identified as three major factors that affected confidence levels (figure 2 with selected quotations).
{kind=link}
{kind=link}
Factors affecting pharmacists’ confidence levels.
Community pharmacists' role
Pharmacists were perceived as convenient, easily accessible and credible health professionals who are well placed to provide vaccination services. Pharmacists were also perceived as an alternative vaccination service provider to GPs, especially for those consumers not covered the NIP. The willingness of pharmacists in becoming immunisers and their support of service expansion were apparent, as described by one participant: “We’re just hoping it can be expanded and continued in the future” (P29). Despite being an advocate for professional service expansion, participants of this study appeared to be aware of their strengths and limitations, and were conversant with the relevant guidelines and regulations.
All 25 participants agreed that pharmacist vaccination services should be expanded to other vaccinations. In addition to influenza vaccination, other vaccinations suggested included pertussis, tetanus, measles, mumps and rubella, hepatitis A and B, pneumococcal, typhoid and travel vaccines.
Positive service impact
The impact of vaccination services on the professional image of pharmacy was paramount and extended beyond the context of immunisation services. In addition to promoting the professional image of pharmacies and pharmacists, it was evident that the provision of vaccination services encouraged the uptake of other professional services in the pharmacy:…they see a pharmacy more as a health provider and it gives that extra boost of health providing rather than just drugs and medication…it gives pharmacy a bigger scope of practice in terms of health care and health management…talk to them about the other services that a pharmacy provides…they were all quite shocked [surprised] that pharmacies do blood pressure readings and stuff like that. I think it is an opportunity to talk about their health matters with the patients…(P75)
In the context of convenience and accessibility, it was identified that by offering the service through community pharmacies, pharmacists could contribute towards increasing the immunisation rates especially among those not covered under the NIP: “They’re usually the ones that don’t hold the appointments with the doctors, that aren’t going to go to the doctors, and really are often quite time poor” (P18). Increasing the vaccination rates may also lead to other positive impacts, such as herd immunity and public health promotion: “…it just helps to protect the community in terms of herd immunity and so forth” (P48).
Participants stated that pharmacist vaccination services could help reduce the burden on the Australian health system and reduce GPs waiting times: “you’re reducing doctors' time; you’re reducing probably the expense and the workload on to the PBS [Pharmaceutical Benefits Scheme]…” (P85). Furthermore, referral of consumers covered under the NIP to GPs encourages communication between pharmacists and GPs, which enhances pharmacist–GP relationships and promotes interprofessional collaboration.
Discussion
In total, 15 621 influenza vaccinations were administered at 78 WA community pharmacies by immuniser pharmacists between March and October 2015. There were no major adverse events, and <1% of consumers experienced minor events which were appropriately managed within the pharmacies. Between 12% and 17% of consumers were eligible to receive free influenza vaccinations under the NIP but chose to have it at a pharmacy. Of specific interest was the high percentage of vaccinations delivered in rural and regional areas indicating that provision of pharmacist vaccination services facilitates access to rural and remote consumers. Immuniser pharmacists reported feeling confident in providing vaccination services and were of the opinion that pharmacist vaccination services should be expanded to other vaccinations. Pharmacists also reported significant professional satisfaction in providing the service. All participants intended to continue providing influenza vaccinations in 2016.
Convenience and accessibility were important aspects in usage of services and the majority of consumers lived in the postcode where the pharmacy was located. Recent Australian research reinforced convenience as the leading factor influencing consumers' choice of pharmacy services.43 Convenience and accessibility were similarly highlighted as important considerations in initial US pharmacist vaccination service findings.9 These results are also consistent to two recent Canadian studies that indicated convenience was a main advantage to being vaccinated at a pharmacy.17 ,44 Providing easy access through appointment or walk-in vaccinations gave consumers flexibility in accessing immunisation services. International research has also shown that specific consumer groups (ie, younger, working-aged, healthy adults) prefer after-hours services45 when traditional vaccination providers are likely to be unavailable and hence community pharmacy vaccination services could attract these groups.
According to the Global Vaccine Action Plan 2011–2020,46 countries are encouraged to set national immunisation targets and have strategies in place to meet these targets. In some parts of Australia, specifically in WA, overall immunisation rates are below the national immunisation coverage target of 95% and are considered lower than in other Australian jurisdictions.47 ,48 Some studies conducted overseas have shown increased immunisation rates in the community with the addition of pharmacists as immunisation providers through the provision of vaccination services.44 ,49 However, a recent evaluation of London vaccination data showed no evidence of increased influenza vaccination uptake resulting for a pharmacy initiative allowing the administration of influenza vaccinations in pharmacies50 whereas the 2014 Canadian study showed marginal increases.17 The ongoing evaluation of the potential impact of changes to legislation to enable pharmacists, and other health professionals such as nurse practitioners to be able to administer vaccinations is therefore important in informing policy.
As stated in the WA Immunisation Strategy 2013–2015,48 “WA has the lowest GP-to-population ratio in the nation. Optimising the use of nurses and other trained health care workers is, therefore, critical to WA's efforts to expand and improve immunisation service delivery.” With an increased number of trained immuniser pharmacists and a concerted advertising programme to raise community awareness, pharmacists could contribute towards meeting the goal and aims of this strategy, ultimately achieving an improved immunisation rate.
The majority of exit survey participants commented that pharmacist vaccinations should be expanded to people <18 years old. A 2012 US study of 86 parents showed they felt confident about a pharmacist providing influenza vaccinations to their children.51 The Australian Influenza Surveillance Report highlighted that children <15 years old accounted for one-third of all influenza notifications.52 Expanding the scope to include younger children therefore requires consideration as allowing pharmacists to immunise children will assist with reducing the number of influenza infections in this age group.
Availability of pharmacist vaccination services facilitated access to rural and remote consumers, similar to findings from international studies.53–55 An area that should be explored is provision of pharmacist vaccination services to specific deprived groups such as ATSI people. An US study of pharmacist vaccination services provided to deprived communities showed a significant impact on increasing adult immunisation rates in these communities.56 However, the requirement for two pharmacists may limit service provision in these areas and some interview participants commented that it was challenging to have two pharmacists on board in rural/regional pharmacies. This requirement should be reconsidered by legislative authorities as such restrictions are not required with such a low-risk procedure.
In addition to influenza vaccination, other vaccinations the participants indicated that could be administered by pharmacists included pertussis, tetanus, measles, mumps and rubella, hepatitis A and B, pneumococcal, typhoid and travel vaccines in general. Various of these vaccinations are already included as pharmacists'-administered vaccinations in the USA,15 ,57–59 UK20 ,21 and NZ.24 Consideration should be given to broadening the types of vaccinations available particularly of those vaccines that have consistently low rates of community uptake such as HPV,60 and in areas of low vaccination such as in ATSI communities.61
Provision of pharmacist vaccination services created opportunities to establish therapeutic relationships. This facilitated holistic patient-centred care which fits the Government's approach towards funding for the provision of professional services.62 Pharmacists are well placed to ensure good communication between healthcare providers and maintain good surveillance and immunisation registration quality. However, interview participants commented that appropriate funding should be considered, a finding that is similar to recently published US research that identified inconsistent reimbursement as a challenge for pharmacists that need to be addressed.49 From the perspective of healthcare resource allocation in Australia, pharmacist-delivered vaccinations saves money for the government as pharmacists are not paid a consultation fee through Medicare, as is the case with other health professionals, that is, GPs. However, for the service to be sustainable government funding to pharmacists needs to be considered.
Strengths and weaknesses
This is the first study that comprehensively evaluated the implementation of pharmacist vaccination services in Australia and explored the uptake of the services from pharmacists' perspectives. The study involved mixed methodology with both quantitative and qualitative data through surveys, pharmacy computer records and interviews. The various data sources enabled contextualising and triangulation of information and hence enriched the exploration of the research topic.63 However, this study had limitations as the research involved voluntary self-administered baseline and exit surveys to pharmacists who chose to provide pharmacist vaccination services. These pharmacists potentially were biased in their responses. The interview participants involved purposive sampling of immuniser pharmacists who indicated their willingness to be interviewed. Although there is a likelihood of bias, it was considered important to interview participants who had experience in the delivery of vaccination services. Also, this study was conducted in WA and findings might differ in other Australian jurisdictions due to slight differences in legislative provisions.
Conclusion
This initial evaluation of WA pharmacist vaccination services showed that vaccine delivery was safe. Convenience and accessibility were important aspects in service usage. There is scope to expand pharmacist vaccination services to other vaccines and younger children; however, government funding to pharmacists needs to be considered. Greater numbers or immunisation rates could be achieved with an increased number of trained pharmacists, appropriate funding and a concerted advertising programme to raise community awareness.
Acknowledgments
The authors thank the participants for their time. The authors also thank Matt Tweedie and Denise Crockford from the Pharmacy Guild of Australia (WA Branch) and Stefanie Johnston from the Pharmaceutical Society of Australia (WA Branch) for assistance with recruitment, their time and expertise.
References
Footnotes
Contributors HLH, PC and AV devised the study and its methodology. HLH, PC and AV created the surveys and interview tool and sought ethics approvals. SA and RP did quantitative data analysis and SA conducted the interviews, TFS did the qualitative analysis, HLH managed the overall project. All authors had access to the data, contributed to all drafts of the paper and approved the final copy for publication. All authors state that they had complete access to the study data that support the publication.
Funding This work was supported by funding from the Western Australia Department of Health.
Competing interests None declared.
Ethics approval The study received Human Research Ethics Committee approvals from Curtin University and The University of Western Australia (RDHS-58–15 and RA/4/1/7510).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.tb084