Article Text

Abstract
Introduction The inappropriate use of antibiotics is a key driver of antimicrobial resistance. In China, antibiotic prescribing and consumption exceed recommended levels and are relatively high internationally. Understanding the influences on antibiotic use is essential to informing effective evidence-based interventions. We conducted a scoping review to obtain an overview of empirical research about key behavioural, cultural, economic and social influences on antibiotic use in China.
Methods Searches were conducted in Econlit, Medline, PsycINFO, Social Science citation index and the Cochrane Database of Systematic Reviews for the period 2003 to early 2018. All study types were eligible including observational and intervention, qualitative and quantitative designs based in community and clinical settings. Two authors independently screened studies for inclusion. A data extraction form was developed incorporating details on study design, behaviour related to antibiotic use, influences on behaviour and information on effect (intervention studies only).
Results Intervention studies increased markedly from 2014, and largely focused on the impact of national policy and practice directives on antibiotic use in secondary and tertiary healthcare contexts in China. Most studies used pragmatic designs, such as before and after comparisons. Influences on antibiotic use clustered under four themes: antibiotic prescribing; adherence to antibiotics; self-medicating behaviour and over-the-counter sale of antibiotics. Many studies highlighted the use of antibiotics without a prescription for common infections, which was facilitated by availability of left-over medicines and procurement from local pharmacies.
Conclusions Interventions aimed at modifying antibiotic prescribing behaviour show evidence of positive impact, but further research using more robust research designs, such as randomised trials, and incorporating process evaluations is required to better assess outcomes. The effect of national policy at the primary healthcare level needs to be evaluated and further exploration of the influences on antibiotic self-medicating is required to develop interventions that tackle this behaviour.
- public health
- health policy
- international health services
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The scoping review design facilitated the inclusion of a wide range of evidence using varied study designs and enabled a comprehensive summary of the extent and nature of the evidence base concerning influences on antibiotic use in China.
This scoping review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews guidelines.
A narrative synthesis was additionally undertaken to enhance the accessibility of the results for policy-makers, practitioners, and consumers, facilitating uptake of evidence-based practice.
A limitation of the scoping review method is that a quality assessment of the evidence is not conducted and therefore the relative robustness of the evidence is not systematically reported.
The review used English search terms and searched databases of literature published predominantly in English, therefore, evidence published only in Chinese is not included in this review.
Introduction
Antimicrobial resistance (AMR) is widely regarded as an increasing threat to global health and well-being. The overuse and misuse of antibiotics has been identified as a key driver of AMR.1 In China, studies have shown that both antibiotic prescribing and consumption exceed recommended levels, and are higher than in many other countries.2–5 For instance, at Community Health Institutions across China prescriptions for antibiotics were double WHO recommended levels.2 6 An investigation of antibiotic consumption from 2000 to 2010 across 17 countries found a 36% global increase, of which 76% was accounted for by an increase in five countries, including China.4
Improving our understanding of the drivers of inappropriate antibiotic prescribing and consumption are key to informing the development of evidence-based policy and practice. Much of the available evidence on which current policy and practice are informed emanates from European and North American countries. This evidence suggests that diverse, and multilevel factors operate at individual, societal, organisational and policy levels to influence suboptimal antimicrobial use.7 8 Although some influences may be common across different countries and populations, cultural and structural differences need to be identified and responded to within specific settings. A better understanding of variation between countries is necessary to design interventions that are context and target group specific, in order to reduce health and care inequalities.
Since the late 1970s China has undergone far-reaching economic change with a rapidly expanding market-oriented economy,9 resulting in the weakening of the community health and medical system that was developed under Mao Zedong. A consequence of these changes has been the need for myriad healthcare reforms that aim to provide all citizens with access to basic medical care.10 Primary healthcare is delivered through community health centres (CHC) and stations (CHS) in urban areas and through township health centres (THC) and village clinics (VCs) in rural areas. CHC, CHS and THC are all part of the state healthcare system, whereas VC are run by independent practitioners, although VC are contracted to deliver some public health services and are to some extent overseen by THC.11 Practitioners at THC all have some biomedical training, whereas practitioners in VC may have trained principally in Traditional Chinese Medicine (TCM) and have only minimal biomedical training. TCM is widely available within the state system, with over 90% of CHC and THC providing both TCM and biomedical treatments.12 The costs of most health services provided by both state run and VC will be reclaimed from one of the three major Government run health insurance scheme (for rural residents, urban employed or non-working urban residents such as children, elderly and disabled).13 The provider–payment mechanisms introduced to ensure universal access to primary care in China unintentionally introduced incentives that led to over utilisation of medicines and services.14
The overuse of antibiotics was inadvertently incentivised by some of these reforms. For instance, government subsidies for public hospitals sharply declined from 60% of total hospital revenue in the early 1980s to less than 25% by 2008, while remuneration mechanisms for clinicians allowed a 15% markup on biomedical pharmaceuticals from initial wholesale cost to retail price, thus incentivising drug prescribing.15 16 Other hypothesised influences on antibiotic overuse and misuse include patient expectations and beliefs about antibiotics and a lack of access to laboratory diagnostics for village practitioners.11 17–19 However, the extent and scope of the available evidence concerning key influences on antibiotic use in China has not been collated or synthesised, to our knowledge. We address this gap through a systematic scoping review of the evidence that aims to answer the following question: What is the evidence concerning key behavioural, cultural, economic and social predictors for, and explanations of, antibiotic use in humans in China?
Methods
A systematic scoping review was undertaken to explore and map the evidence base in this broad and complex area.20 The review protocol was published on the Open Science Framework21 prior to conducting the database searches. We drew on an established framework to guide the methodology and adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews.22 The volume, nature and characteristics of the primary research were mapped in order to identify evidence gaps, which can be further examined in subsequent research. A narrative synthesis of a large and wide-ranging body of research sought to make the results accessible to policy-makers, practitioners and consumers, facilitating uptake of evidence-based practice.
Eligibility criteria
To systematically develop an inclusive review approach, the SPICE framework was used to define its scope23:
Setting: Chinese hospitals, health clinics, pharmacies and the community.
Population: humans of all ages.
Phenomenon of interest: factors associated with antibiotic use including prescribing.
Comparison: any or no comparator.
Evaluation: no restriction (all study types included).
All study types including quantitative descriptive and intervention studies, qualitative, mixed-methods and systematic reviews were eligible for inclusion. In the category of intervention studies, we included both experimental research (eg, randomised controlled trials (RCTs)) and non-experimental studies (eg, studies analysing secondary data in order to examine the effects of real-world policy changes).
We excluded studies from countries other than China, abstracts, commentaries and letters.
Search strategy
Searches were conducted in Econlit, Medline, PsycINFO, Social Science citation index and the Cochrane Database of Systematic Reviews chosen to cover a range of disciplines including anthropology, economics, medicine, politics, psychology and sociology. The search period was from 1 January 2003 to 28 February 2018. A start date of 2003 was chosen as this was the year the New Rural Co-operative Medical System was introduced in China; a voluntary health insurance programme for rural residents that is subsidised by central, provincial and county governments and seeks to improve rural access to healthcare.24 A list of key English search terms were compiled based on existing antibiotic reviews,5 17 25 using the SPICE framework and checking and reviewing the abstract of relevant articles for commonly used terms. Database searches were combined with Boolean search commands (see online supplemental file 1) for search terms. Records were stored and managed in Endnote V.X9.
Supplemental material
Study selection
Twenty per cent of all titles and abstracts were independently screened by two reviewers (AS and CCo or AS and PK) to check inter-rater reliability. Reviewers discussed their inclusion decisions until consensus could be reached. Having checked that the inclusion criteria were understood and implemented properly, one reviewer (AS) screened all remaining studies. Six of the studies reviewed, in Mandarin, were assessed for eligibility by a Mandarin-speaking coauthor (RF) who was familiar with the review process. During the screening of these six studies, English language versions were identified for five of these and, four studies were assessed as eligible for inclusion (CCo). Full texts of all studies included at screening were reviewed for eligibility and reasons for exclusion were documented. The included studies were grouped into two main types during the selection stage: (1) intervention and (2) descriptive/non-intervention studies.
Data extraction
A data extraction form was developed and incorporated details on the source, study design, behaviour related to antibiotic use, influences on behaviour and intervention effect (see online supplemental file 2). Data were extracted by one reviewer (CCo). Ten per cent of studies underwent double-data extraction (CCa) to check for internal consistency of the process. Where discrepancies occurred, these were discussed and resolved by consensus.
Supplemental material
Patient and public involvement
There was no formal involvement of patients or the public in this scoping review.
Collating, synthesising and reporting results
The extracted data were quantified by study characteristics using Excel and Stata (V.15).26 Summary information included year of publication, study design, economic region of China,27 study context, population sampled or type of data, and main focus of the study including the type of intervention assessed in the case of intervention studies.
For the descriptive/non-intervention studies, a narrative synthesis was conducted to facilitate the organisation and summary of the data.28 We used the Behaviour Change Wheel system for further characterising intervention types into nine intervention functions and eight policy categories (see table 1).29
Definitions of interventions and policies described by the behaviour change wheel
Results
Description of included studies
After removal of duplicates, the initial electronic searches identified 2305 potentially eligible records. Screening identified 75 studies matching the inclusion criteria (figure 1).
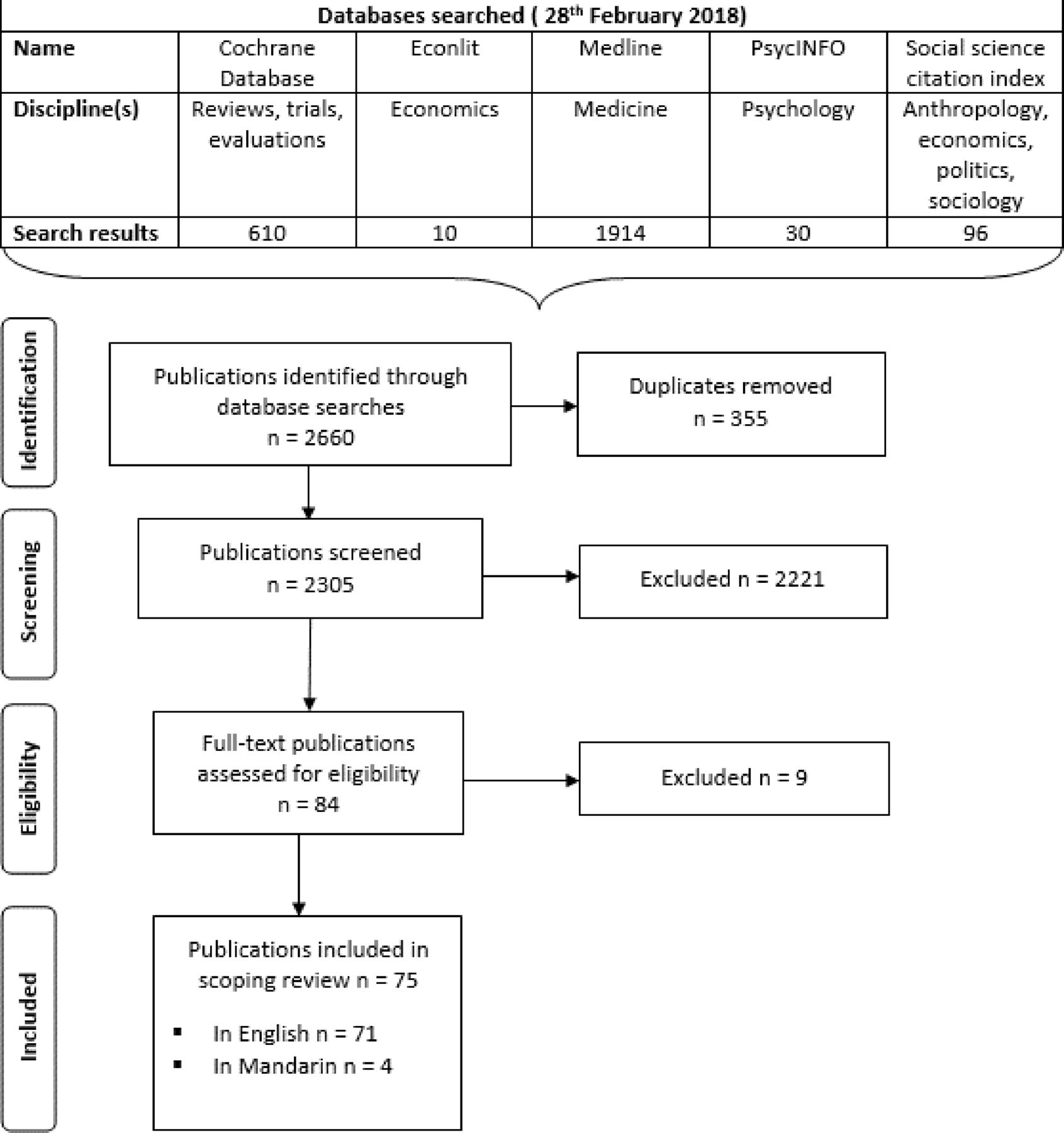
{kind=link}
Flow diagram of the selection process for publications included in the scoping review.
A summary of key study characteristics is presented in table 2 and additional details of intervention studies in table 3. Intervention studies made up nearly two-thirds of the included studies (44/75) (table 2). Overall, few studies were published from 2003 to 2009 (5/75), while the 1-year period from 2014 to 2015 accounted for 31 studies and the latter period (2016–February 2018) 21 studies. Over half of studies were conducted in East or Central China. Almost half of the descriptive studies (15/31) were conducted in community settings, and of those conducted in clinical settings none were conducted in tertiary or teaching hospitals. All intervention studies were conducted in clinical settings, of which 36% were conducted in primary care or CHC (16/44). Intervention study populations included adult and child in-patients, physicians, other healthcare workers and community members (table 3). Primary outcomes were antibiotic use (n=17) and antibiotic prescribing (n=19). Most of the intervention studies used a comparator group design (n=39). National policy guidance made up many interventions evaluated (n=20) while other interventions included public reporting of antibiotic prescribing, pharmacist interventions with local antibiotic stewardship, performance related pay, medical insurance and educational or other interventions. In respect to behaviour change intervention and policy categories, only the primary category is presented, although it was common for interventions to incorporate more than one intervention and policy category.
Description of all studies included in the scoping review (n=75)
Characteristics specific to intervention studies included in the scoping review (n=44)
Summary of key behaviours and influences
A synthesis of the findings from included studies was based on study type (intervention/descriptive) and key behaviours relating to antimicrobial use including antibiotic prescribing, adherence to antibiotics, self-medicating with antibiotics and the sale of antibiotics without a prescription (table 4). Details of the studies and their key findings are presented in online supplemental file 3 (descriptive studies) and online supplemental file 4 (intervention studies).
Supplemental material
Supplemental material
Main categories and subcategories from the narrative analysis of the descriptive studies (n=31)
Antibiotic prescribing
Fourteen descriptive studies identified influences on antibiotic prescribing (online supplemental file 3),15 17 18 30–42 which included: clinical assessment, healthcare practitioners’ skills, knowledge and training, patients’ knowledge and expectations concerning antibiotics, external or environmental factors and financial incentives (table 4). Most intervention studies (42/44) focused on antibiotic prescribing or consumption as a key outcome measure (online supplemental file 4).43–84
Clinical presentation
Clinical assessment, incorporating both symptoms and patient characteristics, was a key factor influencing prescribing decisions. Greater severity of illness and the presence of certain disease related symptoms predicted antibiotic prescribing.34 38 Symptoms that favoured antibiotic prescribing for acute cough included confusion (delirium) (aOR 6.8), cough (aOR 3.7), wheeze (aOR 3.2), shortness of breath (aOR 2.9), sputum production (aOR 2.7), feeling unwell (aOR 1.9) and muscle pain (aOR 1.6).12 38 For patients with diarrhoea, presence of abdominal pain increased odds of antibiotic prescribing (aOR 7.6), as did taking antibiotics prior to consulting with a hospital physician (aOR 4.07).34
Physicians’ knowledge, skills and training
Healthcare providers’ knowledge and skills were identified as important factors in antibiotic prescribing.17 Doctors having a higher academic degree compared with an undergraduate degree (b 0.08 v 0.18 p=0.03), and being an internist compared with a surgeon or obstetrician (b 0.06 v 0.16 p=0.30 or 0.21 p=0.014) were associated with a lower level of antibiotic prescribing.37 A lower level of clinical competency in village practitioners compared with paediatricians, including a lack of knowledge of the association between the length of treatment and antibiotic resistance, the meaning of AMR,15 and the correct treatments for children39 was associated with a higher level of antibiotic prescribing.35 Village practitioners acknowledged they were unsure about prescribing antibiotics for very young children (under 3 years) in respect to dose and type of antibiotics to use.39 Uncertainty of treatment coupled with more severe illness in children resulted in village practitioners referring children to county or township hospitals.35 39 Other factors related to differences in healthcare providers’ antibiotic prescribing practices included recency and extent of their medical training, their knowledge of the latest antibiotics and whether they felt they had adequate knowledge and skills to prescribe antibiotics correctly, particularly for children.15 17 18 35 The prescribing competency of physicians varied from hospitals to primary care.36
Interventions aimed at influencing physician antibiotic prescribing
Antibiotic-related training reduced the proportion of clinicians who prescribe antibiotics incorrectly for common cold (14% vs 29% in control).18 Within the hospital setting, clinical pharmacy services providing education and recommendations to physicians on antibiotic use influenced antibiotic prescribing,44 including a reduction in the rate of use of antibiotics from 100% to 7.3%.49
National guidelines and regulations on clinical use of antibiotics aimed at physicians, can be helpful in improving appropriate antibiotic prescribing.46–48 53 66 In one study, village practitioners highlighted an absence of authoritative national clinical prescribing guidelines.15 Since the National Guideline for Antimicrobial Use in Clinical Practice was launched in late 2004 antibiotic use has decreased. For instance, a study of five large children’s hospitals identified a 23% reduction in antibiotic use from 2005 to 2006.53
Complex antibiotic stewardship interventions that incorporated both guidelines and training for physicians indicated a positive influence on antibiotic practices,51 61 68 80 including a decrease in use of certain classes of antibiotics (ie, second and third-generation cephalosporins) and in antibiotic use overall in a paediatric intensive care units,80 as well as decreases in the percentage of antimicrobial prescriptions and the proportion of prescriptions containing restricted antimicrobials in hospital.68
Patients’ knowledge and expectations about antibiotics
Patients’ lack of knowledge about antibiotic use appeared to be a key factor influencing the inappropriate use of antibiotics in China.17 Patients who demonstrated better knowledge about the appropriate use of antibiotics and the association between antibiotic use and resistance were less likely to be prescribed antibiotics compared with patients who did not display strong antibiotic knowledge (aOR 0.47).32 38 Patients requested specific antibiotics from village practitioners if they had been prescribed them previously for similar symptoms, demonstrating the important influence of past experience on patients’ treatment expectations.85 In Hong Kong, patients who self-identified as usually seeking help from a TCM practitioner rather than a biomedical doctor were slightly more knowledgeable about antibiotics (average knowledge score of 4.1 vs 3.9), preferred doctors who rarely prescribed antibiotics (aOR 1.29) and were less likely to accept antibiotics from a biomedical doctor when offered (aOR 0.38).86 In contrast, while medical students’ antibiotics knowledge score was higher than non-medical students,87 88 they were significantly more likely to ask a doctor to prescribe antibiotics (19% vs 12%).87 Physicians often perceived pressure from patients to prescribe antibiotics,17 31 and this had a strong influence on prescribing: patients’ expectation (aOR 5.1), anticipation (aOR 5.1) and direct request (aOR 15.7).38
Only two studies concerned educating patients. One multicomponent antimicrobial stewardship intervention providing brief caregiver education indicated a significant absolute risk reduction of 29% in the antibiotic prescribing rate.61 Evidence from a systematic review on the impact of clinical pharmacy services, including delivery of education to outpatients and inpatients, showed some evidence of a positive influence on the appropriate use of antibiotics.44
External or environmental factors
The type and organisational structure of a health facility setting appears to influence antibiotic prescribing,18 40 such as in the difference in the proportion of prescriptions for common cold between county hospitals (47%), township (44%) and VCs (71%).18 Focus groups with directors of health institutions pointed to an extremely high antibiotic prescription rate, up to 80%–90%, at township and village level facilities compared with the national target of 20% set by China’s Ministry of Health.39 A change of governance structure in CHC (from hospital-affiliated model to a self-managed independent model) resulted in a significant decrease in antibiotic prescribing, including a 9.2% decrease in the proportion of patients receiving an antibiotic injection and a 7.3% decrease in the proportion receiving two or more antibiotics.74 Primary care practitioners working in the private, rather than public, sector had a higher odds of prescribing antibiotics (aOR 9.7).89
The following external factors were highlighted as barriers to effective antibiotic prescribing: limited access to diagnostic testing (blood tests and laboratory diagnostic and antibiotic sensitivity tests are not available in VCs),15 39 lack of ambulance transport between villages and townships, and patients being unable to afford costs of transportation and hospital care.35 Transportation was a specific problem in some villages during the rainy season when road travel becomes difficult .35 Other external barriers to improved antibiotic prescribing included poor quality health services, pressure from high workloads on doctors, and the lack of effective control and regulatory mechanisms on medicine.17
Several intervention studies identified reductions in antibiotic prescribing attributed to the impact of regulatory mechanisms at national level,17 46–50 66 78 81 or local level.68 70 75 77 For example, following the introduction of National Special Rectification Scheme on Clinical Use of Antibiotics in 2011, various antibiotic consumption measures in hospitals nationwide showed significant reductions including prophylactic use for type 1 incision operations,47 proportion of antibiotic use in inpatients,46 66 and outpatients,66 and defined daily doses per 100 inpatient days46; in addition to a significant decrease in annual antibiotic consumption from 2009 to 2013 in one individual hospital.48
Financial incentives
Financial influences on antibiotic prescribing include: drug sales as a source of income for hospitals and practitioners17 31 35 39; inducements from pharmaceutical companies15; patient’s insurance status17 40; and incentives/ gifts from patient to prescriber.33 A systematic review identified economic incentives as the most frequently mentioned factor (30% of 67 reviewed studies in China) influencing inappropriate drug use in China, including antibiotics.17 Health workers described financial incentives from pharmaceutical companies to prescribe antibiotics with profit splitting of the mark-up on drug sales.15 Village practitioners commented that to make a living they needed to supplement their low salaries with activities such as injections, which generated additional payment35 and they feared losing patients and associated income if they did not prescribe antibiotics.39 Conversely, an audit study found that gifts given by patients to physicians resulted in a reduced proportion of physicians prescribing antibiotics to patients (50%–33.8%).33 Another study found that the antibiotic prescribing rate dramatically increased from 10% to 55% when antibiotics were bought from hospital pharmacies rather than elsewhere (implying an internal financial incentive to prescribe), and further increased from 14% to 85% when coupled with patients requesting them.31
In addition to financial factors that directly influenced physicians’ prescribing behaviours, economic incentives at the health system level were also associated with antibiotic prescribing. Increased government health funding in China may be associated with improvements in doctors’ antibiotic prescribing behaviours; for example, the proportion of prescriptions containing antibiotics in urban CHC gradually decreased from 45% to 31% with the increase of government health funding between 2007 and 2011.45 Similarly, a change in health financing from a fee-for service to capitation with pay-for-performance system was associated with 15%–16% reductions in antibiotic prescriptions among THC and VCs, respectively.43 55 Patient insurance status was also a factor influencing antibiotic prescribing,17 40 65 76 with evidence that patients enrolled in the township applied cooperative medical scheme, compared with those who were not, were more likely to be prescribed antibiotics (OR=1.80).76
Adherence to antibiotic therapy
Seven descriptive studies identified influencing factors associated with compliance with antibiotic therapy (online supplemental file 3).85–87 90–93
Patient characteristics
In adult outpatients, one study found that a higher average antibiotic knowledge score among patients was associated with better adherence to antibiotic instructions (B=0.481),90 while in an international survey of antibiotic compliance, younger age was associated with non-compliance in China.92 Residents in Hong Kong noted that recovery before the end of full course and concerns about side-effects were the main reasons for non-compliance with the full antibiotic course,94 while being male, younger than 40 years old, having primary education or less, being in a low or middle income, and being a user of TCMs were associated with reduced likelihood of finishing a course of antibiotics (aOR 0.67).86 95 In parents and care givers of young children (0–7 years) a lower adherence to a prescribed antibiotic regimen was associated with being a parent, rather than being a grandparent or carer, and with parents being younger and better educated.91 A study among students found that medical students score more poorly on a composite score measuring appropriateness of antibiotic behaviour/practice than non-medical students.87
Self-medication with antibiotics
Nine descriptive studies identified factors associated with self-medicating with antibiotics in different populations including community members in Hong Kong,94 95 clinicians (primary care clinicians (general practitioners and pulmonologists),96 university students88 89 97 98 and parents of young children (online supplemental file 3).99 100
Studies of populations from mainland China living in Hong Kong found evidence of an association between lower levels of self-medication with antibiotics and an awareness of the potential harm of this practice (OR 0.47).95 Higher levels of self-medication were associated with having leftover antibiotics (aOR 6.03 among local-born; aOR 5.51 among recent immigrants),94 and recent immigration status (aOR 2.37). Hong Kong residents commented on how expensive it was to see a clinician and that buying antibiotics was less expensive and “worked fine”.95
Among parents and caregivers, factors influencing self-medication with antibiotics included: having a family member in the healthcare profession (aOR 1.38)100; having child health insurance (aOR 1.30); caregiver having a positive attitude towards self-medicating children (aOR 2.66); being a female carer (aOR 1.25); storing antibiotics at home (aOR 2.79/6.25)99 100; (29, 22) living in a rural location (aOR 1.64)99; (29) raising more than one child (aOR 2.17); purchasing antibiotics without prescription (aOR 6.26) and higher age of the child (aOR 1.15). In contrast, factors associated with not self-medicating with antibiotics included: knowledge that antibiotics should only be sold with a prescription (aOR 0.77)100 and good adherence to physician’s advice (aOR 0.64).99
Sale of antibiotics without a prescription
Only one descriptive study was identified, a cross-sectional survey that aimed to identify factors associated with the sale of antibiotics without prescription (online supplemental file 3).42 This study sampled urban community pharmacies in three cities across China and focused on the sale of antibiotics for two discrete problems, paediatric diarrhoea and adult respiratory problems. Sale of antibiotics without a prescription varied significantly by city, with proportions reported as 58%, 37% and 74% in the case of paediatric diarrhoea and 61%, 81% and 96% in adult respiratory problems in Nanjing, Changsha and Xi’an, respectively. The proportion of inappropriate antibiotic sales was lower in pharmacies where a licensed pharmacist was present (34% vs 60%).
Discussion
Between 2003 and 2018, there was an increase in the number of studies on key influences on antibiotic use in China published in English language journals. This scoping review identified 31 descriptive studies (quantitative and qualitative) and 44 intervention studies. The increase in the latter study type, particularly between 2014 and 2015, may reflect the introduction of widescale antibiotic policy and healthcare reforms in China95; over half of the interventions evaluated were national policy guidelines with before-and-after designs. A small number were RCTs/cluster RCTs, none of which included qualitative or mixed-method process evaluations.
In general, higher rates of antibiotic prescribing were associated with more severe clinical presentation, lower levels of clinical training (both antibiotic specific and general), patient preference for antibiotic treatment, lower level of the healthcare system or private health facilities, and financial incentives built into the system. Antibiotics were sold without prescription by community retail pharmacies but sales without a prescription were lower in those pharmacies with a licensed pharmacist on site. Self-medication with antibiotics was widespread among the studies and higher rates of self-medication were associated with greater access (health professional relative, supply of left-over antibiotics, health insurance, higher income), populations where higher antibiotic use was the norm (rural, medical students, mainland China vs Hong Kong), preference for antibiotic treatment, and low awareness of the potential harms, such as antibiotic resistance, from excessive antibiotic use.
There is evidence that the introduction of policies to reduce the overuse of antibiotics in China may have had a positive impact. Reforms to China’s rural healthcare provision and 15% mark-up policy introduced new mechanisms for compensation for village and higher-level hospital health practitioners including user fees, especially from drug sale revenues,101 which contributed to overprescribing and prescribing of expensive drugs by health practitioners.102 103 With more recent National Essential Medicines and Zero Mark-up policies that removed these financial incentives, our review indicates a decrease in the proportion of prescriptions containing antibiotics at both national and local levels. Similar financial policies, such as pay-for performance, that separate practitioners’ income from drug sales have also led to reductions in antibiotic prescribing in the UK and Taiwan.104 105 However, government efforts to restrict the use of antibiotics in China have not dealt with the issue of low pay for village practitioners who experience pressure to subsidise their income. Indirect financial incentives remain that include additional compensation for clinical services, including administration of intravenous antibiotics which are frequently prescribed by village practitioners.
Higher rates of antibiotic prescribing were associated with less clinical training, lower-level health facilities and rural areas. These factors are linked as rural areas are served by VCs, which are staffed by practitioners who have more limited training than hospital doctors and may not possess a medical degree and have limited access to diagnostic testing.12 In China, most qualified health practitioners are concentrated in large hospitals and urban areas, with lower-level township hospitals in the more rural areas usually staffed with practitioners with the more limited training.106 This review found evidence that antibiotic focused training for clinicians was associated with reduced errors and reduced prescribing rates.39 44 55 56 63 71 73 78 Antibiotic prescribing training or guideline introduction are common components of successful antimicrobial stewardship interventions in clinical settings in low-income and middle-income countries (LMIC).107 108 However, the effectiveness of clinically specific guidelines or training may be reduced if the practitioners themselves have a very limited medical education. These inherent weaknesses in the rural primary care system in China contribute to the problem of overuse of antibiotics and may constrain the impact of national guidelines.12
Patient preference or expectation for antibiotic treatment was associated with higher antibiotic prescribing rates and with higher rates of self-medication. Patient expectations (perceived and actual) of antibiotic treatment is a known influence on antibiotic prescribing.109–111 Evidence-based educational interventions directed at changing patient knowledge, beliefs and attitudes towards antibiotics can reduce antibiotic treatment expectations, but it is not clear whether patient education can affect antibiotic prescribing in the absence of an intervention aimed at clinicians.112 Patient beliefs about when antibiotic treatment is needed are based on experiences of being prescribed antibiotics for certain symptoms, and the way in which clinicians link antibiotic prescription to these symptoms in the clinical encounter.113 114 High rates of antibiotic prescribing create expectations of antibiotic treatment, practitioners’ anticipation of patient antibiotic expectations mean antibiotics are more likely to be prescribed, thus creating a positive feedback loop that supports a norm of high antibiotic use.19 This review found evidence that higher rates of antibiotic prescribing were seen in populations where norms of high antibiotic use might be expected, such as in rural areas18 88 99 and in patients who usually attend biomedical rather than TCM practitioners.86 95 In order to reduce patient antibiotic expectations as well as practitioner willingness to pre-empt such expectations by prescribing antibiotics, particularly within areas or populations where high use is the norm, interventions that target both patient beliefs and clinician prescribing are needed.
Self-medication with antibiotics, bought from retail pharmacies or obtained from family and friends, is common across LMICs,115 even when prohibited by law.116 This review found evidence of higher rates of self-medication by medical students,87 88 which may seem counter-intuitive, since their medical education might be expected to lead to more appropriate use. Higher use of antibiotics has been observed in university students studying a range of clinical sciences.115 It may be that students undergoing biomedical training have a positive attitude towards antibiotics, perhaps viewing them as safe and effective, which may be a more important influence than knowledge of clinical guidance on use. Self-medication with antibiotics is higher in LMICs where health systems are weaker and people purchase antibiotics from retail pharmacies because they are more accessible than formal healthcare services.115 The sale of antibiotics without prescription was prohibited in China in 2003 and the National Action Plan to Curb Bacterial Resistance 2016–2020117 introduced a series of educational and monitoring initiatives aimed at reducing non-prescription antibiotic sales. Such multifaceted interventions are likely to be more effective, particularly if they target both pharmacy workers and customers.118
Strengths and limitations
The scoping review design facilitated the inclusion of a wide range of evidence using varied study designs. This enabled a comprehensive summary of the extent and nature of the evidence base concerning influences on antibiotic use in China. A limitation of the scoping review method is that a quality assessment of the evidence was not conducted. Hence, we are not able to comment on the robustness of the evidence reported here. A further limitation is that the review used English search terms and searched databases of literature published predominantly in English, which means that evidence published only in Chinese will not have been included in this review.
Gaps in the literature
The evidence base is dominated by studies with relatively weak designs (observational or before and after intervention studies), which focus mainly on secondary and tertiary level hospital settings. Many of the interventions evaluated were policies or guidelines and there may have been differences in the way these are interpreted and implemented at provincial, city, town, and village healthcare level, but none of the intervention studies had integrated process evaluations, so there is no evidence on variation in implementation or effectiveness. None of the studies explicitly used behavioural theory to develop interventions, although the influences on antibiotic use and prescribing behaviours are complex and operate at multiple levels.23 105 The lack of evidence regarding the impacts of national policy interventions on antibiotic use at a rural level is linked to a lack of reliable surveillance data from rural primary care.119 Although, national surveillance systems exist, such as the China Antimicrobial Resistance Surveillance System and Centre for Antibacterial Surveillance, that provide national standardised data on AMR and the clinical use of antibiotics, most data come from tertiary hospitals. Similar gaps in the evidence have been found for evaluations of antibiotic stewardship programmes in LMICs and from Asia at the rural hospital and community level.96 97
Conclusions
This scoping review has described the extent, nature and characteristics of the primary research on the influences on antibiotic use in China. The results of this scoping review highlight key gaps in the evidence and can inform future research directions.
For instance, although evidence suggests that China’s legislative reforms aimed at reducing the overuse of antibiotics are having some positive effects, all of the supporting evidence emanates from urban healthcare contexts and evidence of their impact at the rural health facility level is lacking and therefore urgently required. This is particularly important as we found evidence that inequalities within the Chinese health system relating to context, including inadequately trained village practitioners, low-quality care in rural areas,12 106 120 and poor accessibility to urban healthcare, appear to interact to drive high antibiotic prescribing rates. Thus, within the rural context, high antibiotic use is the norm and fuelled by widespread self-medication with antibiotics, often purchased without prescription from retail pharmacies. As evidence suggests that the drivers of inappropriate antibiotic use in China are multifaceted increased knowledge of this context is required in order design and deliver effective antimicrobial stewardship programmes. In urban contexts where evidence exists there is a need for more robust evaluations.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Annegret_S, @HelenSLambert
Contributors AS, PK, RF, HL, DW, IO, SM and CCo contributed to the conception or design of the work and CC, AS, PK, CCa and TZ were involved in the acquisition, analysis, or interpretation of data. CMo, TZ and CCa were involved in drafting the manuscript and AS, PK, RF, HL, DW, IO, SM and CCo critically revised the manuscript. All authors gave final approval of the submitted manuscript, and all authors agreed to be accountable for all aspects of the work,with CCa acting as guarantor.
Funding Newton Fund (UKRI and NSFC) the National Natural Science Foundation of China (NSFC) supported this study under the UK-China AMR Partnership Initiative, grant number MR/P00756/1 and 81661138001. The funding source had no role in study design, analysis or in the decision to submit the manuscript for publication. CLC and IO and CMC acknowledge support from the NIHR Health Protection Research Unit in Evaluation of Interventions at the University of Bristol.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.