Article Text

Abstract
Objective This study systematically reviewed the effect of melatonin (MLT) on quality of life (QoL) and symptoms among patients with cancer.
Design Systematic review and meta-analysis.
Data sources Cochrane Library, PubMed, Embase, Web of Science, Medline, CINAHL, Scopus, ClinicalTrials.gov, China Biology Medicine (CBM), ProQuest and Open Grey were searched from inception to November 2021.
Eligibility criteria We included randomised controlled trials (RCTs) assessing the effects of MLT on QoL, sleep quality, fatigue, depression, pain, stomatitis rate and stomatitis severity in adult patients with cancer, without language restrictions. Studies that reported the effects of MLT along with other interventions and had incomplete or absent outcome data were excluded.
Data extraction and synthesis Two independent reviewers extracted data, and another two reviewers assessed the risk of bias. The risk of bias for each eligible study was assessed using the Cochrane assessment tool. The mean difference or standard mean difference (SMD) with 95% CIs was used in the computation of continuous variables to synthesise data. The relative risk was used for dichotomous outcomes. Heterogeneity was assessed and quantified (I2 statistic).
Results A total of 19 qualified studies that included 2101 patients with cancer (MLT: 1078, control: 1023) were included in the meta-analysis. The results indicated that MLT had no significant effect on QoL (SMD=−0.01, 95% CI (−0.14 to 0.11), p=0.83), sleep quality (SMD=−0.18, 95% CI (−0.62 to 0.26), p=0.42), fatigue (SMD=−0.34, 95% CI (−0.73 to 0.06), p=0.10), pain (SMD=−0.34, 95% CI (−0.7 to 0.02), p=0.06) or stomatitis severity (RR=0.78, 95% CI (0.47 to 1.30), p=0.35). MLT reduced stomatitis rate among patients with cancer (RR=0.47, 95% CI (0.26 to 0.88), p=0.02), except those with head and neck cancer (RR=1.09, 95% CI (0.92 to 1.29), p=0.35). MLT eased depression in patients who received administration for more than 14 days (SMD=−0.14, 95% CI (−0.27 to –0.01), p=0.03) and those who underwent surgery (SMD=−0.17, 95% CI (−0.32 to –0.03), p=0.02).
Conclusion The findings showed that MLT did not improve the QoL, sleep quality, fatigue, pain or stomatitis severity among patients with cancer. It had a limited effect on decreasing the stomatitis rate and easing depression. Different treatments, durations and cancer types were the main sources of heterogeneity. Further large-scale RCTs are urgently needed. In addition, the effects of different combinations of MLT dosage and duration, administration types and joint measures are worthy of further study.
PROSPERO registration number CRD42021292855.
- adult oncology
- pharmacology
- clinical pharmacology
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A strict search strategy was used in multiple databases.
Most of the studies were of high quality with a low risk of bias, which could further lend confidence to the current pooled results.
We widely explored the effectiveness of melatonin (MLT) in different populations, treatments, dosages and durations in subgroup analysis.
For every dimension of MLT, including quality of life, sleep, fatigue, depression, pain and stomatitis, the literature is limited, which limits the generality of the conclusion.
The main significant results were from subgroup analysis of the limited studies, and the results should be interpreted prudently.
Introduction
Melatonin (MLT) is an important endogenous indolamine that is synthesised and secreted into the systemic circulation and cerebrospinal fluid by the pineal gland and has recognised antiaging, anti-inflammatory and antioxidant properties.1 As a strong antifibrotic agent,2 MLT can be used as a desired preconditioning agent in cell-based therapy.3 4 It also has a substantial role in regulating the circadian rhythm and sleep during the night.5 6 Recent studies have proven the effect of MLT on limiting skeletal muscle frailty, prolonging physical performance7 and preventing bone loss.8 In the oncology field, MLT has significantly apoptotic, angiogenic, oncostatic and antiproliferative effects on various oncological cells.9 It was proven that low levels of MLT might be a risk factor for breast cancer.10 Meanwhile, MLT coadministration improves the sensitivity of cancers to inhibition by conventional drugs and reduces the toxic consequences of anticancer drugs while increasing their efficacy.11 There is major concern about the symptoms induced by cancer and cancer treatment that patients encounter, including physical symptoms and psychological/spiritual distress,12 leading to decreased quality of life (QoL). Equally, MLT plays an important role in enhancing QoL by improving survival and decreasing symptoms.13 The positive association between MLT and various health outcomes in patients with cancer has been shown in some studies.14 A recent meta-analysis revealed that MLT may benefit patients with cancer by improving survival and ameliorating the side effects of chemotherapy.15 Palmer et al showed the neuroprotective effect of MLT to counteract the adverse effects of chemotherapy on cognitive function, sleep quality and depressive symptoms in patients with breast cancer.16 A recent clinical trial concluded that MLT supply decreased the levels of fatigue in patients with breast cancer.17 However, some of the recent published findings suggest conflicting results18 19 that MLT intervention cannot improve the QoL, reduce the symptom burden or present the uncertain results.20 We are not aware of any systematic reviews and meta-analyses that have synthesised the evidence of the function of MLT in patients with cancer. The effect of MLT on health outcomes in the cancer group mains nonspecific and ambiguous. Thus, with accumulating evidence, we performed a systematic review and meta-analysis of randomised controlled trials (RCTs) to investigate the roles of MLT in improving QoL and symptoms in patients with cancer.
Materials and methods
Search strategy
A thorough search was conducted in the Cochrane Library, PubMed, Embase, Web of Science, Medline, CINAHL, Scopus, ClinicalTrials.gov and China Biology Medicine (CBM) from inception to November 2021 for RCTs without language restrictions. Sources of unpublished studies and grey literature were searched through ProQuest and Open Grey. We used medical subject headings and text words to search the studies. The search strategies are provided in online supplemental file 1.
Supplemental material
Eligibility criteria
Participants
Studies including adult patients (≥18 years) who were diagnosed with cancer according to National Cancer Institute codes, regardless of cancer type, cancer stage (early, middle or advanced) and current treatment (such as radiation therapy, chemotherapy, surgery, targeted therapy, immunotherapy, combination of any of the above treatments or without any treatment), were eligible.
Interventions and controls
All trials that reported and evaluated the effects of MLT were included. Literature were excluded if they met the following criteria: (1) they were not RCTs; (2) studied the effects of MLT along with other interventions and (3) incomplete or absent outcome data.
Outcomes
The primary outcome was QoL. The scores of sleep quality, fatigue, depression and pain, stomatitis rate and stomatitis severity were the secondary outcomes.
Studies
Only RCTs were eligible.
Data extraction
Two independent researchers (SY, TW) extracted the data of eligible studies and performed double-checks. Any disagreements and differences were resolved by a third investigator (XB). The following data from the full text of selected studies were extracted: first author’s name, year of publication, the characteristics of the patients, the characteristics of the intervention and the control groups (study design, form of intervention, dose of MLT supplementation, duration), number of participants in each group and outcome data (means and SD for continuous data; number of incidents for dichotomous data).
Risk of bias assessment
Two reviewers (YT, HC) independently evaluated the risk of bias for each eligible study using the Cochrane assessment tool, which consists of the following seven domains: ‘random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other bias’. Each question can be rated as follows: yes (+), low risk of bias; unclear (?), unclear risk of bias; no (−), high risk of bias. Any disagreement between the reviewers was resolved by discussion until consensus was reached.
Data analysis
The meta-analysis was performed using Review Manager Software (V.5.3). The scores of QoL and symptoms was estimated by the mean difference (MD) when trials measured an outcome using the same measurement method or scale. We used the standard MD (SMD) when different instruments were used to measure the same outcome. For dichotomous outcomes (such as stomatitis rate and stomatitis severity), we used relative risk (RR). The effect size (ES) and the 95% CI were computed. ESs with scores of 0.2–0.5, 0.5–0.8 and >0.8 were considered as small, medium and large effects, respectively. Forest plots were used to display the pooled ES, 95% CI, weight in percentage. If variability was presented by measures other than the mean or SD, we used standard approaches for estimating data. If the studies did not report SD, we used the following formula to calculate missing SD: SD=√N×(upper 95% CI-lower 95% CI)/3.92. If a study provided medians and IQRs, we transformed the median and IQR to the mean and SD by a method for nonnormal data.21 I2 was used to measure the statistical heterogeneity among the trials in each analysis. If p>0.1 and I2 <50%, a fixed-effects model was adopted; if p<0.1 and I2 ≥50%, then a random-effects model was adopted. If heterogeneity was identified, subgroup analyses were conducted on different cancer types, treatments, dosages and durations. Sensitivity analysis was performed by removing studies with a high or unclear risk of bias. Reporting and publication bias were investigated by visually examining the degree of asymmetry of a funnel plot.
Patient and public involvement
No patients were involved.
Results
Literature search
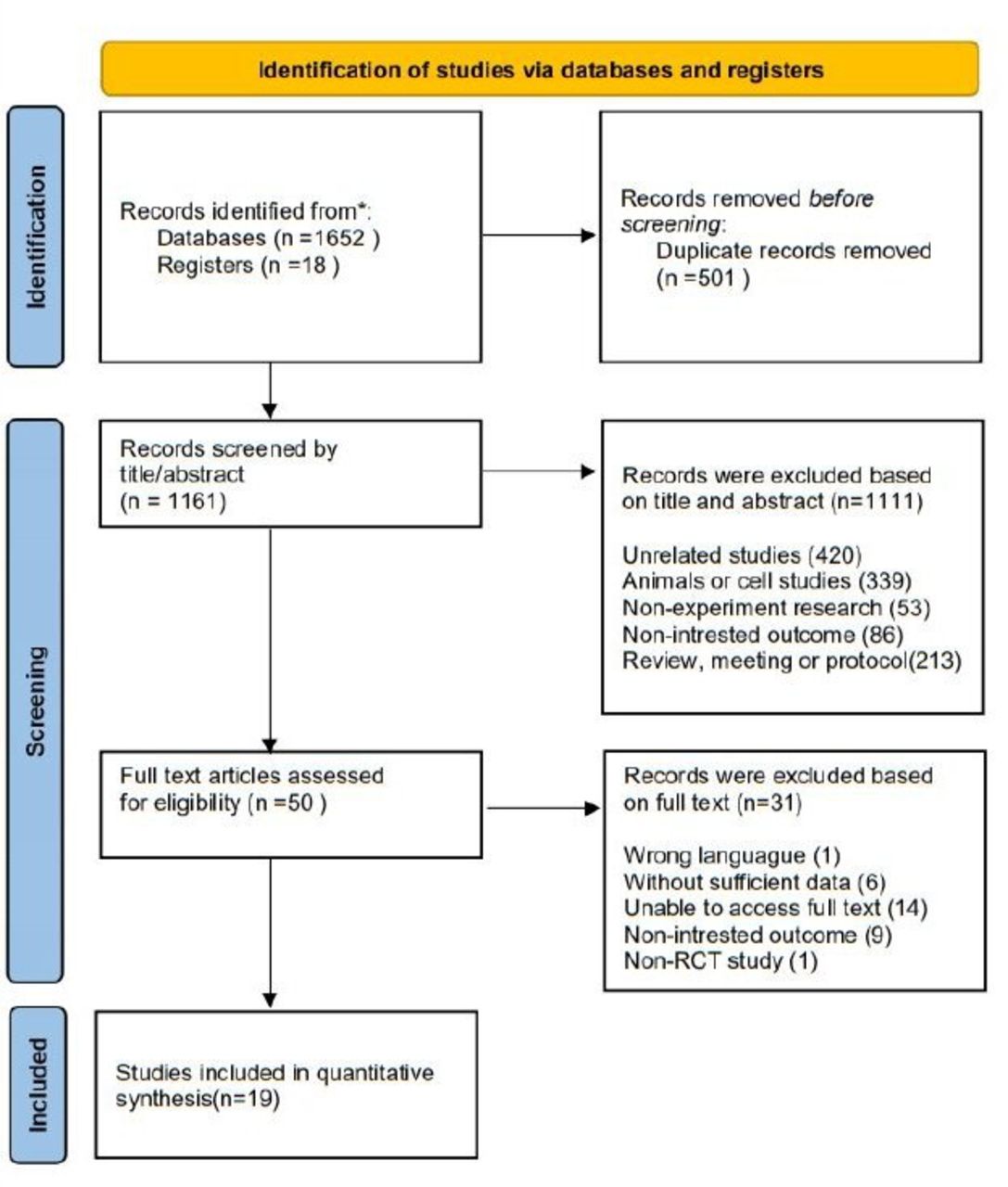
The initial search identified 1670 publications through PubMed, Embase, Medline, Scopus, SinoMed, Web of Science, Cochrane and Clinical Trials. After excluding 501 duplicates, a total of 1161 studies were retrieved for title and abstract screening. After screening the titles and abstracts, 1111 articles were excluded, and 50 papers were retrieved for full text review. Out of 50 retrieved papers, 1 article was excluded due to wrong languages,22 6 articles were excluded without complete data, 14 articles were excluded without full text, 9 articles were excluded without target outcome and 1 article was excluded due to a non-RCT study.23 Therefore, a total of 19 articles were included in the final meta-analysis.24–42 The flow chart of the literature search is shown in figure 1.

Study flow diagram. RCT, randomised controlled trial. *The number of records identified from each database and register searched were: pubmed (16), embase (38),medline (289), scopus (508), sinomed (21), web of science (633), cochrane (136), clinical trial (18).
Quality assessment
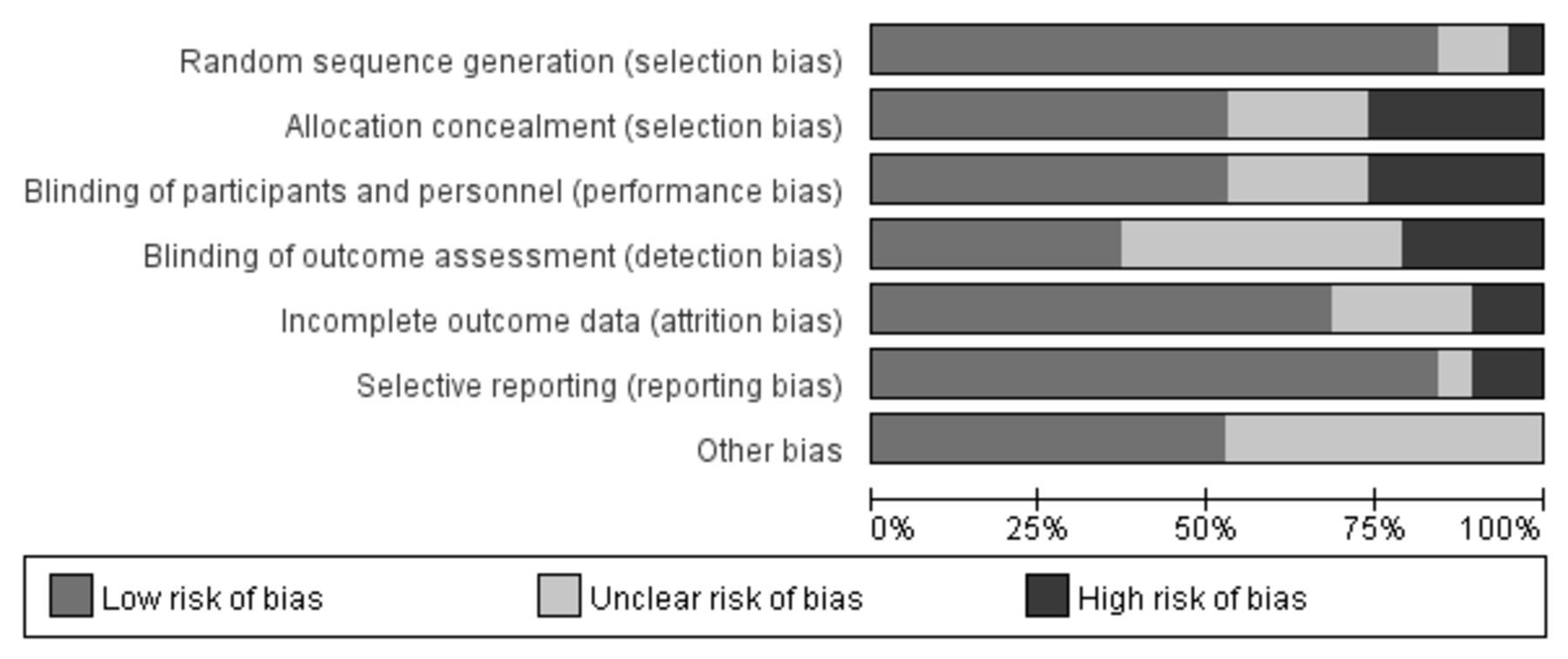
We used the Cochrane scoring system to assess the quality of the included studies. Two reviewers had different opinions on bias in one article in ‘incomplete outcome data’, and one article in ‘selective reporting’. Through the discussion, final consensus was achieved. The overall risk of bias as shown was moderate (figure 2). Nearly all studies reported appropriate random sequence generation. Most studies reported completed data and had low risk of bias on the item ‘selective reporting’. Almost one-third of the studies did not report blindness in the outcome assessment. The individual risk of bias for each study is presented in figure 3.
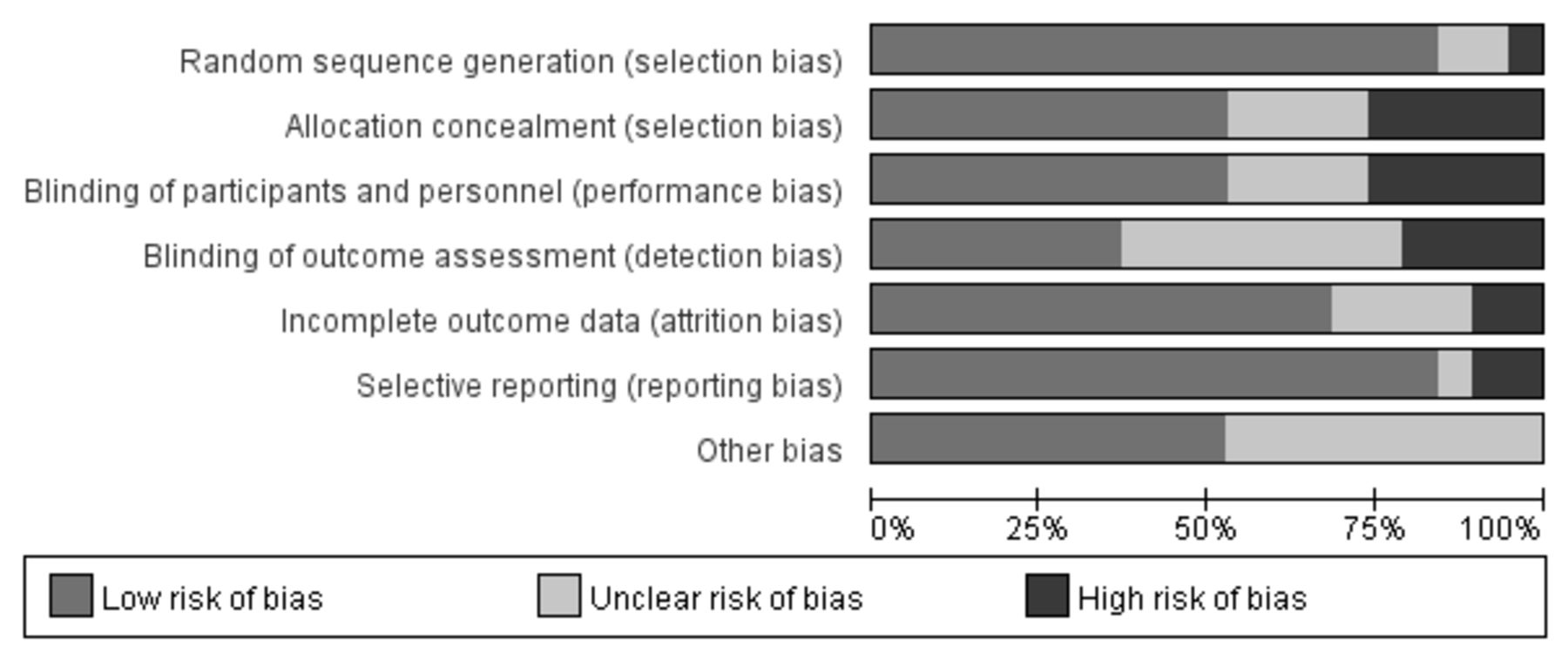
The overall risk of bias.

The individual risk of bias for each study.
Literature characteristics
The characteristics of the patients, interventions, controls and measures are shown in table 1.
The characteristics of the literature
Participants
The publication dates ranged from 1997 to 2021. Among the 19 studies included in the systematic review, the mean age of the participants ranged from 46.05 to 67.2. The sample size ranged from 14 to 709 participants. Regarding treatment trajectory, 12 studies were conducted in patients with cancer with adjuvant chemotherapy and/or radiotherapy,25 26 29–32 35–38 40 41 1 was in patients with advanced cancer with fatigue,33 1 was in breast cancer survivors,24 3 were in patients with cancer with surgery,27 34 39 and 2 were in patients with advanced cancer with poor sleep quality.28 42 Regarding cancer diagnosis, six studies were in breast cancer,24 27 34 36–38 two were in non-small-cell lung cancer,26 39 three were in head and neck cancer,25 32 35 one was in colorectal cancer40 and seven studies were not restricted to cancer type but were mostly in patients with advanced cancer.28–31 33 41 42
Intervention
The follow-up period ranged from 7 days to 1 year. The MLT dosage varied between 3 and 20 mg. Regarding the types of MLT administration, 17 involved oral MLT,24–31 33 34 36–42 1 involved MLT oral gargle32 and 1 was combined.35 Nearly all studies gave the MLT at night, except one which compared dosage given both in the morning and at night.26
Instruments
All studies used standardised and validated tools. QoL was measured by four validated tools: the European Organisation for Cancer Research,26 37 Treatment validated for the Brazilian population (QLQ-BR 23),37 Functional Assessment of Cancer Therapy,41 42 Ferrans and Powers Quality of Life Index,26 European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative Version (EORTC QLQ-C15-PAL)33 and Lung Cancer-13.39 Sleep quality was measured by the Pittsburgh Sleep Quality Index,24 26 36 37 40 42 Visual Analogue Scale (VAS),27 34 Karolinska Sleepiness Scale,27 34 Sleep Quality Scale,40 Athens insomnia scale28 and Medical Outcomes Study Sleep Survey.39 Depression was measured by the Beck Depression Inventory,37 39 Beck Depression Inventory,36 Center for Epidemiologic Studies-Depressio,24 Major Depression Inventory,27 Hamilton Rating Scale for Depression,40 Hospital Anxiety and Depression Scale.42 Fatigue was measured by the Multidimensional Fatigue Inventory,33 EORTC QLQ-C15-PAL (fatigue domain),33 Brief Fatigue Inventory,38 VAS,27 Multidimensional Fatigue Index 20 questionnaire,39 QLQ-C30 (fatigue domain)26 and Functional Assessment of Cancer Illness Therapy-Fatigue subscale.42 Pain was measured by VAS,27 34 Brief Pain Inventory,39 QLQ-C30 (pain domain)26 and Numeric Rating Scales.25 36 The incidence of stomatitis was calculated by the ratio of the occurrence number to the total number.25 29–32 35 41
Meta-analysis
Effect of MLT on QoL
Overall, six clinical trials evaluated the effect of MLT on QOL. The results showed that there was no statistically significant difference between the intervention and control groups (SMD=−0.01, 95% CI (−0.14 to 0.11), p=0.83) with no heterogeneity (I2=0%, p=0.42) (figure 4). All six studies used a 20 mg MLT dosage. Subgroup analysis based on study durations (p=0.65–0.92) and treatment types(p=0.45–0.6) showed no significant differences.

Forest plot of the effect of MLT on QoL among patients with cancer. MLT, melatonin; QoL, quality of life.
Effect of MLT on sleep quality
Nine clinical trials evaluated the effect of MLT on sleep quality. Pooled ES from the random effect model showed that there was no significant effect on sleep quality (SMD=−0.18, 95% CI (−0.62 to 0.26), p=0.42) (figure 5). There was significant heterogeneity between studies (I2=87%, p<0.001). We deleted a study40 with obvious heterogeneity and I2 decreased to 79% (SMD=−0.35, 95% CI (−0.73 to 0.03), p=0.07). Subgroup analysis based on dosage, study durations, treatments, different combinations of dosage and duration showed no significant differences between subgroups (table 2).
Subgroup analyses of melatonin supplementation on sleep quality

Forest plot of the effect of MLT on sleep quality among patients with cancer. MLT, melatonin.
Effect of MLT on fatigue
The overall ES of MLT for fatigue alleviation was medium (SMD=−0.34, 95% CI (−0.73 to 0.06), p=0.10) with high heterogeneity (p=0.002, I2=74%). However, there was no significant difference. The study of Sedighi Pashaki et al38 showed great heterogeneity because only this one proved a significantly lower level of fatigue in the intervention group. We removed it, and the heterogeneity decreased to 0% (figure 6).

Forest plot of the effect of MLT on fatigue among patients with cancer. MLT, melatonin.
Effect of MLT on depression
Six clinical trials evaluated the effect of MLT on depression. Only Palmer et al showed a significant effect on depression.37 The overall treatment effect on depression showed that there was no statistically significant difference between the intervention and control groups (SMD=−0.24, 95% CI (−0.53 to 0.05), p=0.10) with high heterogeneity (p=0.03, I2=60%). A sensitivity analysis was performed by removing one study from the analysis (figure 7).37 Regarding subgroup analysis, a significant difference was observed for different study durations and treatments, although both showed a slight ES. Patients who received an intervention duration greater than 14 days had significantly lower depression (SMD=−0.14, 95% CI (−0.27 to –0.01), p=0.03) with low heterogeneity (p=0.4, I2=0%) (figure 8). Meanwhile, MLT alleviated depression in patients with cancer who underwent surgery (SMD=−0.17, 95% CI (−0.32 to –0.03), p=0.02) with low heterogeneity (p=0.35, I2=0%) compared with those received chemotherapy (figure 9). No significant difference was observed among studies on the different dosages (p=0.27–0.43), cancer diagnosis (p=0.20) and combined chemotherapy (p=0.13–0.42).

Forest plot of the effect of MLT on depression among patients with cancer. MLT, melatonin.

Forest plot of longer MLT duration on depression among patients with cancer. MLT, melatonin.

Forest plot of MLT on depression among patients with cancer underwent surgery. MLT, melatonin.
Effect of MLT on pain
Five clinical trials evaluated the effect of MLT on pain (SMD=−0.34, 95% CI (−0.7 to 0.02), p=0.06) with high heterogeneity among studies (p=0.03, I2=62%). No significant difference was observed among studies on the cancer diagnosis (p=0.27–0.47), combined treatments (p=0.37), durations (p=0.11) and dosages (p=0.16–0.27). Sensitivity analysis was performed by removing one study,25 and the heterogeneity decreased to 0% (figure 10).

Forest plot of the effect of MLT on pain among patients with cancer. MLT, melatonin.
Effect of MLT on stomatitis
Regarding stomatitis, seven clinical trials evaluated the effect of MLT on the incidence of stomatitis. The finding showed that there was no significant ES (RR=0.71, 95% CI (0.45 to 1.13), p=0.15) (figure 11), with high heterogeneity (p<0.001, I2=86%). All of the study durations were more than 2 weeks, and all patients accepted chemotherapy or radiotherapy. In addition, nearly all these clinical trials gave an MLT of 20 mg, except one that used a 3% MLT oral gel.32 However, removing it or not caused little change to heterogeneity and ES. Further subgroup analysis showed that the cancer type might be the main source of heterogeneity. MLT did not reduce the incidence of stomatitis among patients with head and neck cancer under adjuvant chemotherapy or radiotherapy (RR=1.09, 95% CI (0.92 to 1.29), p=0.35), with low heterogeneity (p=0.64, I2=0%). However, it had significant value in patients with other kinds of tumours except head and neck cancer (RR=0.47, 95% CI (0.26 to 0.88), p=0.02) with high heterogeneity (p=0.03, I2=66%) (figure 12).

Forest plot of the effect of MLT on stomatitis incidence among patients with cancer. MLT, melatonin.
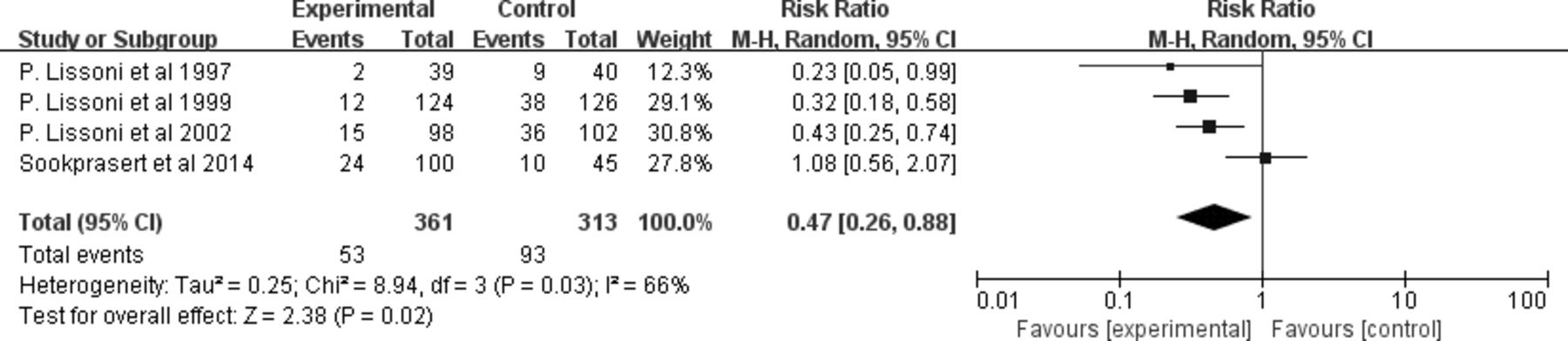
Forest plot of the effect of MLT on stomatitis incidence among patients with cancer except head and neck cancer. MLT, melatonin.
For stomatitis severity, three clinical trials evaluated the effect of MLT on reducing 3–4 grade (severe) stomatitis according to the WHO grading system.43 The overall treatment effect showed that the intervention had no statistically significant difference between the intervention and control groups (RR=0.78, 95% CI (0.47 to 1.30), p=0.35) with low heterogeneity (p=0.22, I2=35%) (figure 13).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of the effect of MLT on stomatitis severity among patients with cancer. MLT, melatonin.
Discussion
To the best of our knowledge, this study is the first meta-analysis to investigate the effect of MLT on QoL, sleep quality and other symptoms, such as fatigue, depression, pain and stomatitis, in patients with cancer. Unfortunately, in this study, we did not prove the beneficial effect of MLT on QoL, sleep quality, fatigue or pain. However, it has the potential to improve depression and reduce the incidence of stomatitis with small ESs.
Most of the suffering that patients with cancer now face comes from disturbing symptoms, such as poor sleep, fatigue, depression, pain and so on. Effective symptom control greatly improves QoL. Thus, the effect of MLT on QoL might be achieved through relieving symptoms. Innominato et al revealed that bedtime MLT was associated with a significant improvement in sleep quality, fatigue severity, QoL, and social and cognitive function in patients with advanced breast cancer.44 However, contradictory conclusions revealed that MLT did not improve appetite, weight, or QoL in cachectic patients with advanced cancer.45 In addition, a previous study reported beneficial short-term effects of MLT on sleep but not QoL.46 Our review included six trials that regarded the QoL of patients with cancer as a health outcome. None of them proved a significant improvement in QoL in the intervention group, although Grutsch et al26 and Sookprasert et al41 provided a trend for better QoL compared with baseline. For such invalid effectiveness, one of the possible interpretations might be the differences due to the study population, interventions and measurements. Another explanation might be the multidimensional properties of QoL, which contained domains of physical, psychology, spirit and social. Thus, the mere elimination of symptoms played a limited role in improving the QoL, especially for patients with cancer who were faced with many other disturbing aspects.
Due to the important role in regulating the circadian rhythm and sleep, many studies have been conducted to verify the value of MLT on sleep. MLT may be preferable to traditional hypnotics in the management of insomnia.47 A network meta-analysis supports the effectiveness of MLT in improving sleep-onset difficulties.48 A review of the influence of dietary sources of MLT on sleep quality indicated that the sources of MLT consumption of milk and sour cherries may improve sleep quality.49 There are many conflicting studies regarding different populations, dosages and durations. Fatemeh et al found the significant effects of MLT on sleep quality in patients with respiratory diseases, metabolic disorders and sleep disorders but not in mental disorders, neurodegenerative diseases and breast cancer.50 Under the condition of using the Pittsburgh Sleep Quality Index as a unified measurement tool, 20 mg MLT for 10 days in patients with breast cancer under chemotherapy showed a positive sleeping improvement,37 while the same dosage for at least 28 days revealed a meaningless result in patients with lung cancer.51 Meanwhile, the optimal combination of dosage and duration remains unknown. Innominato et al found that 5 mg for 2 months has a positive effect on sleep quality and QoL in patients with advanced breast cancer.44 Similarly, in patients with advanced cancer, the combination of 14 days 20 mg MLT plus bright white light therapy did not improve sleep quality.42 Under fewer doses, 14 days 3 mg MLT actually improved sleep in patients with cancer with insomnia.28 Our review revealed that MLT could not improve sleep. The subgroup analysis did not find a significant difference in different MLT durations, dosages, or combinations of dosage and duration. The optimal combination of dosage and duration in improving sleep for patients warrants further exploration. The administration type is another factor. It was found that a 2 mg prolonged release MLT formulation for 14 days resulted in significant and clinically meaningful improvements in sleep quality, morning alertness and sleep-onset latency in primary insomnia patients52 and in Parkinson’s disease patients with a poor sleep quality.53 However, most of the studies we included used oral MLT. How the administration type affects effect on sleep in patients with cancer remains to be studied. The effectiveness of the combination of bright light and MLT remains controversial. Yennurajalingam et al proved that it could not work in patients with advanced cancer with insomnia,42 while it could improve subjective daytime sleepiness in patients with delayed sleep phase disorder.54
MLT may be an effective treatment for patients with chronic fatigue syndrome.55 Nevertheless, in this study, none of the studies showed any improvement in fatigue in patients with cancer. Only a high-quality trial proved a significant effect of MLT on patients with reast cancer undergoing adjuvant chemotherapy and radiotherapy,38 with MLT doses of 18 mg a day from 1 week before until 1 month after adjuvant radiotherapy. The evidence supporting the usage of MLT for cancer-related fatigue (CRF) is limited. Short-term use of dexamethasone or methylprednisolone is recommended for the control of CRF in patients with metastatic cancer according to European Society for Medical Oncology guidelines,56 while the use of eszopiclone, megestrol acetate and MLT is not recommended for the control of CRF. However, the preventive effect of MLT on CRF is still under study. Nonpharmaceutical interventions were also recommended,56 such as relaxation exercise, massage, cognitive–behavioural therapy and physical activity, which were demonstrated to have moderate-to-large ESs.57 Multimodal therapy, qigong, aerobic exercise and cognitive–behavioural therapy might be the best choices for CRF.58
MLT seems to be able to ease pain. However, the results have varied in different studies. Lee et al found that the prophylactic administration of MLT conferred significant clinical benefits in reducing postoperative pain and opioid use, as well as improved sensory recovery following orthognathic surgery.59 Tunay et al found that preoperative oral MLT led to a reduction in pain scores, total morphine consumption and supplemental analgesic requirements after surgery.60 MLT could also improve pain in females with primary dysmenorrhea.61 However, the evidence was limited in critically ill patients in the ICU and patients after total knee arthroplasty.62 63 For patients with cancer, the evidence is also restricted. Our review revealed that MLT had no effect on pain relief. Only Elsabagh et al found a beneficial effect of MLT on alleviating pain in patients with head and neck cancer undergoing radiotherapy, with a dosage of 20 mg for 6 weeks.25 At the same time, Palme et al found a drop in pain scores from baseline in the intervention group.36 The minor role of MLT on pain in patients with cancer could be explained by the fact that cancer-related pain is one of the most common and troublesome symptoms affecting patients with cancer with high severity.64 For such severe pain, effective analgesics, such as opioids, are more helpful. In addition, despite the availability of effective treatments, cancer-related pain may be inadequately controlled in up to 50% of patients. Thus, multidisciplinary interventions are required,65 and single MLT seems too weak for cancer pain.
Circadian rhythm disruption underlies the pathophysiology of psychiatric disorders, especially depression.6 MLT is a pleiotropic regulator molecule, and its analogues have been observed to resynchronise the circadian rhythm and to alleviate depressive symptoms.66 However, duration and treatment might affect the antidepressant effects of MLT, and both showed a slight ES. We found that MLT supplementation had a significant effect in patients who received more than 14 days of treatments and those who underwent surgery. Our assumption is that patients under operation tend to be in the early stages of the disease with lighter disease load and slight depression. The antidepressant effect of a long MLT duration in patients with less serious disease was shown in some studies. For example, MLT for 12 weeks had beneficial effects on decreasing depression in women with polycystic ovary syndrome,67 patients with Parkinson’s disease68 and diabetic haemodialysis patients.69 Nevertheless, it had no prophylactic antidepressant effect on acute coronary syndrome70 or patients with acute mania.71
Oral mucositis refers to inflammation and ulceration of the oral mucosa, which is a frequent side effect of cancer therapy.72 Stomatitis, especially the grade 3 or 4 mucositis,73 can hamper oral nutrition, resulting in malnutrition, reduce QoL and introduce the need for dose reductions and interruption of chemotherapy.74 MLT has potential direct antitumour activity and has been proven to modulate the effects of cancer chemotherapy by enhancing therapeutic efficacy and reducing toxicity.75 Our review showed that MLT had no effect on mucositis. Further subgroup analysis showed that the cancer type was the major source of heterogeneity. MLT could not reduce the stomatitis rate among patients with head and neck cancer, while it had a slightly significant effect in patients with other tumours. Among the studies conducted in patients with head and neck cancer, Borbalas et al35 found that oral MLT gel demonstrated a consistent trend in lowering incidence and shortening mucositis duration.32 Onseng et al revealed that adjuvant MLT delayed the onset of oral mucositis. Elsabagh et al found that MLT reduced severe oral mucositis development.25 None of them proved that MLT could reduce the incidence of stomatitis. The possible interpretation was the significant toxicity of systemic high doses of chemotherapy and radiotherapy for head and neck cancer.76 Compared with other patients with cancer who only received chemotherapy or radiotherapy, most patients with head and neck cancer received the combined chemoradiotherapy. In addition, radiation in the head and neck increases the odds of stomatitis occurrence. We also found that in the MLT group, the reported incidence of stomatitis was higher in patients with head and neck cancer (52.5%–90%) than in other cancer populations (5.12%–24%). Moreover, our review revealed that MLT could not reduce the severity of stomatitis. A meta-analysis showed that probiotics might reduce the incidence and mitigate the severity of cancer therapy-induced mucositis.77 Additionally, photobiomodulation was recommended for the prevention of mucositis.78 79 However, how they affect patients with head and neck cancer under chemoradiotherapy is still unknown.
Strengths and limitations
To the best of our knowledge, this study is the first meta-analysis to investigate the effect of MLT on QoL and symptoms in patients with cancer. Eleven databases were widely searched for eligible studies. Risk of bias analysis was conducted independently by two reviewers using the validated Cochrane assessment tool. The trial quality was generally moderate, with most studies having a low risk of bias, which could further lend confidence to the current pooled results. In the subgroup analysis, we also widely explored the effectiveness of MLT in different populations, treatments, dosages and durations. There are some limitations. The first is the insufficient literature. We reviewed many aspects of MLT, such as QoL, sleep, fatigue, depression, pain and stomatitis. A total of 19 articles were included in the final meta-analysis. However, for every dimension, the literature is limited, from only 5–9. This is mostly the result of the lack of RCTs of MLT in patients with cancer. Thus, insufficient data were used for synthesis. There were 14 excluded articles without full text, which limits the generality of the conclusion. Meanwhile, the assessment of publication bias was not allowed because no dimension had more than 10 references. Furthermore, the main significant results were from subgroup analysis, and the results should be interpreted prudently.
Conclusion
Due to its nontoxic property and beneficial effects,80 81 MLT is increasingly used as an adjuvant medicine in anticancer treatment. We included a moderate number of trials with varied populations and examined the effectiveness of MLT on patients with cancer to provide evidence-based findings on using MLT in a real clinical setting. Our review showed that MLT did not improve QoL, sleep quality, fatigue or pain among patients with cancer. MLT has positive effects on decreasing the stomatitis incidence and depression, which may make it a reasonable option for stomatitis and depression prevention in the clinic. Even so, there are still many restrictions. Further large-scale RCTs are urgently needed. In addition, the effects of different combinations of MLT dosage and durations, administration types and joint measures are worthy of further study.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This is a meta-analysis. The Hunan Cancer Hospital Research Ethics Committee has confirmed that no ethical approval is required.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors had contributed to this study. XL and RF conceived and designed the original study protocol. RF and XB performed literature search and literature screening. SY and TW took responsibility for the integrity of the data and the data analysis. XL interpreted the results. YT and HC assessed the risk of bias of the studies. RF was responsible for writing the first draft of the paper and revision of the manuscript. XL is responsible for the overall content as guarantor. All authors critically reviewed and approved the final manuscript.
Funding This study was funded by Special Science Popularization for Construction of Innovative Hunan Province (2019ZK4029).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.