Article Text

Abstract
Objectives This study aimed to develop and assess the feasibility and cost impact of an intervention involving a practice pharmacist embedded in general practice to improve prescribing safety, deprescribe where appropriate and reduce costs.
Setting Four-doctor suburban general practice.
Participants Inclusion criteria: patients receiving 10+ repeat drugs per month. Exclusion criteria: deceased, <18 years of age, nursing home resident, no longer attending, late-stage life-limiting condition, unsuitable on clinical/capacity grounds. 137 patients were eligible. 78 were recruited as participants, all of whom completed the study.
Intervention Pharmacist conducting holistic medication reviews in the study group over a 6-month period.
Primary outcome measures Anonymised medication changes, cost, biochemical monitoring and clinical measurements data were collected. Cost analysis of having a pharmacist as part of the general practice team was calculated.
Results In total, 198 potentially inappropriate prescriptions (PIPs), and 163 opportunities for deprescribing were identified; 127 PIPs (64.1%) were actioned; 104 deprescribing opportunities were actioned (63.8%). The pharmacist identified 101 instances in which further investigations were warranted prior to prescription issue, of which 80 were actioned (79.2%). It was calculated that monthly savings of €1252 were made as a result of deprescribing.
Conclusions This study has shown that the integration of pharmacists within general practice in Ireland is feasible and is an effective means of improving prescribing safety and implementing deprescribing through medication reviews. The combination of safety and cost concerns support taking a holistic approach to deprescribing with the patient. This study highlights the ease with which a pharmacist could integrate into the general practice setting in Ireland and points to how this could be sustainably funded.
- PRIMARY CARE
- Health informatics
- HEALTH ECONOMICS
- Quality in health care
Data availability statement
Data are available in a public, open access repository. This does not include patient identifiable data. The full anonymised dataset is available from the Zenovo repository, DOI: 10.5281/zenodo.4475526.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The pharmacist, being embedded in the practice was able to gain valuable insights into the repeat prescribing and biochemical monitoring processes that can contribute to prescribing safety issues.
The holistic, patient-centred approach to medication reviews employed in this study increased the scope of potentially inappropriate prescriptions that could be identified.
The data collected during medication reviews is a snapshot of a single point in time, without follow-up to determine if whether deprescribed medications remained deprescribed.
In relation to the annualised cost savings on the medications prescribed, calculations were based on the assumption that patients collected all medications prescribed each month from the community pharmacy.
Cost calculations included only drug reimbursement prices and did not include additional costs such as pharmacist dispensing fees.
Introduction
WHO has estimated that at least half of all medicines are prescribed or dispensed inappropriately, with many resulting in avoidable harm.1 As populations age and more and more people live with chronic conditions, the use of multiple medications concurrently—generally referred to as ‘polypharmacy’—is becoming increasingly prevalent.2 This represents a key challenge to safe prescribing. Polypharmacy is often defined as being on five or more medications. However, there is a rising occurrence of ‘excessive’ polypharmacy, typically defined as being on 10 or more medications.3 ‘Problematic’ polypharmacy has been defined by The National Institute for Health and Care Excellence ‘as the prescribing of multiple medicines inappropriately, or where the intended benefits of the medicines are not realised’.4 Polypharmacy has been described as one of the greatest prescribing challenges in general practice (GP).5 It increases the potential for inappropriate prescribing,6 adverse drug reactions7 and drug–drug interactions.8 Potentially inappropriate prescriptions (PIP) can occur where a medication is prescribed without a valid clinical indication, or when the risks of prescribing outweigh the benefits.6 PIP is often assessed using explicit criteria that serve as an objective measure of medication appropriateness against accepted standards.9 According to a study carried out by Cahir et al, patients with PIP have been found to have a nearly two-fold increased risk in emergency department attendance.10 The number of medications prescribed is the most important predictor of inappropriate prescribing and risk of adverse drug events.11 12 ‘Deprescribing’ has been defined as ‘the planned and supervised process of dose reduction or discontinuation of medication(s) that may cause harm or are no longer providing benefit’.13 In contrast to when a drug is first prescribed, which involves establishing a diagnosis and indication for treatment, deprescribing is the process of determining which medication may be causing an adverse effect or lacks an indication.14
The management of patients taking multiple medications is a challenge for GPs, as there is often poor communication between primary and secondary care.15 Addressing incomplete reconciliation of medications and inadequate patient education were ranked as top safety priorities among 113 GPs in the PRIORITIZE study.16 While pharmacists in countries such as the UK and Canada have been formally integrated into GP, to date this has not been the case in Ireland.17 Studies outside Ireland have shown that pharmacists, working as part of the GP team, have positively affected prescribing safety18 and added value to patient-centred clinical services.18 19 However, to date, there is little evidence on the cost-effectiveness of pharmacists integrated within GP to improve prescribing practices and health outcomes in primary care.20
This study aimed to assess the feasibility and cost impact of an intervention in which a pharmacist worked within a GP setting to improve prescribing safety and deprescribing by conducting medication reviews with polypharmacy patients. The objectives were to identify the number and proportion of PIP, deprescribing opportunities, resultant cost savings and instances where biochemical monitoring/clinical measurements and patient education were required prior to prescription issue.
This study formed part of the Tomorrow’s Care project, which is a collaboration between the Health Service Executive (CHO 7 Division), Trinity College Dublin and a large teaching and academic practice (GPs at Tallaght Cross) examining innovative work practices in GP, including the introduction of a practice pharmacist and a data analyst.
Methods
This study was conducted at a single four-doctor suburban GP in West Dublin, which primarily serves patients with a medical card entitlement living in communities with a range of deprivation indexes. A practice pharmacist was present 1.5 days per week with the support of a data analyst. The role of the pharmacist was to resource the practice with activities such as deprescribing, improving prescribing safety and reducing costs.
Patient and public involvement
Given that this study sought to explore the utilisation of a practice pharmacist to improve prescribing safety and reduce costs, the focus of the study design was on the practicalities and operational aspects of integrating a pharmacist and collecting appropriate data. However, the interaction between the pharmacist and participants during the study also provided an opportunity to gain informal patient-level feedback that would highlight aspects that will benefit from more formal patient and public involvement in future studies.
Recruitment
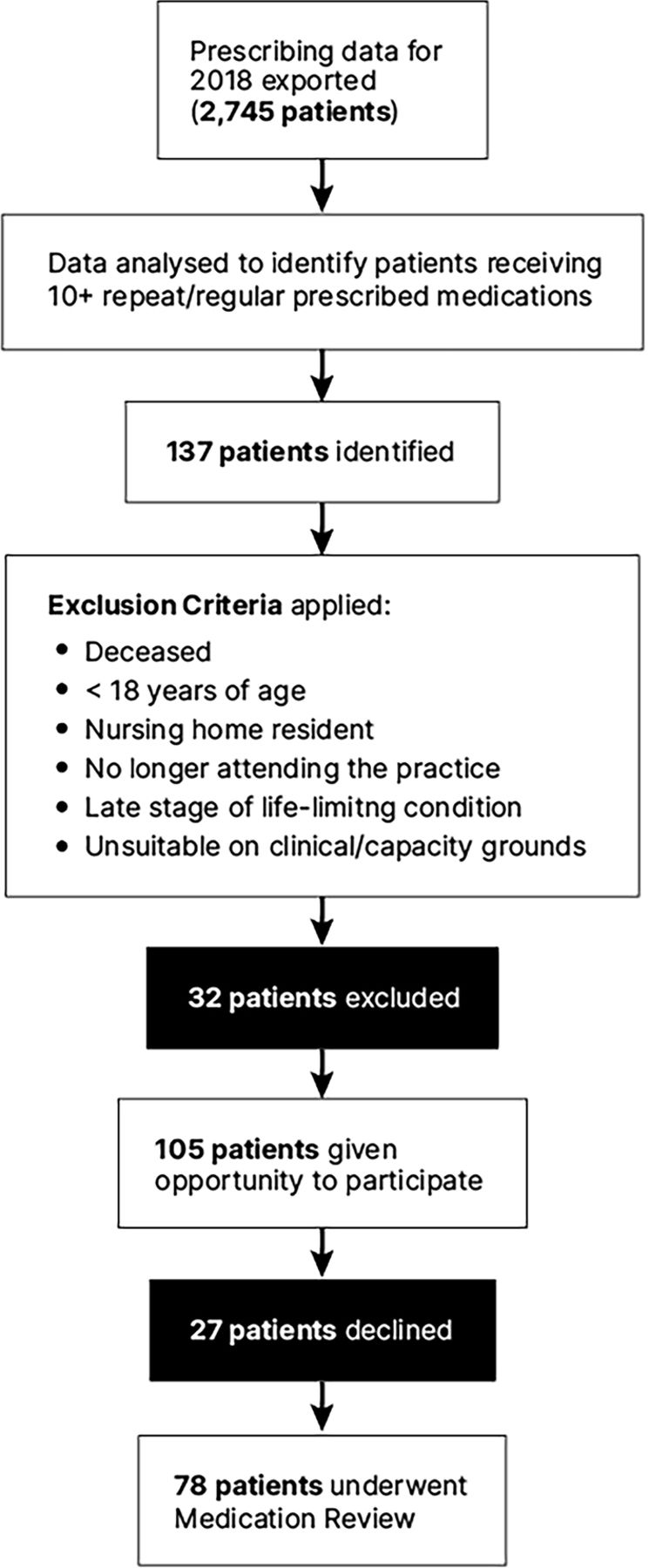
A prescriptions report for the year 2018 was generated using the practice management software and processed using Microsoft Excel and Microsoft Access to provide details of all drug items prescribed. The following inclusion criteria was applied: any active patient of the practice prescribed 10 or more regular medications per month. Medications for acute illnesses, such as antibiotics, were not included because such items are for temporary short-term use only, and so were not considered by the authors as constituting ‘regular’ medications. In total, 137 patients were identified using this approach in advance of the intervention period from January to June 2019 (figure 1).

Participant selection process.
Common chronic conditions such as Type 2 Diabetes and Chronic Obstructive Pulmonary Disease, with their associated polypharmacy, are often thought of as diseases of the elderly. However, such conditions are increasingly recognised as affecting younger age groups.21 22 For this reason, patients over 18 years of age were included. Exclusion criteria (figure 1) were then applied, and 105 patients were deemed eligible. Eligible participants were recruited by the practice manager at the time of repeat prescription request during the 6 month period from January to June 2019. In total, 78 patients agreed to participate. Informed consent was obtained, and medication reviews scheduled.
Medication review
The Polypharmacy Guidance Realistic Prescribing tool23 was selected by the pharmacist as a basis for the medication reviews due to its holistic patient-centred approach (figure 2). A medication was deemed inappropriate if it did not have a valid indication, was prescribed at the wrong dose or duration, or carried a high risk of an adverse drug interaction or event. Clinical judgement, taking into account patient perspective and contextual factors, was used to identify instances of PIP and opportunities for deprescribing.

The medication review process. GP, general practice.
Each medication review took approximately 45–60 min and followed a structured, stepwise process:
Step 1—review diagnoses and clinical notes and identify what matters to the participant.
Step 2—identify potentially unnecessary medications. Review clinical history, hospital prescriptions and correspondence. Clarify errors or omissions on the medication list. Expired indications, higher than usual maintenance doses, or excessive quantities were noted.
Step 3—reconcile medications, including non-prescription medications, by liaising with the participants and community pharmacist to obtain a complete and accurate medication list. Note instances of non-adherence.
Step 4—check that clinical measurements, biochemical results and chronic disease management reviews are up to date.
Step 5—highlight medication safety concerns, such as drug interactions, and robustness of biochemical monitoring for high-risk medications, such as ACE inhibitors, diuretics, metformin, non-steroidal anti-inflammatory drugs (NSAIDs), anticoagulants and methotrexate.
Step 6—check for opportunities to substitute more cost-effective alternatives.
Step 7—deliver education regarding indications, correct use of medications, biochemical monitoring and clinical measurements. Discuss potentially unnecessary medications and enquire about medication adherence.
During each review, numerical data were gathered in Excel.24 Following each medication review, the findings and relevant suggestions were reported to the GP. There followed a discussion between the GP and pharmacist regarding appropriate medication changes or relevant monitoring/investigations. Where further monitoring was required the pharmacist organised this directly with the practice nurse and patient. Finally, the GP or pharmacist informed the participants and their community pharmacist of any medication changes. The participants were given an accurate up-to-date medication list outlining the indications for each medication and associated cautions. Eight weeks following review, telephone contact was made with the participants to check adherence and address any issues.
Cost calculations
Cost savings resulting from deprescribing of medications were calculated using publicly available drug reimbursement prices25 alone, and did not include additional fees, such as pharmacist dispensing fees. For each medication that was prescribed during the study period, the total cost to the health system over twelve months was calculated. A cost analysis was conducted to determine the total savings, taking into account the cost of providing the intervention.
Results
In total, 78 participants underwent medication review, resulting in the identification of 198 PIPs, and 163 opportunities for deprescribing.
Potentially inappropriate prescriptions
Of the 198 instances of PIP, 127 (64.1%) were successfully actioned by the pharmacist and GP. The reasons that prescriptions were deemed inappropriate were identified and categorised (figure 3).

Number of instances of potentially inappropriate prescriptions identified (PIPs), by rationale and percentage subsequently actioned.
Expired Indication accounted for 67 (33.8%) of PIPs identified. Examples included ‘as required’ medications that were no longer needed, and medications that had been stopped in hospital but remained on the GP’s medication list. Inhalers were the most common type in this category. In many cases, medications prescribed in hospital for short-term use persisted on the medication list inadvertently. Typical examples were supplements, laxatives, and antiemetics. Of the 67 PIPs in this category, 74.6% were removed from medication lists.
Excessive quantity accounted for 43 (21.7%) of PIPs. This category largely comprised inhaled bronchodilators, opioid/paracetamol combinations, antianginal sprays and topical NSAIDs, which were often included on repeat prescriptions despite no longer being required. The GP subsequently removed 62.8% of PIPs in this category from medication lists.
Excessive duration accounted for 37 PIPs (18.7%), and consisted predominantly of benzodiazepine and Z-drugs, which are generally indicated for short-term use. Only 10.8% of this category of PIPs were successfully addressed.
Incorrect dose accounted for 30 PIPs (15.2%), 29 of which were successfully addressed (96.7%). A common example was proton pump inhibitors (PPIs), which in a number of cases continued to be prescribed at a high-dose despite a hospital-issued prescription specifying a dose reduction after a defined period of time. There were also a number of cases identified where a dose change had been documented by the prescriber in the clinical notes, but the medication list had not been amended accordingly.
Drug interactions accounted for 13 PIPs (6%). The most frequent drug interaction identified was the analgesic tramadol combined with selective serotonin reuptake inhibitors. NSAIDs were frequently identified as a source of potential drug–drug and drug–disease interactions, particularly with regard to concomitant use with anticoagulants, as well as in the presence of certain comorbidities, older age, and excessive alcohol use. The GP subsequently addressed 9 (69%) of these PIPs following review.
Deprescribing
At least one opportunity to deprescribe was identified in 66 participants (84.6%), with an average of 2 deprescribing opportunities per participant. In one case, seven opportunities were identified for a single participant. In total, 163 deprescribing opportunities were identified across the medication review group, with 104 addressed by the GP and pharmacist (63.8%). Figure 4 illustrates the number of deprescribing opportunities and the proportion that were successfully addressed according to drug class.

Top 15 deprescribing opportunities by drug class, including number of deprescribing opportunities, number deprescribed (actioned) and associated monthly savings. NSAID, non-steroidal anti-inflammatory drug; PPI, proton pump inhibitor.
Deprescribing efforts were more effective in some drug classes than others. NSAIDs (topical and oral), laxatives and antiemetics, were the most successful classes, with 100% of deprescribing opportunities actioned. Deprescribing oral NSAIDs, in particular, was very effective where safety concerns were identified. There was also relatively good success in deprescribing inhalers, with 86.6% of those that were no longer indicated successfully deprescribed. Similarly, deprescribing of maximal dose PPIs was largely successful (77.7%), resulting in a reduction to maintenance dose as per hospital prescription instructions. In some cases, participants were taking antispasmodic medications daily, despite the fact that such medications are only indicated for intermittent use. When educated on the indication, correct use and lifestyle changes, half of the participants prescribed antispasmodics agreed to discontinue use.
Deprescribing of opioid/paracetamol combinations, benzodiazepines and sedative hypnotics was less successful, with 54.4%, 16.6% and 7.6% addressed by the GP and pharmacist, respectively.
Biochemical monitoring and clinical measurements
The pharmacist identified 101 instances in which further investigations were warranted prior to prescription issue, of which 80 were actioned (79.2%). Examples included monitoring of renal and thyroid function, lipid profile, blood pressure measurement and cases in which an ECG was required.
Patient education
The pharmacist discussed adherence and correct use of medications with 97% of participants. Interaction with community pharmacists was particularly effective in identifying and clarifying instances of medication non-adherence. Each participant was given an accurate up-to-date medication list outlining the indications for each medication, the doses and associated cautions. Education regarding lifestyle advice was delivered to 60% of participants.
Cost impact
It was calculated that monthly savings of €1252.48 were made as a result of deprescribing 104 medications. This could be expected to deliver annual prescription savings of €15 029 in the subsequent 12 months.
Discussion
Our findings suggest that the role of the practice pharmacist in relation to safety is both important and effective, as evidenced by the number of PIPs and deprescribing opportunities identified and addressed.
The intervention was effective, in that a majority of the pharmacist’s recommendations were implemented successfully. This is in line with other studies that suggest medication reviews delivered by pharmacists in the GP setting are more effective than those delivered in the community pharmacy setting.26 27 Possible explanations include barriers that are relatively more problematic in community pharmacy, namely physical separation from GPs, communication difficulties and limited access to patient records.28 The integration of pharmacists into the GP setting offers a potential solution to these barriers by facilitating ease of access to medical records, and ultimately improving communication and cooperation between healthcare professionals.26 The authors felt the high response rate to the intervention (74%) supports both the acceptability of medication reviews to patients and the effectiveness of recruiting patients at the time of repeat prescription requests by the practice manager, a member of the practice team who is familiar to the patients.
Moriarty et al concluded that ‘no single PIP measure appears to be superior to another and therefore the choice of how to measure PIP in research or practice should be considered in light of the circumstances and requirements in each case’.9 Thus, for this study, it was decided not to focus solely on standard instruments for measuring prescribing appropriateness, such as the Screening Tool of Older People’s prescriptions-Screening Tool to Alert to Right Treatment criteria29 and Beers criteria,30 because such measures depend predominantly on pharmacological criteria, and fail to take into account patient preference and certain domains of prescribing appropriateness, such as indication, formulation and cost.31 Rather, a broad definition of PIP was chosen for this study that included patients’ perspectives and contextual factors which allowed a less restrictive type of medication review. While this enabled a more holistic approach to medication reviews, it is likely that this led to the identification of a higher prevalence of PIP than had standard instruments been used alone - 94.8% of participants were found to have at least one PIP.32–34
Despite this holistic approach, our findings in terms of the common types of PIPs encountered in this study are in line with those of previous studies in that maximal dose PPI prescribing and long-term benzodiazepine prescribing were prominent (figure 5).32 35

Top 10 most frequently identified potentially inappropriate prescriptions (PIPs), by class and percentage of total PIPs identified. NSAID, non-steroidal anti-inflammatory drug; PPI, proton pump inhibitor.
Expired indications accounted for a large percentage of PIPs and deprescribing opportunities of which 74.6% were actioned. During medication reviews, the pharmacist noted that in many cases the computerised record was inaccurate in that medications had not been removed from the current medication list (eg, maximum dose PPIs, inhalers with expired indications, laxatives and antiemetic medications). Our study has identified that a practice pharmacist is well placed to improve the quality and accuracy of GP-held medication records.
Excessive quantities of prescribed items were also a notable finding of this study (21.7% of PIPs). The delivery of education by the pharmacist was particularly effective in this regard, as it helped patients to better understand drug indications, and the differences between medications that were essential and those for use on an intermittent basis. We feel this approach helped to empower the participants to work with the pharmacist to identify potentially excessive medication quantities on their prescriptions. Evidence supports the active involvement of patients in their healthcare decisions in order to achieve better health outcomes.36–39 It is our view that patient involvement and partnership is essential in addressing polypharmacy and its associated risks.
Medications prescribed for excessive duration posed a distinct challenge, with only 10.8% successfully actioned. Of the 37 PIPs in this category, 20 were of the benzodiazepine class; 17 were sedative hypnotics. Community detoxification of chronic benzodiazepine use is a recognised challenge,40 41 in part due to drug tolerance making it difficult to implement interventions designed to improve prescribing.42 In that context, it is important to acknowledge that there was some success in reducing use of these medications. There is evidence to suggest that increasing participation of elderly patients in prescribing decisions can help reduce the inappropriate use of benzodiazepines.43 Our findings support such an approach.
As part of the medication review process, participants were given an up-to-date copy of their medication lists outlining the indications for medications, associated cautions and, where applicable, ongoing requirements for monitoring. The pharmacist encouraged participants to keep this information with them at all times to ensure the availability of an accurate source of medication history at transitions of care. Studies suggest that up to 60% of patients admitted to hospital have a discrepancy on their medication list44 and 53% of adult patients have medication errors after discharge.45 Therefore, providing patients with their own accurate medication list is imperative to ensuring the quality and availability of medication information s at transitions of care as recommended by WHO.46
While many medications are initiated in secondary or tertiary care, the majority of prescribing takes place in primary care.47 Given the numerous complexities and considerations that were identified during the medication reviews, it is reasonable to expect that GPs might be able to dedicate time to medication management activities. However, a recent study of GP workloads demonstrated that the average time spent by GPs on medication management during a 10-hour work day was only 21 min.48 This disparity highlights a potentially valuable role for the practice pharmacist in reducing GP workload by taking over non-consultation tasks, such as medication reviews. In our experience the pharmacist was well placed to collaborate with the practice nurse, who had considerable experience and knowledge of the participants, to organise biochemical monitoring for high-risk medications and ensure appropriate clinical measurements were recorded. This is an example of the multidisciplinary team working together to improve medication management.49 Furthermore, the practice pharmacist was ideally suited to liaise with the community pharmacist regarding adherence issues, particularly in cases where participants were reluctant or unwilling to disclose such issues directly.
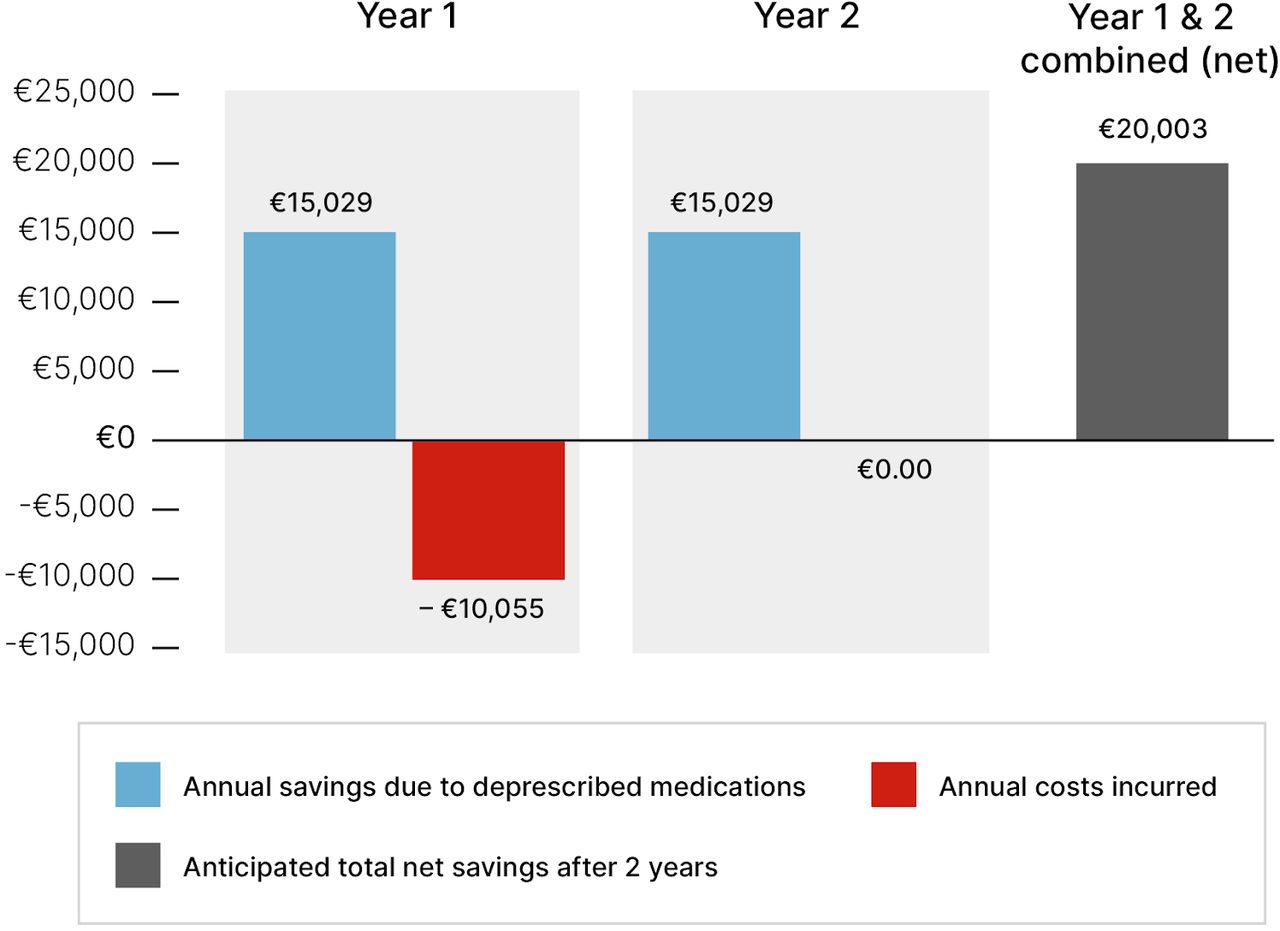
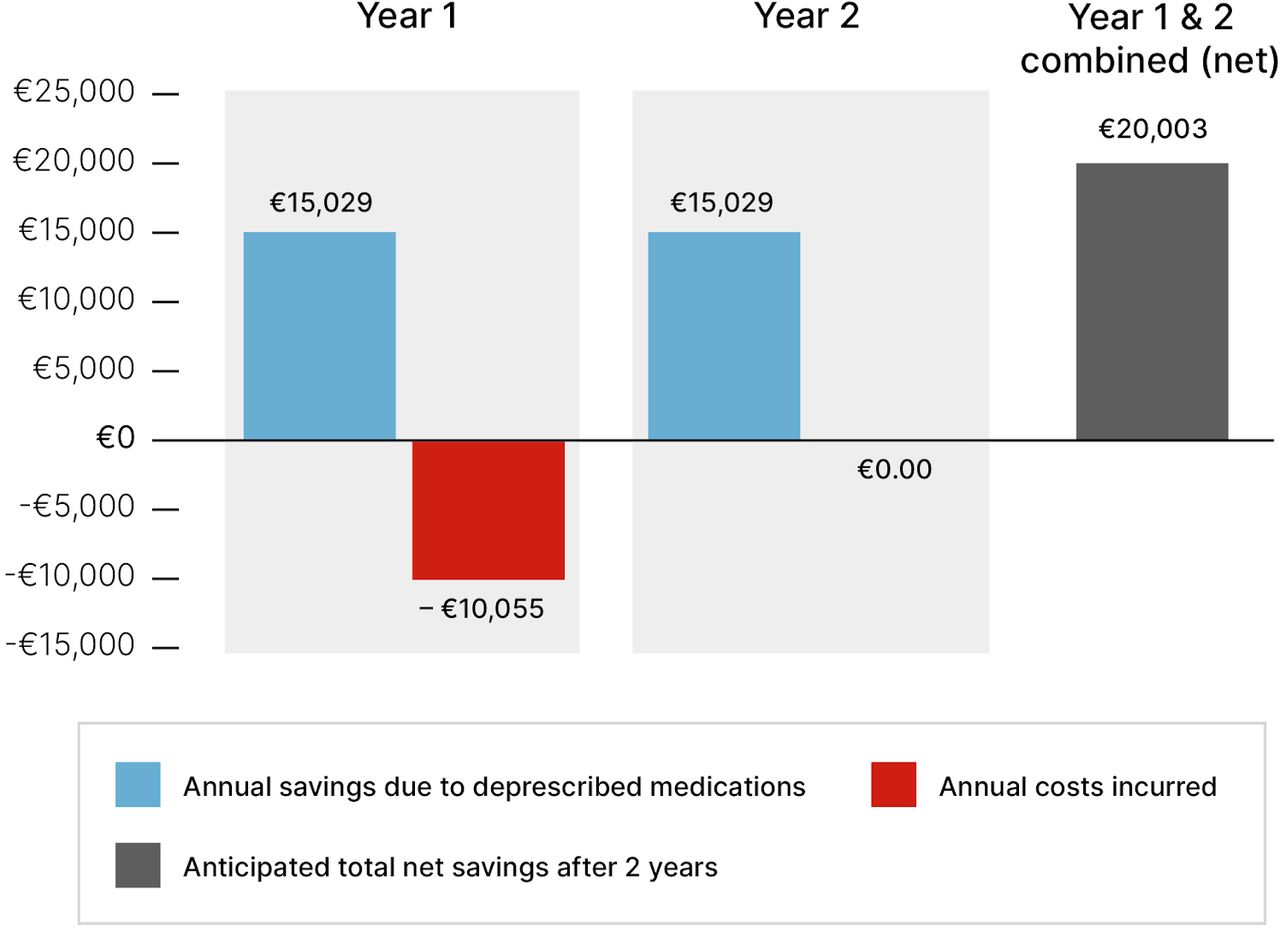
It was calculated that the medications deprescribed during this study would result in an annual cost saving of €15 029. Savings were made across a range of drug classes, with inhaled medications identified as a particularly high-yield cost saving group (figure 4). The total cost of the pharmacist’s salary for the study period was €10 055. This was based on €35 /hour for 10 hours/week over 26 weeks. Other variable costs, such as room rental and GP time, did not apply in this study, but may need to be considered as potential costs in future initiatives. Assuming that the medication changes implemented during the study persisted, net savings of €4974 could be expected by the end of the first year. If the medication changes persisted longer term, net savings of €15 029 could be expected by the end of the second year. This is because the cost of the pharmacist was incurred up-front. Therefore, total net savings of €20 003 could be projected after 2 years. This represents a twofold return on the initial outlay, and a saving of approximately €256 per patient over a 2-year period (figure 6). These figures do not take into account the potential positive impact the medication reviews may have had on costs associated with PIP-related morbidity and medication-related hospitalisations. Cost avoidance measures that reduce potential future spending can result in substantial cost savings over an extended period of time.50
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Projected cost savings over a 2-year period following prescribing interventions.
The intervention was delivered over a 6-month period. In our experience, this was sufficient to allow thorough medication reviews for this volume of patients. This highlights the potential for a single practice pharmacist to carry out medication reviews in two similar-sized practices within a single 12-month period.
Limitations of this study
This was a pilot study examining the integration of a practice pharmacist into a GP to improve prescribing safety and prescribing costs. As such, it does not demonstrate the impact of this intervention on patient outcomes, such as adverse drug events or health service utilisation.
There are a number of important caveats for interpreting our findings. There may have been a selection bias in relation to the exclusion criteria, particularly when patients were deemed unsuitable on clinical or capacity grounds by the GP. By indicating a willingness to participate, there may have been a response bias among those patients who did participate.
The generalisability of this study is limited by inclusion of only one practice, although it was diverse in terms of practice characteristics. It is unclear whether these findings are representative of other practices, where prescribing volumes and patient demographics differ.
The data collected is a snapshot of a single point in time, without follow-up to determine if changes made to patients’ medications persisted. Calculations of annualised cost savings due to deprescribing were based on the assumption that medication changes persisted.
The reviews were carried out by a single pharmacist which may have introduced a degree of subjectivity, particularly in relation to recording PIP.
Strengths
This study represents a real life, pragmatic approach to the integration of a pharmacist into an Irish GP setting to improve prescribing safety and deprescribing.
By being embedded in the practice, the pharmacist was gained valuable insights into repeat prescribing and monitoring processes and the need for regular medication review mechanisms.
This study employed a holistic, patient-centred approach to the medication reviews, empowering patients through shared decision making and uncovering considerable levels of potentially inappropriate prescriptions in the process.
Future research
The insights gained during this study highlight several areas that the authors suggest merit further study. These include further study to assess whether the changes implemented in the intervention were sustained, and to examine if both the medication review process and its cost impact is replicable at other sites.
The authors suggest examining whether pharmacist prescribing rights and the use of predefined protocols for the pharmacist may have a role in medication management.
The pharmacist’s experience of conducting medication reviews highlighted the potential value in providing the patient with an up-to-date medication list, thereby providing the patient with the means to reduce the risk of medication errors that occur at transitions of care. Further research into developing systems that enable an accurate patient-held medication list could be of great benefit.
Conclusions
Our findings indicate that the integration of pharmacists within GPs in Ireland is feasible and is an effective means of addressing PIP and implementing deprescribing through medication reviews, and addressing challenges with the GP workload. The combination of safety and cost concerns support a holistic approach to deprescribing. In our experience, the Polypharmacy Guidance Realistic Prescribing tool offers an effective template for medication reviews. This tool is being used in a large international study, the SIMPATHY Project, which examines inappropriate polypharmacy across the European Union.51 The continuous improvement of polypharmacy management in Scotland since 2012, and learnings from SIMPATHY, have helped shape this tool.23 This study demonstrates that a practice pharmacist, while uncommon in Ireland, can be a valuable and pragmatic resource in the Irish GP setting, and points to how such a role could be sustainably funded.
Data availability statement
Data are available in a public, open access repository. This does not include patient identifiable data. The full anonymised dataset is available from the Zenovo repository, DOI: 10.5281/zenodo.4475526.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Trinity College Dublin School of Medicine Research. Ethics approval ID: 20180401.
Acknowledgments
We would like to acknowledge the assistance of Dr James O’Mahoney, Research Assistant Professor in Cost-Effectiveness Analysis, Centre for Health Policy & Management, School of Medicine, Trinity College Dublin, for his assistance in considering the cost-consequence of the study.
References
Footnotes
Contributors DÓC, A-MB and MÓC were involved in developing the study design. A-MB was responsible for conducting medication reviews. DC and MÓC were responsible for managing the data collection and analysis with additional input from DÓC and A-MB. A-MB prepared the initial manuscript with additional input by DÓC, DC and CD. DÓC and CD critically reviewed the manuscript and suggested revisions. All authors read and approved the final manuscript. DÓC is the guarantor with overall responsibility for the work, conduct of the study, data management, and control of the decision to publish.
Funding This work was supported by the Health Service Executive and Trinity College Dublin grant number 55838838. This study formed part of a larger pilot study examining the integration of a pharmacist into a general practice. The Tomorrow’s Care project is a collaboration between the Health Service Executive (CHO 7 Division), Trinity College Dublin and a large teaching and academic practice (GPs at Tallaght Cross). This project funded a data analyst and pharmacist for this study. Tomorrow’s Care is funded by the CHO7 Division of the Health Service Executive.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.