Article Text

Abstract
Introduction Given the burden of diabetes in ethnic minorities and emerging data on the efficacy of financial incentives in type 2 diabetes mellitus (T2DM), it is critical to examine the efficacy of financial incentives across and within racial/ethnic groups.
Methods and analysis This trial is an ongoing 5-year, randomised clinical trial designed to test the efficacy of a Financial Incentives And Nurse Coaching to Enhance Diabetes Outcomes (FINANCE-DM) intervention composed of (1) nurse education, (2) home telemonitoring and (3) structured financial incentives; compared with an active control group (nurse education and home telemonitoring alone). The study also will evaluate whether intervention effects are sustained 6 months after the financial incentives are withdrawn (ie, 18 months post-randomisation) and whether the intervention is differentially efficacious across racial/ethnic groups. Participants will include 450 adults with a clinical diagnosis of T2DM and HbA1c of 8% or higher who self-identify as White, African American or Hispanic. Participants will be randomised to one of two groups: the FINANCE intervention or Active Control. The location and setting of this study include primary care clinics at the Medical College of Wisconsin (MCW) in Milwaukee, WI and community partner sites affiliated with the Center for Advancing Population Science at MCW.
Ethics and dissemination This trial was approved by IRB at MCW under PRO00033788.
Trial registration number Registration for this trial on the United States National Institute of Health Clinical Trials Registry can be found under ID: NCT04203173 and online (https://clinicaltrials.gov/ct2/show/NCT04203173?id=NCT04203173&draw=2&rank=1).
- general diabetes
- education & training (see medical education & training)
- health economics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study includes use of a randomised controlled study design.
This study includes structured financial incentives combined with telephone-delivered nurse education and skills training and home telemonitoring.
This study includes a large sample size of 450 adults with poorly controlled type 2 diabetes.
This study includes diverse samples across socioeconomic and racial/ethnic groups.
This study is an ongoing clinical trial.
Introduction
Background and rationale
Diabetes mellitus affects more than 34 million adults in the USA.1 Ethnic minorities, specifically African Americans and Hispanics, with type 2 diabetes (T2DM) have higher prevalence of diabetes, poorer metabolic control, and greater risk for complications and death compared with White Americans.1 Evidence from the literature indicates that high-intensity interventions that incorporate multiple components are needed to improve clinical endpoints, especially in ethnic minorities.2–6 These high-intensity interventions typically combine education and skills training,7 8 home telemonitoring9–12 and nurse case management.8 13 Preliminary data from our group suggest that nurse education and home telemonitoring is effective in T2DM.14
Recent evidence from behavioural economics research supports the use of financial incentives to improve health-related behaviours. Effectiveness of financial incentives to improve health behaviours has been demonstrated across conditions and behaviours including smoking, weight loss, dietary behaviour, medication adherence and diabetes self-management, with the most beneficial result lasting up to 18 months post-intervention.15–20 Thus, the evidence in support of financial incentives in chronic disease management, thus far, is promising. Preliminary data from our group suggest that structured financial incentives layered on nurse diabetes education and home telemonitoring is feasible and effective in adults with T2DM.
However, there are three important unanswered questions in this field of research: (1) Are financial incentives layered on nurse education and home telemonitoring superior to nurse education and home telemonitoring alone in improving metabolic control long term? (2) Are the effects of financial incentives on metabolic control sustained once the incentives are withdrawn? (3) Are financial incentives efficacious within and consistent across racial/ethnic groups? This paper describes the rationale, study aims, and research design and methods of an ongoing 5-year, randomised clinical trial to test the efficacy of a Financial Incentives And Nurse Coaching to Enhance Diabetes Outcomes (FINANCE-DM) intervention composed of (1) nurse education, (2) home telemonitoring and (3) structured financial incentives; compared with an active control group (nurse education and home telemonitoring alone). The study also will evaluate whether intervention effects are sustained 6 months after the financial incentives are withdrawn (ie, 18 months post-randomisation) and whether the intervention is differentially efficacious across racial/ethnic groups.
Objectives
Primary aim 1
To test the efficacy of the FINANCE-DM Intervention on glycaemic control at 12 months (long-term effect) and 18 months (sustainability effect) for adults with poorly controlled T2DM (overall efficacy across combined racial/ethnic groups).
Primary aim 2
To test whether the effect of FINANCE-DM on glycaemic control at 12 and 18 months is consistent across three racial/ethnic groups (Whites, African Americans, Hispanics) and, if differential effect of the intervention is found, to estimate magnitude and direction of effect for the three racial/ethnic groups (efficacy within racial/ethnic groups).
Primary aim 3
To determine the cost-effectiveness of the FINANCE-DM intervention.
Secondary aim
To test the efficacy of the FINANCE-DM intervention on secondary endpoints including blood pressure (BP), low-density lipoprotein (LDL) cholesterol, quality of life (QoL) and self-care behaviours (diet, exercise and medication adherence) at 12 and 18 months.
Trial design
An equal number of patients from three racial/ethnic groups (150 Whites, 150 African Americans and 150 Hispanics; total sample of 450) will be randomised to FINANCE-DM intervention (n=225) or an active comparator group (n=225), so that within each racial/ethnic group, half (75 patients) will be randomised to the FINANCE-DM intervention group and the other half (75 patients) will be randomised to the active comparator group.
Methods: participants, interventions and outcomes
Study setting
The location and setting of this study include primary care clinics at the Medical College of Wisconsin (MCW) in Milwaukee, WI and community partner sites affiliated with the Center for Advancing Population Science (CAPS) at MCW. Additional settings include local health fairs, CAPS events and sponsored activities by organisations who serve the study’s target population.
Eligibility criteria
This study will include a total of 450 adults who are age 21 years or older with a clinical diagnosis of T2DM and HbA1c of ≥8% at the screening visit. Participants must self-identify as being White, African American, or Hispanic. Participants must also be willing to use the FORA telemonitoring system (Fora Care, 893 Patriot Drive, Suite D, Moorpark, CA 93021, USA) for 12 months and have access to a landline, ethernet or cellphone for FORA data uploads for the study period. In addition, all participants must be able to communicate in English.
Interventions
The FINANCE-DM intervention comprises (1) nurse education, (2) home telemonitoring and (3) structured financial incentives. For the nurse-delivered diabetes education and skills training, trained nurse educators deliver the manualised diabetes education and skills training intervention via telephone. Participants receive 8-weekly sessions of diabetes education and skills training and monthly booster sessions from months 3 to 12. Each session lasts for ~30 min and is composed of 15 min of a previously tested diabetes education intervention based on American Diabetes Association guidelines and 15 min of diabetes-tailored skills training intervention using motivational enhancement approaches.21 The skills training sessions stresses individualised problem-solving and self-monitoring strategies in adopting lifestyle modifications and is focused on four behaviours—physical activity, diet, medication adherence and glucose self-monitoring.
The telemonitoring system used in this study is the FORA 2-in-1 Telemonitoring System. We have used this system across multiple clinical trials.21–24 The FORA system is an inexpensive, off-the-shelf, state-of-the-art technology whereby a person/caregiver and a provider can communicate accurately on data needed for self-management of diabetes. The system is composed of an easy-to-operate 2-in-1 blood glucose and BP monitor that uploads results to a secure website via a modem. To support behavioural skills training, patients are assigned the FORA 2-in-1 Telehealth System and provided glucose test strips to allow testing at least once a day. The device automatically uploads readings to a secure server as they are performed. The nurse educators have access to the secure server to which the uploaded measurements are stored in real time. The glucose and BP readings are used to tailor and reinforce behaviour change during weekly telephone-delivered diabetes education and skills training sessions and subsequent booster sessions.
Participants receive detailed training on the use of the FORA system and how to problem-solve around common issues with home monitoring devices by the study nurse educators, serving as training and run-in period. We have identified common issues that patients experience with set-up and ongoing use of the system from our prior studies and incorporate that into the training process for participants. In addition, participants have a 2-week run-in period to familiarise themselves with the FORA system and work with study nurse educators to address connectivity issues and other concerns that may arise. After the initial 2-week run-in period, participants continue to have access to the nurses to address technology-related issues that arise.
In addition to nurse-delivered diabetes education and skills training, participants will receive high-frequency financial incentives based on the structure tested in our pilot randomised controlled trial. We weighed the option of rewarding individual behaviours or rewarding a clinical endpoint and decided to go with both for the following reasons: (1) the literature shows that achieving HbA1c targets requires changing key individual behaviours; (2) HbA1c is a clinical endpoint that cannot be manipulated by the patient; (3) there is a very strong link between HbA1c and hard endpoints (eg, complications and mortality); (4) HbA1c is the endpoint that is most likely to be paid for by insurers or employers.
The financial incentives intervention is designed to (1) target multiple behaviours that contribute to glycaemic control (ie, diet, physical activity, self-monitoring and medication adherence); (2) be given at a frequency that is consistent with expected change in HbA1c (ie, every 3 months); (3) be sufficiently large enough to motivate behaviour change, especially in ethnic minorities who tend to have lower health literacy, lower income and lower perceived self-efficacy for diabetes management; (4) reward more aggressive lowering of HbA1c to target (<7%); and (5) reward maintenance of targeted behaviours as indicated by maintenance of HbA1c levels at each post-baseline assessment point.
Participants will receive a reward for (1) uploading glucose measurements, (2) participating in telephone-delivered educational sessions and (3) achieving absolute percentage drops in HbA1c from baseline at each 3-month follow-up intervals as follows: each week, participants can receive up to US$10 for uploading glucose measurements and having good glucose control throughout the week. For each day they upload at least one glucose measurement, they will receive US$1 (up to US$7 at the end of the week). If they upload measurements every day of the week and their average glucose measurements at the end of the week are 150 or below, they will receive an additional US$3. Participants can receive up to US$10 per week for each 3-month period. Participants can also earn US$5 each week if they participate in the telephone-delivered educational session. Educational sessions will last for 8 weeks, so they can receive up to US$5 per week for 8 weeks. Participants can also earn US$5 for attending monthly booster sessions from months 3 to 12. After each 3-month interval, if their HbA1c has dropped 2% from baseline, or absolute HbA1c is <7%, they will receive a reward of US$130; for a 1% drop, or an absolute HbA1c between 7 and 8, they will receive a reward of US$65. Therefore, over the 12 months’ duration of the intervention, each participant can receive a maximum of US$520 for uploading daily glucose readings, US$85 for participating in telephone-delivered educational sessions, and US$520 for 2% absolute drop in HbA1c or maintaining HbA1c below 7%, for a maximum incentive of US$1125.
Patients randomised to the active comparator group are assigned the FORA 2-in-1 Telehealth System and provided glucose test strips to allow testing at least once a day. Blood glucose and BP are measured daily, and results are uploaded to a secure server. A nurse educator reviews the blood glucose and BP readings and use them to tailor and reinforce behaviour change during weekly telephone-delivered diabetes education and skills training session.
Outcomes
The primary outcome is glycaemic control (HbA1c) and cost measured at baseline, 3, 6, 9, 12, and 18 months post-randomisation with the primary time points at 12 and 18 months. Secondary outcomes include LDL cholesterol, QoL, BP and self-care behaviours measured at baseline, 3, 6, 9, 12, and 18 months post-randomisation with the primary time points at 12 and 18 months.
Sample size
For the overall comparison of intervention groups (aim 1), 180 patients per intervention group (60 per racial/ethnic group within each intervention) will provide 85% power to detect a 0.2SD standardised effect size (Cohen’s d) or equivalently a raw effect size of 0.4 percentage point in HbA1c. For aim 2 (consistency of intervention effect across racial/ethnic groups), with 60 participants per intervention-by-racial/ethnic group cell, there will be 85/80% power to detect a standardised effect size of 0.41/0.39SD (Cohen’s d) between pairwise racial/ethnic groups within each treatment. This standardised effect size is equivalent to a raw difference in HbA1c between racial/ethnic groups within each treatment (effect size) of 0.78/0.73 percentage points (assuming the SD for HbA1c=1.9 percentage points, based on pooled SD from previous studies).
Recruitment
Multiple complementary approaches are used to identify eligible study participants. The first method consists of systematic identification of adult patients with T2DM at MCW clinics (General Internal Medicine-GIM, Endocrine, Family Medicine). Using an IRB approval for a partial waiver of HIPAA, we will query clinic billing records over the previous 12-month period. Search criteria will include patient demographics and ICD-coded diagnosis to allow identification of subjects with ICD-10 codes consistent with a diagnosis of T2DM. In addition, recruitment in collaboration with community partners includes (1) recruitment letters and flyers, (2) social media, (3) local newspapers, (4) radio advertisements, (5) self-referral/word-of-mouth, and (6) bus and organisational advertisements.
Methods: assignment of interventions
A permuted block randomisation method is used to assign participants to one of the two intervention groups: (1) FINANCE-DM intervention and (2) Active Comparator. Block size varies to prevent selection bias and to protect blinding. The randomisation will be carried out separately for each racial/ethnic group, and additionally stratified by clinical site (MCW and Community), baseline HbA1c levels (8%–10% vs >10%) and income level (<US$50 000 vs US$50 000+). Using the Research Electronic Data Capture (REDCap), study staff collect eligibility information and enter the information into the study database via the secured study website. Once eligibility is confirmed, intervention assignment will be made by a pre-programmed randomisation scheme.
Methods: data collection, management and analysis
The study design, flow, data collection schedule, measures and instruments can be seen in figure 1, and tables 1 and 2, respectively.
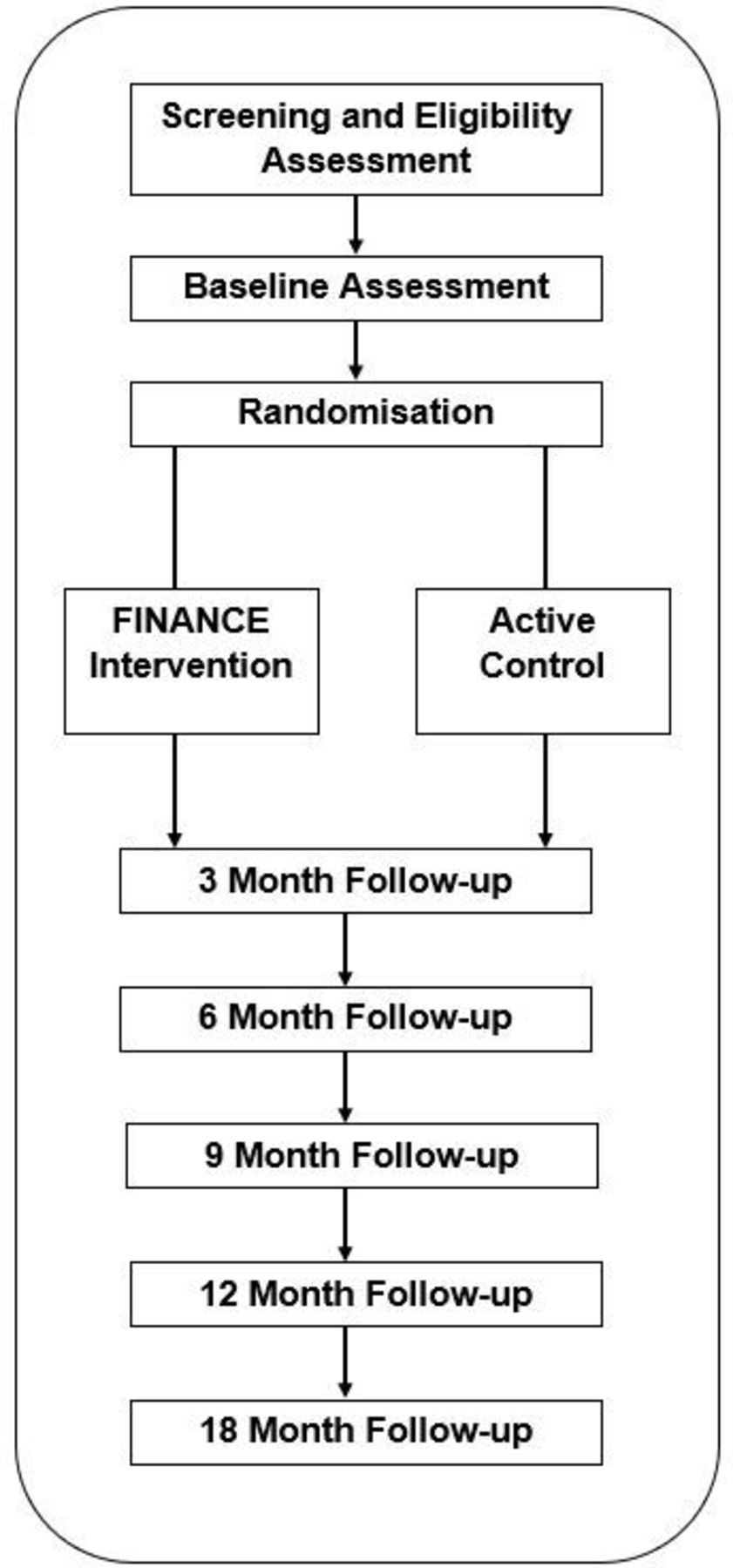
{kind=link}
Design and study flow.
Data collection schedule
Data collection measures
Analysis plan for primary aim 1 (overall intervention comparison)
A longitudinal mixed-model approach will be used with HbA1c as the dependent variable with intervention, time and time by intervention as the primary fixed independent variables, and racial/ethnic group (with appropriate corresponding intervention and time interactions), site and baseline HbA1c as covariables. The approach accommodates missing data under the missing at random (MAR) assumption, time-varying or invariant covariates, and can account for the correlated measurements within subjects. HbA1c least squares means (LSM) from the model will be compared for the intervention groups at the a priori specified primary end-of-study (12 and 18 months) time points and at secondary intermediate time points (3, 6 and 9 months) using p values for corresponding model contrasts. The magnitude and direction of the difference in HbA1c LSM between the two interventions (effect size) will be estimated using 95% CIs. The consistency of effect sizes (intervention differences) will be evaluated using the intervention-by-time interaction term. In additional secondary analyses for the primary aim, other adjustment covariables (eg, demographics, social support, health literacy, depression, medical comorbidity) will be added to the model if imbalance across intervention groups is found and the corresponding further adjusted LSM will be estimated and compared.
Analysis plan for primary aim 2 (differential efficacy of interventions between racial/ethnic groups)
The differential efficacy of the interventions on HbA1c across three racial/ethnic groups (Whites, African Americans, Hispanics) will be evaluated using the two-way and three-way interaction terms (intervention, race/ethnic group, time) in the model described for primary aim 1. The three-way interaction (time-by-(intervention-by-race/ethnic group)), if non-significant, will not be included in the final model and the two-way interaction, if significant, will indicate that the effect of the interventions on HbA1c is not consistent across the race/ethnic groups. The magnitude/direction of pairwise differences in HbA1c LSM between the three race/ethnicity groups within the interventions (and differences between the interventions within each race/ethnic group) at 12 and 18 months (effect sizes) will be determined using 95% CI from appropriate model contrasts.
Analysis plan for secondary aim
The secondary outcomes are systolic BP, LDL cholesterol, QoL (Short Form Survey (SF-12)), behavioural skills (Summary of Diabetes Self-Care Activities (SDSCA)) and medication adherence, and the primary time points are 12 and 18 months. We will use a generalised linear models (GLM) approach, which accommodates a wide range of distributional assumptions as the general analytical framework for inferential analyses for the secondary outcomes. The choice of appropriate GLM link function for each secondary outcome will be made after examining the observed distributions and model fit parameters prior to breaking the treatment masking. Each outcome will be used separately as the dependent variable in the model following a modelling process similar to that for primary aims 1–2, including evaluation of the differential effect of race/ethnicity on the relationship between intervention and outcomes through inclusion of appropriate race/ethnic group interactions in the model (as described in primary aim 2).
Analysis plan for primary aim 3 (cost and cost-effectiveness analyses)
Methods approved by WHO25 and the US Guidelines for Cost-Effectiveness Analysis26 to determine organisational and system costs and calculate cost-effectiveness will be used. Given the many sources of uncertainty, and our desire to obtain cost estimates that may be readily used by different stakeholders, we will conduct cost and cost-effectiveness analyses from provider, payer and patient perspectives. From the provider and payer perspective, we will calculate the total cost of the programme per participant using the resource cost method which includes personnel, overhead, supplies and equipment costs necessary to provide FINANCE-DM. From the payer perspective, we will estimate the cost of reimbursing the provider and providing incentives to the patient. From the patient perspective, we will calculate the patient’s time cost and cost associated with purchasing healthier foods and or engaging in healthier physical activities. Effectiveness will be measured based on changes in HbA1c, QoL (SF-12), quality-adjusted life years and patient productivity (working hours and income).
GLM estimation with appropriate distribution assumptions will be made based on the distribution of each of the clinical and economic outcomes. Adjusted marginal impact of FINANCE-DM for each clinical and economic outcome from each perspective will be ascertained by adjusting for patient sociodemographic, comorbidity and delay discounting characteristics. Adjusted marginal impact of FINANCE-DM from each perspective will be used to estimate separate incremental cost-effectiveness ratios for the provider, payer and patient. Bootstrapping procedures will be applied to obtain CIs around all our cost-effectiveness estimates.
Methods: monitoring
Nurse educators are all bachelors level trained and completed an intensive week-long training that included assigned readings, thorough orientation to study purpose and procedures, and protection of human subjects protocol. Supervision regarding adherence to intervention model is provided by a study co-investigator on a bi-weekly basis via teleconferencing. Fidelity ratings are completed on a weekly basis.
Methods: patient and public involvement
The development of the research question and outcome measures were informed by patients’ priorities, experience and preferences through a process of intervention mapping which included holding an informal focus group with a sample of patients from the local community. The investigative team presented a series of intervention strategies and designs; a round-table discussion took place to refine the intervention based on patients’ priorities, experience and preferences. The frequency of intervention calls were informed by patients based on the perceived burden. Patients also informed the intervention strategy by sharing their experience based on time, location and messaging. Results of this study will be presented and disseminated to study participants at a community forum where participants will be invited to learn about the findings and next steps.
References
Footnotes
Contributors LEE is the principal investigator and obtained funding for this grant. RW, JSW, RK, CED, TD and JAC made substantial contribution to the development of this protocol.
Funding This study is funded by grant number R01DK120861 from the National Institute of Diabetes and Digestive Kidney Disease. The authors would like to acknowledge other partial supported by the National Institute of Diabetes and Digestive Kidney Disease (K24DK093699, R01DK118038, PI: LEE), National Institute for Minority Health and Health Disparities (R01MD013826, PI: LEE/RW), and American Diabetes Association (1-19-JDF-075, PI: RW).
Disclaimer Funding organisations had no role in the analysis, interpretation of data or writing of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.