Article Text

Abstract
Objectives The prevalence of malnutrition after hospitalisation is reported to be 20%–45%, which may lead to adverse outcomes, as malnutrition increases the risk of complications, morbidity, mortality and loss of function. Improving the quality of nutritional treatment in hospitals and post-discharge is necessary, as hospital stays tend to be short. We aimed to identify and map studies that assess the effectiveness of individualised nutritional care plans to reduce malnutrition during hospitalisation and for the first 3 months post-discharge.
Design This was a systematic scoping review.
Methods We systematically searched for all types of studies in the following databases: EMBASE, MEDLINE via PubMed, and the Cumulative Index to Nursing and Allied Health Literature, with no restriction on data or publication language. We also reviewed the reference lists of the included studies. The abstracts and full articles were simultaneously screened by two independent reviewers. Differences of opinion were discussed among the two investigators, and a third reviewer assisted with the discussion until consensus was reached. Studies in which the patients received an individual nutritional care plan related to their hospital stay and were followed up post-discharge were included. We then conducted a thematic content analysis of the extracted literature.
Results Nine randomised controlled trial studies met the inclusion criteria: six were conducted in Scandinavian countries. All studies were mainly conducted among elderly patients (mean ages varied from 75 to 88 years). The review studies measured 10 different outcomes; the most common outcomes were nutritional status and readmission. Six studies reported one or more significant positive intervention effect. Inconsistent results were identified for four outcome variables.
Conclusions Individualised nutritional care plans and follow-up home visits might improve patients’ nutritional status. However, there is need for a systematic review that assesses study quality and extends the time to 6 months post-discharge.
- nutrition & dietetics
- health & safety
- quality in health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first scoping review to identify and map studies that assess the effectiveness of individualised nutritional care plans.
The evidence obtained from the included studies may help guide nutritional practice and future research.
There were no language restrictions in this review.
The search strategy was created by the research team, which included an experienced medical librarian.
Three months’ follow-up time may be insufficient, especially for determining whether an intervention can reduce the risk of readmission or mortality rates.
Introduction
Hospitals worldwide struggle to prevent malnutrition, especially among hospitalised older adults.1–4 Studies have reported the prevalence of malnutrition to be 20%–45% at the time of discharge.5–7 Incomplete nutrition treatment may adversely impact patients’ health outcomes, as malnutrition increases the risks of complications, loss of function, prolonged hospital stay, morbidity and mortality.6 8–12 Therefore, there is a need to improve the quality of nutritional treatment in hospitals.
Nutritional problems neither occur, nor are solved, overnight and caring for patients with multifaceted nutritional issues is considerably more complex than merely addressing a failure to eat. Providing nutritional care may include psychological, physical and social issues—such as dental problems, addiction, dementia, dysphagia, depression and loneliness—that affect patients’ appetites and ability to eat.13 Cooperation and communication among healthcare providers are important to ensure that patients receive proper and coordinated nutritional treatment and care.14 Individualised care acknowledges the uniqueness of the individual, and may improve the quality of nutritional care in cases of complex nutritional problems. One randomised controlled trial (RCT) study indicated that individualised nutritional treatment improves energy intake and the activities of daily living (ADLs) of older patients who had an acute stroke with malnutrition risk, as compared with a standard care group.15
The average length of stay in hospitals has declined since 2000 in most countries.16 The average length of stay in hospitals due to all causes among the 36 member countries of the Organisation for Economic Co-operation and Development was approximately 8 days in 2015.16 17 Shorter hospital stays have led to an increased need for nutrition treatment post-discharge to promote improvement in nutritional status—for example, energy intake and body mass index—to prevent complications and readmission.18–20 However, lack of continuity in care and poor communication have been identified as important risk factors for malnutrition.14 21 22
In 2012, a systematic review concluded that transitional care initialised in hospitals could yield positive outcomes among hospitalised adult patients.23 Another study revealed that dietetic care in hospitals was the most potent predictor of post-hospital care, although dietetic post-discharge care was conducted for only a few patients.24 Early and prolonged nutrition intervention can lead to better nutrition status and reduce length of hospital stays.25 Hospital-initiated care plans with follow-up by qualified healthcare providers post-discharge may be effective in improving nutritional status as well as reducing complications and decreasing readmission rates among aged patients.26 27 The advantages of nutritional intervention initiated during hospital stay may be missed if continuity of care is not adequately addressed when patients are discharged.
Therefore, individualised care plans with follow-ups could be an effective approach to improve nutritional care and may reduce malnutrition. This scoping review, unlike a previous systematic review,22 focused on individualised nutritional care plans and not individualised dietary counselling. We aimed to bring new insight concerning how individualised nutritional care plans with follow-ups can reduce malnutrition.
Individualised care plans are developed based on a detailed individual assessment of patients’ nutritional needs, conditions and desires.28 29 The individualised care plan includes patients’ nutritional status, individual nutritional treatment measures, dietary intake and requirements. The plan includes appropriate nutritional interventions, which are evaluated and adjusted according to changes in the patient’s situation and condition.26 Information about adjustment of physical, psychological and social factors that hinder appropriate dietary intake can also be added.29 A multidisciplinary team involved in the patient’s care design the nutritional care plan. This may include recommendations provided by dietitians, nurses, occupational therapists, midwives and the medical team; however, the recommendations are not limited to those from these professions.30 A nutrition care plan contains clearly documented nutrition interventions to achieve defined goals of treatment; these plans are revised continuously to assess their effectiveness and are adjusted, if needed, until the treatment goals are obtained.28–30
There is a need to map the research evidence on this topic. Systematic scoping reviews can be very useful for mapping research evidence and are frequently used to identify research gaps, clarify key concepts, and report on the types of evidence that address and inform practice in a research field.31 32
Aims
This study aimed to identify and map studies that assess the effectiveness of individualised nutritional care plans with follow-ups to reduce malnutrition during hospital stay and for the first 3 months post-discharge from the hospital. The particular research questions to be addressed were:
What types of individualised nutritional care plan interventions are addressed in the literature?
Which populations are studied?
What outcomes are measured in the studies?
Are these interventions effective?
If these interventions are effective, in what way are they effective?
Methods
A systematic scoping review methodology was employed, based on an a priori published protocol (see online supplemental file 1).33 Briefly, this scoping review was guided by Arksey and O’Malley’s framework,34 which was extended by Levac et al35 and the Joanna Briggs Institute.36 It adhered to the Extension for Scoping Reviews of Preferred Reporting Items for Systematic Reviews and Meta-Analyses: Checklist and Explanation.37
Supplemental material
Search strategy
The search strategy was created by the research team, which included an experienced medical librarian. As recommended by the Joanna Briggs Institute,36 a three-step search strategy was used in this review and published in the protocol.33 Literature search strategies were developed using medical subject headings browser and text words related to nutrition, individualised care plans and transitional care.33 EMBASE, MEDLINE via PubMed, and the Cumulative Index to Nursing and Allied Health Literature were searched in April 2019, and the search was updated in January 2020. Searches were performed with no language and date of publication restrictions. The databases were searched from the time of database inception. All reference lists of included articles were searched to identify additional studies. The reference lists of related reviews were also searched.
The criteria for inclusion in this study were adult patients of both sexes; aged ≥18 years; who received an individualised nutritional care plan. The nutritional care plan had to be written, obtained related to the patient’s hospital stay, and followed-up in the next 3 months post-discharge from the hospital surgical, medical or rehabilitation unit. There were no further requirements for the plans. All outcomes measured in the studies were of interest. This review considered studies involving patients who were discharged from any hospital, for up to 3 months post-discharge. In addition, we included studies lasting longer than 3 months if they reported results for up to 3 months post-discharge; when interventions lasted for more than 3 months, we included results only up to 3 months post-discharge.
Study selection and data abstraction
References from the literature search were imported to Covidence, an internet-based software program that facilitates screening, data extraction and collaboration among reviewers. The first and last authors independently screened the abstracts and titles according to the inclusion and exclusion criteria. The same two investigators independently assessed the full-text reports retrieved for potential inclusion. Differences of opinion were discussed, and a third reviewer assisted with discussions until consensus was reached. All data were independently charted from the included papers by the first and last authors. A standardised charting form was developed and aided in categorisation of the data.
This scoping review provides a narrative account of findings from the existing literature through thematic content analysis of the extracted literature. Multiple outputs from the same trial are reported according to the manner in which the original article reported them. Study quality assessment was not relevant, as the objective of a scoping review is to identify gaps in the literature and highlight future areas for systematic review.34 35
Results
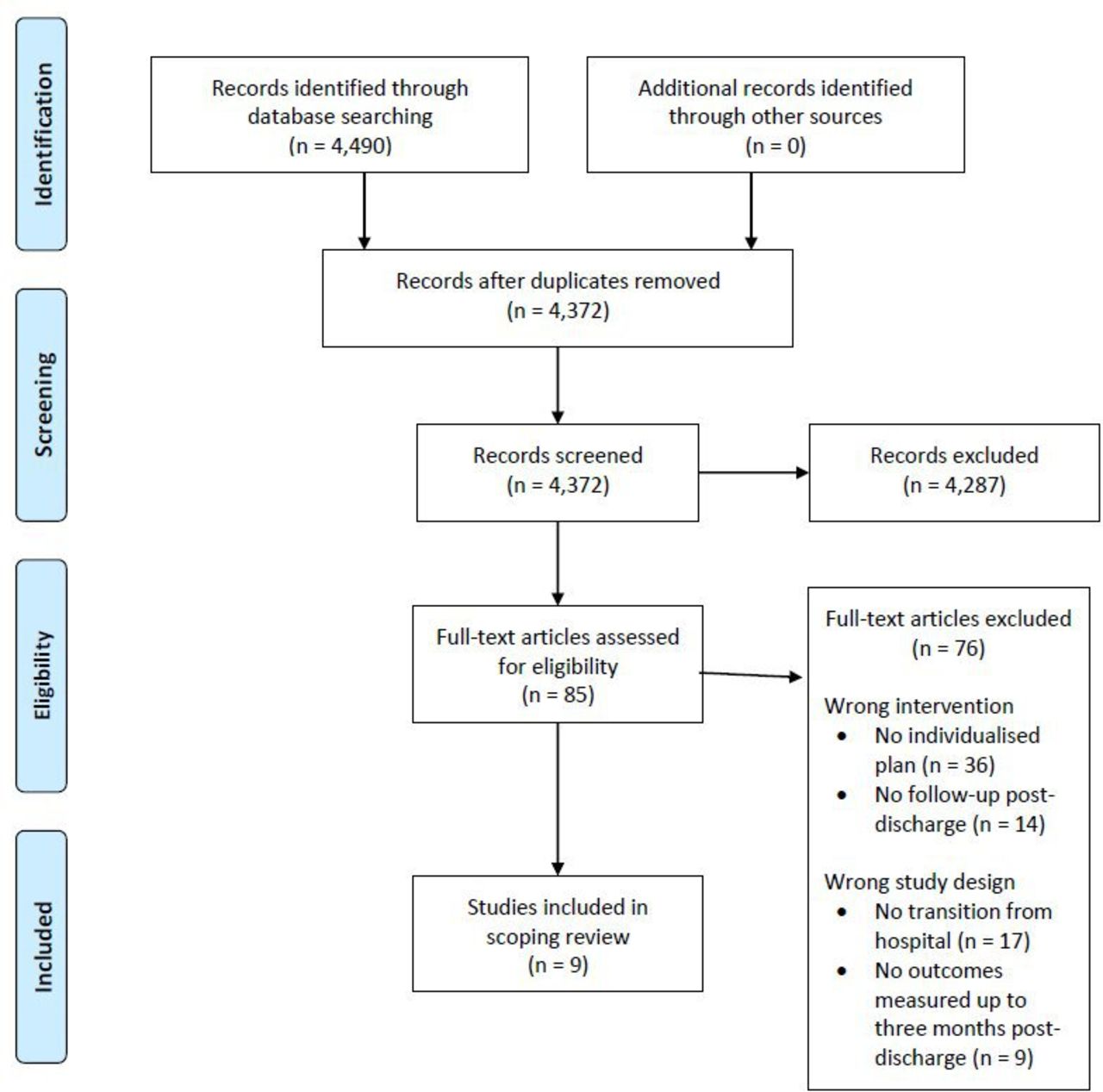
The study flow diagram (figure 1) indicates the 4490 citations resulting from the literature search. Eighty-five potentially eligible articles remained and were retrieved in full text, of which 76 were excluded based on the inclusion and exclusion criteria. This resulted in a total of nine RCTs that were included in this review.19 25 27 38–43 All types of study designs were searched; however, only these nine RCTs met all inclusion and exclusion criteria. Reasons for article exclusion were primarily due to inappropriate study population (ie, no transition from the hospital); other reasons included inappropriate intervention (ie, the study did not include an individualised nutritional care plan or the study did not entail any post-discharge follow-up). The intervention in two studies lasted for more than 3 months40 43; only the results up to 3 months were included in this study.
{kind=link}
Study flow diagram (http://www.prisma-statement.org) for the scoping review process, from Moher et al (2009).46
Here, the data from the studies are presented and discussed concerning the overall concepts/components related to the effectiveness of individualised nutritional care plans for adults during hospital stay and the first 3 months post-discharge. The results are presented in full in tables 1–3.
Description of included studies (N=9), ordered alphabetically
Description of the individual nutritional care plans in the included studies and the follow-up post-discharge from hospital
Outcomes measured in the studies and the intervention effects
Characteristics of the included studies
Five of the included studies were from Denmark,19 27 38 41 42 one was from Norway,39 one was from Israel,40 one was from Australia25 and one was from Taiwan.43 The studies were conducted between 2011 and 2019. Sample sizes ranged from 71 to 259, and participants’ mean ages varied from 75 to 88 years. Pedersen et al27 41 published two articles, both originating from the same trial. Beck et al19 38 also published two articles, originating from different trials. Eight studies involved patients aged >60 years, and one study included patients aged ≥18 years.39 The mean age across all nine studies was ≥75 years.
Nutritional care plan intervention
The individual nutritional care plans had a variety of characteristics and were performed by different professions in different settings. The plan was designed either in the hospital25 27 39–43 or after the patient was discharged home.19 39 The care plan was designed by a clinical nutritionist,39 dietitian,19 38 40 42 43 clinical nurse specialist27 41 or ward dietitian,25 in all cases together with the patient. The studies entailed two,19 25 three27 40–42 or four38 39 follow-up visits. One study did not report the number of follow-ups.43 The visits were performed either by home visit,19 38 40 42 a telephone call,25 43 both home visit and telephone call,39 or a home visit for intervention group 1 and a telephone call for intervention group 2.27 41 The follow-ups were conducted by dietitians (sometimes together with municipality care/general practitioners),19 25 38 40 43 clinical dietitians,27 41 or, in combination, municipality care and geriatric hospital nurses.42 One study39 did not report who was responsible for the follow-ups. The individualised care plans were all developed based on an individual assessment of patients’ nutritional needs, conditions and desires. The main characteristics of the nutritional care plans are provided in table 2.
Outcomes and effect of interventions
The studies measured 10 different outcomes (table 3). Eight studies measured nutritional status,19 25 38–43 such as appetite, body mass index, dietary intake and weight. Five studies measured re/hospitalisation19 25 27 38 42 or both rehospitalisation and changes in length of hospital stay. Four studies measured ADLs,19 38 41 42 including feeding, transfer, grooming, using the toilet, bathing, walking, climbing stairs, dressing, and bowel and bladder control. Four studies measured physical performance19 38 41 42; for example, mobility, gait speed, muscle strength, handgrip strength, chair-stand, disability, and tiredness in daily activities, rehabilitation capacity and Cumulated Ambulation Score. Quality of life was measured in four studies.19 25 39 41 Two studies measured the need for social services19 38 —need for home care, home nursing and meals-on-wheels. One study measured depression,41 one study measured complications during hospitalisation25 and one study measured self-rated health.42 Three studies measured one outcome up to 3 months post-discharge,27 40 43 one study measured two outcomes39 and five studies measured ≥four outcomes.19 25 38 41 42 Seven studies19 25 27 38 41–43 reported one or more significant positive effects of the intervention. The effectiveness of the interventions is shown in table 3.
Discussion
To the best of our knowledge, this is the first scoping review to identify and map studies that assess the effectiveness of individualised nutritional care plans. The search strategy aimed to locate all study designs; however, only nine RCTs met the inclusion criteria. The dearth of studies on such a common topic may be due to several factors. Nutritional counselling may be more common than preparing nutritional care plans. Also, nutritional care plans may be prepared in the hospital but not followed up post-discharge, which was an inclusion criterion for this review.
All the studies mainly included geriatric patients at nutritional risk, and only one study focused on a particular diagnosis.43 All RCTs except one43 entailed samples that comprised mostly women. Four studies had geographical restrictions,25 38 39 42 which might have led to the exclusion of rural patients. Six of the nine included studies were performed in Scandinavian countries,19 27 38 39 41 42 which might reflect the long tradition of focusing on person-oriented care in Scandinavia.44 User participation and patient perspective are among the cornerstones of the Nordic model and approach to healthcare provision,45 which might lead to more individualised care in Scandinavia.
The reviewed studies revealed that individualised nutritional care plans were based on individual needs and requirements, although the content of the individualised plans somewhat differed. In addition, to meet patients’ nutritional needs, the individualised nutritional plan might include/consider meals-on-wheels19 27 38 41; economic factors, such as inexpensive food sources and recipes40; and oral nutritional supplements (ONSs).19 25 27 38 40–42 Patients’ nutritional problems and constraints are complex. Aged people are heterogeneous regarding health status, prognosis, nutritional needs, physiological resources, preferences, individual goals29 and economic status. The included studies considered diverse aspects of patients’ situations when individualised nutritional care plans were performed. Additionally, the studies entailed different follow-ups. The observed effects of the interventions might be due to the type of follow-ups and/or content of the plans.
As noted, the reviewed studies measured 10 different outcomes. Most studies measured nutritional status19 25 38–43 and re/hospitalisation.19 25 27 38 42 A research gap was reflected in the lack of studies measuring cognitive outcomes. This review did not find any unambiguous answer to the research questions regarding whether interventions were effective and in what way they were effective. Specifically, four studies indicated that the intervention had a significant effect on nutritional status,19 38 42 43 and four studies demonstrated that the intervention did not.25 39–41 One study showed that the intervention had a significant effect on ADLs in one intervention group,41 and three studies did not.19 38 42 One study revealed a significant effect on physical performance,38 and three studies showed no such effect.19 41 42 One study showed significant effect on readmission,27 and four studies showed no such effect.19 25 38 42 All four studies that measured mortality19 25 38 42 reported non-significant results, which may indicate that individual nutritional care plans do not reduce mortality. However, we did not include studies in which the intervention lasted longer than 3 months post-discharge; to reduce mortality, interventions may need to last longer than 3 months.
In sum, this review yielded ambiguous results concerning four outcomes, which need to be further investigated. The different results, and whether they are significant, may be due to assessment tools, the number of participants or the study design.
We argue that there is a need for a systematic review and, if possible, a meta-analysis on this subject, and one that assesses study quality. We suggest the following potential hypothesis for a future systematic review: individualised nutritional care plans can reduce malnutrition during hospitalisation and up to 6 months post-discharge from hospital. The use of ONSs was important for the effect of an individualised plan.
Limitations
A limitation of this study may be the time limit—up to 3 months post-discharge. The lack of an outcome effect may be because the interventions were too short to provide any evidence of improvement. Three months’ follow-up time may be insufficient for determining whether an intervention can reduce the risk of readmission or mortality rates.
Conclusion
No uniform definition of an individualised nutritional care plan was used in the studies. The individualised care plans were all developed based on an individual assessment of patients’ nutritional needs, conditions and desires; although, the content of the individualised plans differed somewhat. In addition, to meet patients’ nutritional needs, the individualised nutritional plan might include ONSs; meals-on-wheels and economic factors, such as inexpensive food sources and recipes. Our results suggest that individualised nutritional care plans and follow-up home visits may improve patients’ nutritional status. However, only nine papers were included and these measured 10 different outcomes. This does not lend strength to any of the outcomes. This scoping review can inform future research; there remains a need for a systematic review to assess study quality and extend the time to 6 months post-discharge.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KI developed the research questions and methods and contributed substantially to drafting and editing. LU contributed to the methods, and edited and provided feedback throughout the writing process. IGK provided feedback throughout the writing process. CS and PP contributed to the development of the search strategy. PP contributed to developing the research questions and was a major contributor in review analysis. All authors read and approved the final version of this manuscript.
Funding KI, LU and IGK received funding from the Faculty of Nursing and Health Sciences, Nord University. CS and PP received funding from Aalborg University Hospital.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study. All data were obtained from publicly available materials.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.