Article Text

Abstract
Introduction Few studies have assessed the efficacy of smoking cessation interventions in individuals with type 2 diabetes, but interventions adapted to the specific needs of this population are warranted. The aim of this study is to assess the efficacy of a smoking cessation intervention in a population of smokers with type 2 diabetes and to measure the metabolic impact of smoking cessation.
Methods and analysis The study is an open-label, randomised control trial. Participants recruited from a sanitary region of Switzerland will be randomly allocated to either the intervention or the control arm. The intervention group will have four individual counselling sessions over 12 weeks. Trained research nurses will conduct the behavioural intervention, using motivational interviews and addressing diabetes and gender specificities. The control group will have one short counselling session at baseline and will be given written information on smoking cessation. Both groups will have a follow-up visit at 26 and 52 weeks. Demographic and medical data will be collected at baseline and follow-up, along with blood and urine samples. The primary study outcome is continuous smoking abstinence validated by expired-air carbon monoxide from week 12 to week 52. Secondary study outcomes are continuous and 7-day point prevalence smoking abstinence at 12 and 26 weeks; change in motivation to quit and cigarette consumption; and change in glycosylated haemoglobin levels, body weight, waist circumference and renal function after smoking cessation. In a subsample of 80 participants, change in stool microbiota from baseline will be measured at 3, 8 and 26 weeks after smoking cessation.
Ethics and dissemination Ethical approval has been obtained by the competent ethics committee (Commission cantonale d’éthique de la recherche sur l’être humain, CER-VD 2017–00812). The results of the study will be disseminated through publications in peer-reviewed journals and conference presentations.
Trial registration numbers ClinicalTrials.gov NCT03426423 and SNCTP000002762; Pre-results.
- diabetes & endocrinology
- general medicine (see internal medicine)
- preventive medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Smokers with various degrees of motivation to quit (including smokers not motivated to quit) are included with few exclusion criteria to ensure high external validity and thus clinical generalisability.
The 12-month follow-up will assess the long-term efficacy of the behavioural smoking cessation intervention.
The smoking cessation intervention is tailored to diabetes and gender specificities.
The smoking cessation intervention is compared with usual care; thus, participants in the control group might benefit from other interventions that may contaminate the control group.
As a result of group heterogeneity and few exclusion criteria, there is a higher risk of attrition.
Introduction
Smoking is the leading cause of avoidable death worldwide and among the top five causes of morbidity and decreased disability-adjusted life-years.1 More than a quarter of the Swiss population currently smokes cigarettes.2 Similarly, diabetes is a major public health problem and its burden is increasing globally.3 In Switzerland, it is estimated that about 450 000 people have diabetes, more than 90% of them having type 2.3 Smoking increases the risk of developing type 2 diabetes, and people with type 1 and type 2 diabetes who smoke are at increased risk of complications and premature death.4–6 Avoiding tobacco use could prevent a large proportion of cases of diabetes and its complications.7
Smoking prevalence and impact on people with diabetes
In those with diabetes, smoking has been repeatedly shown to increase the risk of mortality,8–12 as well as macrovascular complications such as coronary heart disease13–16 and stroke.17 Regarding microvascular complications, smoking has been shown to increase the risk of developing or worsening nephropathy, retinopathy18 and peripheral neuropathy.6
Despite the high rate of complications related to cigarette smoking, smoking prevalence remains high among people with diabetes.19–21
Smoking cessation in people with diabetes
It is a challenge for clinicians to induce a change in the behaviour of people with diabetes and to encourage a healthy lifestyle.22 Smokers with diabetes might differ from other smokers regarding not only their risks, but also their reasons for smoking and motivations to quit. Evidence suggests that they are less motivated to quit than other smokers, possibly because they fear weight gain.23 24 Smokers with diabetes are also more likely to have depression,23 25 a condition that has been shown to hinder efforts to stop smoking.26 In addition, they may be inadequately informed about the benefits of smoking cessation or available options to help them quit.27 28 These factors explain in part why success rates for smoking cessation are often low among people with diabetes.29 Most smokers with diabetes are not aware of the important risk of microvascular and macrovascular complications associated with smoking30 and often do not perceive smoking cessation as a top priority.31 32 Rather, diabetic smokers are most concerned about their weight, dietary adherence and diabetes management.33 Moreover, health professionals might be less prone to give smoking cessation advice to people with diabetes.27
Limited evidence is available on the effectiveness and efficacy of smoking cessation interventions in people with diabetes. Several studies have tested multifactorial interventions (which included smoking cessation in addition to other interventions such as physical activity) with various levels of intensity.34–38 Some studies showed an increase in smoking abstinence in participants who received multifactorial intervention,36 but the effect of smoking was difficult to isolate or the studies lacked power to show significant results when restricted to smokers.35
A systematic review and meta-analysis, published in 2014, summarised randomised control trial studies that assessed smoking cessation interventions among people with diabetes.39 In this review, which included four studies, smoking cessation rates at 6 months were variable, ranging from 0% to 18%, and the overall risk ratio of smoking cessation, which compared more intensive with less intensive smoking cessation interventions, was non-significant (risk ratio 1.32, 95% CI 0.23 to 7.43) using a random-effects model.
The few studies that have prospectively assessed the impact of smoking cessation on diabetes control and complications show contradictory findings. In a case control study from Japan that included 31 participants with type 2 diabetes, smoking cessation was associated with an increase in body weight (+1.2 kg), glycosylated haemoglobin (HbA1c) levels (+1 unit) and systolic and diastolic blood pressure at 12 months compared with continuing smoking.40 In contrast, in a 12-month observational study that included 193 participants with newly diagnosed type 2 diabetes, smoking cessation was associated with improvement in microalbuminuria, insulin resistance, and glycaemic control and with a reduction in peripheral vascular disease and polyneuropathy, but it had no effect on retinopathy.41 Chaturvedi et al showed that former smokers with diabetes had a lower risk of mortality than did continuing smokers, risk attenuation increasing with length of cessation.42 In a study that included men only, smoking cessation was estimated to be the best way to prolong life in people with diabetes compared with other interventions for reducing cardiovascular risk factors.43 Thus, smoking cessation is highly beneficial for long-term outcomes among diabetic patients, but little is known about short-term outcomes such as weight gain and diabetes control following smoking cessation.
Smoking, diabetes and microbiota
Studies recently reported modifications of intestinal and oral/nasopharyngeal microbial flora after smoking cessation in non-diabetic human subjects.44–46 It has been hypothesised that a change in the microbiota among non-diabetic smokers (a change to ‘obesogenic’ flora) after smoking cessation might partly explain weight gain.45 Fingerprinting of the microbiota has been studied in people with diabetes and compared with that in cardiovascular and control groups. The diabetes group showed a significantly increased proportion of aerobic bacteria, an increased proportion of coliforms, and a reduced proportion of bifidobacteria; the balance between beneficial and pathogenic bacteria was disturbed among those with diabetes.47 Moreover, the increased proportion of coliforms (with highly active lipopolysaccharide) and aerobic bacteria might result in an increased rate of intraluminal inflammation and dysbiosis, possibly leading in some susceptible persons to irritable colon syndrome or inflammatory bowel disease. The design of the studies that assessed the change in microbiota after smoking cessation and the limited number of subjects makes it difficult to generalise the results. Furthermore, no studies have prospectively assessed the impact of smoking cessation on the gut microbiota of subjects with type 2 diabetes.
Smoking, diabetes and gender
The prevalence of type 2 diabetes seems to be higher among men than among women.48 Risk factors for diabetes and complications seem also to differ between men and women, as diabetes confers a higher cardiovascular disease risk among women.49–51 Concerning diabetes process of care, women have better glycaemic control and adherence to recommended self-care than men do.52 However, women with diabetes are less likely to receive aspirin or antihypertensive or lipid-lowering drugs, and are treated less aggressively, thus gaining poorer control over their cardiovascular disease risk factors than men can.53–55
Despite an overall decrease in smoking prevalence over the past decades in high-income countries,56 the gap between men and women smokers has narrowed.57 Women have different reasons and motivations to smoke than men do.58 59 They are more likely to use cigarettes as a strategy to manage their weight and to cope with stress and emotions.58 60 61 Furthermore, women have different concerns associated with quitting, such as weight gain.62 63 They have a higher perceived risk of quitting and are more likely to relapse because of weight gain.64 65 It is, thus, important to take into account gender and diabetes specificities to better address barriers to quitting and to improve success in smoking cessation.
Smoking, diabetes, social stigma and depression
Recent research has shown that patients with type 2 diabetes experience social stigma, as diabetes is portrayed as the ‘blame and shame’ disease associated with bad lifestyle habits (nutrition, sedentary behaviour, smoking).66–69 Sources of diabetes-related social stigma include the media, healthcare professionals, friends, family and colleagues. Social epidemiologists have provided evidence on the effect of social stigma on psychosocial stress, leading to hypertension and other poor health outcomes.70 71 They are pleading for further studies to include both individual-level and structural-level measures of stigma and their effect on health outcomes. It is hypothesised that diabetes social support groups and motivational interviews can play a role in reducing the structural stigma experienced by diabetic persons, and thus its psychosocial effect on health.
In addition, the bidirectional association between diabetes and depression is well established.72 In fact, while depression is often perceived as a consequence of diabetes due to the burden of chronic illness, research has shown that depression may be a risk factor for the development of diabetes, explained by the biochemical changes and poor health-related behaviour in persons with depression.72 It is here hypothesised that the motivational interview, which includes a depression component, has an effect on diabetes self-care management on the one hand, and allows screening and appropriate referral in case of depression on the other.
Rationale for the study
In the latest US guidelines for treating tobacco use and dependence, the authors conclude that additional research is needed on counselling, cessation medications, and the impact and effectiveness of tailored interventions in individuals with diabetes.73 The purpose of the current study is to evaluate the efficacy of a smoking cessation intervention tailored to diabetes and gender needs among type 2 diabetic smokers. The secondary purpose is to measure and compare the metabolic consequences of smoking cessation and the influence of gut microbiota on metabolism among type 2 diabetics who successfully quit smoking and among those who continue to smoke. A substudy explores the relationship between social stigma, depression and diabetes self-care management.
Methods and analysis
Design
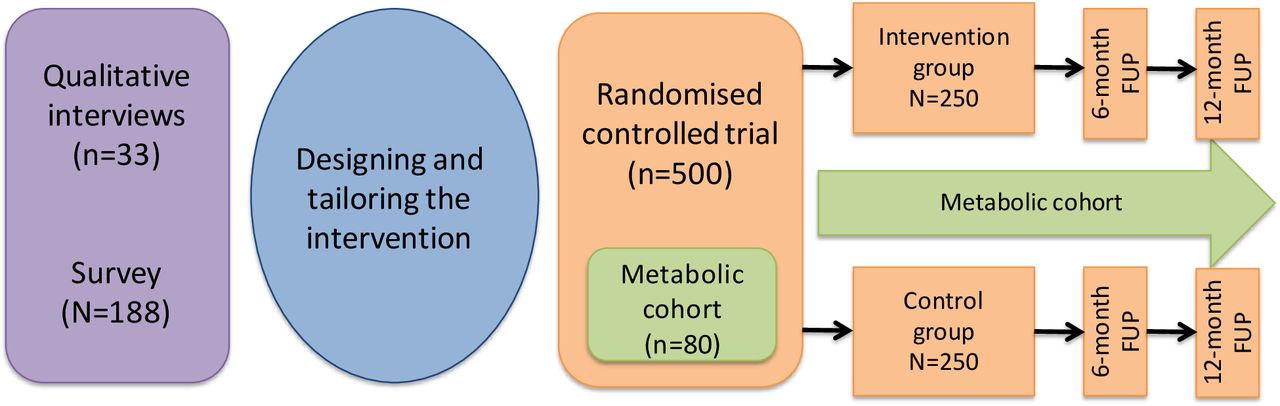
A total of 500 participants will be randomly assigned to either the intervention or the control group by using a computer-generated allocation method (orange area of figure 1). Allocation will be stratified by sex in order to obtain the same proportion of men and women in both groups.

Diabetes and Smoking Cessation: a Gender-Oriented Study (DISCGO). Study 3 phase design figure. FUP, follow-up.
Intervention
The intervention consists in behavioural smoking cessation. Combined pharmacotherapy and behavioural interventions have been shown to be effective in helping smokers to quit in the general population.73 74 For the present study, we will use an evidence-based smoking cessation intervention and tailor it to the participants from the findings of the previous phases of our study.75
The smoking cessation intervention will be standardised and follow Swiss and international guidelines.73 76 77 It will include both psychosocial support and evidenced-based pharmacotherapy treatment, which produce higher success rates when combined.74 78 79 Counselling will cover topics such as assessing ambivalence and enhancing motivation with motivational interviewing methods80 (using, eg, past successes in the field of smoking cessation or other lifestyle changes such as diet or physical activity), identifying barriers to quit (that are specific to people with diabetes, such as weight and diabetes management), coping with cravings and intensive relapse prevention strategies. Participants will be advised to use over-the-counter nicotine replacement therapy (NRT). A 2-week starting kit will be provided, consisting of a nicotine transdermal patch, and a short-acting NRT will be provided to participants for free.
The behavioural intervention will last 30–45 min and will be conducted by research nurses. These study nurses will take basic training in motivational interviewing (certified training of 4 sessions of 4 hours each). They will have an interview guide that will be flexible enough to adapt to the patient’s stage of motivation and preferences, as suggested by motivational interviewing techniques.
The intervention will follow the 5A steps, which is a well-described and systematic model currently being used in our smoking cessation outpatient clinic:
Ask for smoking status: The nurse will ask at each visit if the participant has smoked during the last 24 hours, the number of cigarettes (or other tobacco product) smoked, and the date of the last cigarette.
Assess motivations and need to quit: The nurse will assess the overall motivation to quit and the confidence to quit in the participants by using Likert scales from 1 to 10. She/he will also discuss with the participants their specific motivations to quit, as well as barriers and needs.
Advise about the possibility of smoking cessation and its benefits: The nurse will give information specific to diabetes that is adapted to the needs of the participants. This advice will be given by using recommended motivational interview techniques.
Assist the smoker to quit or decrease smoking by using a motivational interview±NRT: The nurse will then assist the participant to quit or change his/her cigarette consumption. No pressure will be put on smoking cessation, that is, no quit date will be fixed, unless the participant is ready and willing to quit, and every step towards a decrease in consumption will be encouraged. NRT will be systematically proposed to the participants in the intervention group who are willing to quit or decrease their consumption, but will be optional.
Arrange follow-up with the participant with 3 contacts of 30 min at weeks 3, 8 and 12, in which the nurse will again address smoking cessation by using the 5As approach, motivational interviewing and cognitive–behavioural techniques.
Control group
Participants assigned to the control group will receive a less intensive and non-tailored intervention for smoking cessation. For this arm the structured three steps ‘Ask, Advise, Refer’ or ‘AAR’ approach will be used: Ask for smoking status. Advise to quit in a clear manner. Refer to external help: participants will receive a booklet with written information on smoking cessation (non-specific to diabetes and gender) and links to support facilities (national quitline, smoking cessation clinic, websites, self-help). This unique intervention of 5–10 min will be performed by the research nurse.
Patient and public Involvement
This study, DISCGO-RCT (Diabetes and Smoking Cessation: a Gender-Oriented Randomised Controlled Trial) is the next phase of the DISCGO-MIX study (CER-VD project ID: 302/15, Swissethics ID PB_2016–01459) (purple area of figure 1; see also below for details), which is intended to define the beliefs, motivations and specific needs of diabetic smokers by using a mixed-methods approach.75 Using qualitative methods, we explored patients with diabetes and healthcare provider’s experiences and priorities. We adapted the intervention on the basis of their comments and preferences (eg, no interest in group sessions, desire for a motivational and ‘guilt-free’ approach). We did not discuss the design of the study with patients and did not include them in conducting the study. Nevertheless, we contacted patients’ associations to help us recruit participants and diffuse information. We plan to send the participants the main results individually by using a simple factsheet with pictograms. We did not assess the burden of the intervention by the patients themselves before the start of the study.
Sample size
Power calculations indicate that a sample size of approximately 400 people is needed for the primary endpoint, that is, to detect a 10% difference in smoking abstinence between the intervention and control groups at 52 weeks with a 2-sample proportions test by using Pearson’s χ2 test (power 80%, significance level 0.05). From previous studies in the general population, smoking cessation rates are around 5%–20% without interventions.45 If we hypothesise that smoking abstinence in the control group will be 10% at 12 months, an increase of 10% in the intervention group, that is, a 12-month smoking abstinence of 20%, would be considered clinically significant. We hypothesise a 20% attrition rate; therefore, the sample will be increased to 500 participants.
The analyses on the impact of smoking cessation on microbiota are exploratory and no sample size calculations have been performed. We will use a convenience sample of 80 participants (metabolic cohort).
Outcomes
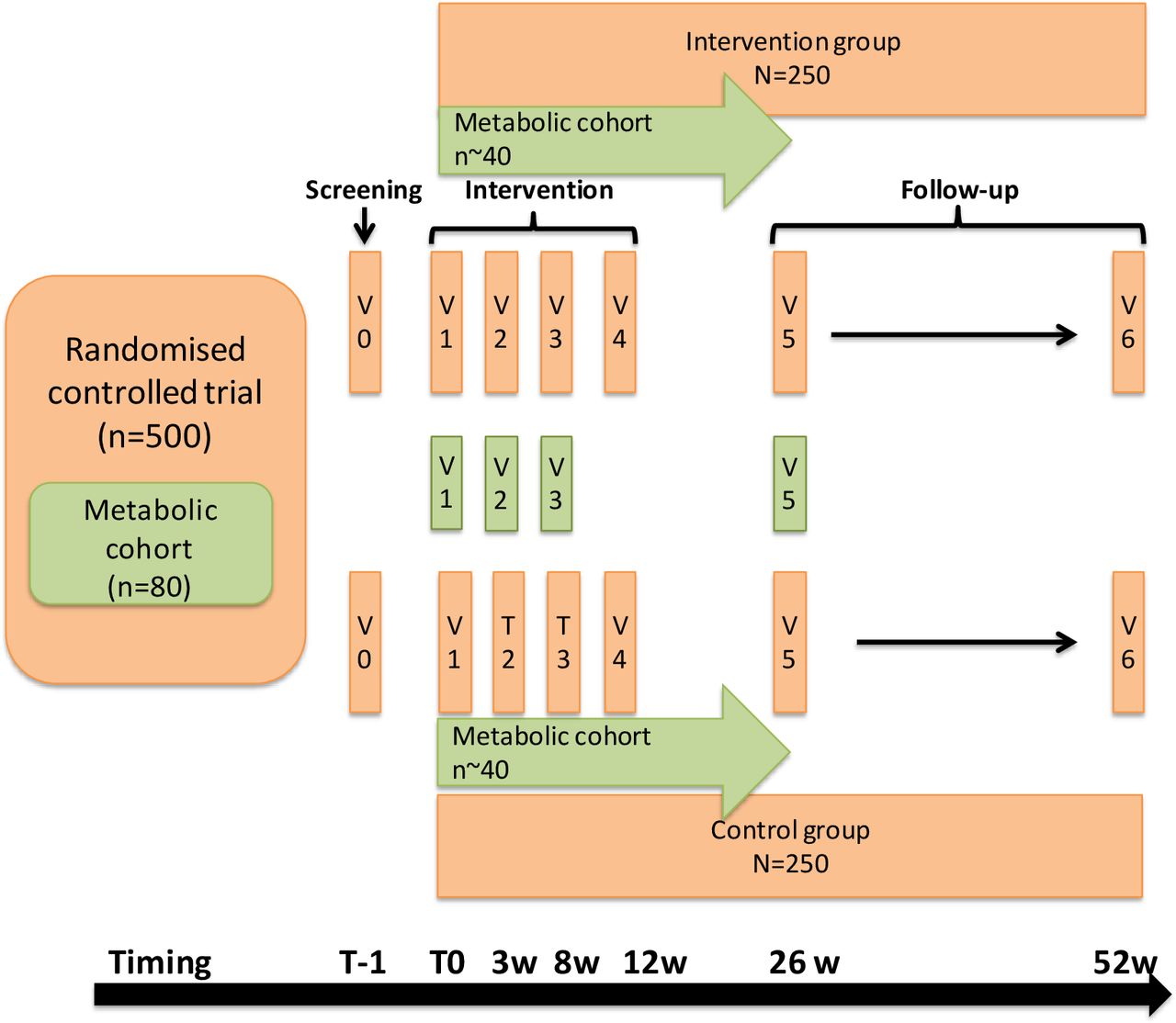
The primary outcome is to assess the efficacy of a personalised smoking cessation behavioural intervention compared with usual care on validated continuous smoking abstinence among type 2 diabetic smokers for up to 52 weeks (see below and figure 2). The study calendar, including all visits, measures and questionnaire details, is shown in table 1. Outcome measures are summarised in table 2.
{kind=link}
{kind=link}
Randomised controlled study design with nested microbiota study figure. V, visit.
Study questionnaire and procedures calendar
Study outcomes calendar
Smoking abstinence will be defined as a continuous abstinence rate from week 12 (end of intervention) to week 52 (end of follow-up), as recommended by the quality criteria for measuring smoking abstinence.81 Abstinence at each visit will be defined as a self-report of no smoking or use of other nicotine-containing products (electronic nicotine delivery system, smokeless tobacco) since the previous visit or contact, as confirmed by an expired carbon monoxide (CO) level of <10 ppm.81 82
The secondary outcomes for smoking cessation are as follows:
Continuous smoking abstinence validated by CO at 12 and 26 weeks.
7-day point prevalence abstinence validated by CO at 12, 26 and 52 weeks.
Change in motivation to quit and number of quit attempts from baseline to 12, 26 and 52 weeks.
Harm reduction (decrease of ≥50% of cigarette consumption) at 12, 26 and 52 weeks.
The secondary metabolic endpoints are as follows:
Change in body weight and waist circumference from baseline to 12, 26 and 52 weeks.
Change in HbA1c levels from baseline to 12, 26 and 52 weeks.
Change in renal function as assessed by the estimated glomerular filtration rate (eGFR) (Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) creatinine-based formula) and albumin/creatinine ratio from baseline to 12, 26 and 52 weeks.
The exploratory endpoint (metabolic cohort) is as follows:
Change in faecal microbiota from baseline to 3, 8 and 26 weeks. Different alpha and beta-diversity indexes will be used to characterise and compare the microbiota. Moreover, the rate of aerobic vs anaerobic bacteria, as well as the proportion of so-called beneficial gut bacteria such as species of Faecalibacterium and Akkermansia, will be compared between the different study groups.
The exploratory substudy on social stigma and depression will investigate the following:
Association between social stigma (using the Everyday Discrimination Scale (EDS))83 84 and diabetes self-care management (using the Summary of Diabetes Self-Care Activities (SDSCA))85 and between the EDS and HbA1c levels.
Association between depression (using the Patient Health Questionnaire for Depression (PHQ-9))86 and diabetes self-care management (using the SDSCA) and between the PHQ-9 and HbA1c levels.
Change in PHQ-9 score from baseline to 52 weeks.
Study population
Participants fulfilling all of the following inclusion criteria are eligible for the study:
Informed consent as documented by signature.
Having smoked >100 cigarettes during his/her entire life and currently smoking cigarettes (no minimal threshold).
Having been diagnosed with type 2 diabetes.
Being ≥18 years old.
Speaking and understanding French.
The presence of any one of the following exclusion criteria will lead to exclusion of the participant:
Not being able to give informed consent and to follow the study procedure (due to dementia, psychological disorder, language problem).
Being pregnant or breast feeding.
Being enrolled in another smoking cessation study or programme or in a multibehavioural programme that includes smoking cessation.
Enrolment of the investigator or other research collaborators, their family members, employees and other dependent persons.
Planning to move out of Switzerland within the next year.
Inclusion and exclusion criteria for the renal secondary outcome:
Same inclusion and exclusion criteria as above and,
CKD with Kidney Disease Improving Global Outcomes CKD stage G3-5 (eGFR <60 mL/min based on the formula CKD-EPI (creatinine)) and/or stage A3 (urinary albumin/creatinine ratio >30 mg/mmol on a urinary spot).
Recruitment and screening
Participants will be recruited from the Lausanne University outpatient clinics; medical or surgical wards (after discharge) of the Lausanne University Hospital; private practices of general internists and specialists in endocrinology from the region of Lausanne; the community via advertisements on selected websites, newspapers and social networks; pharmacies; and ambulatory centres from peripheral hospitals within a radius of 20–30 km around the investigation centre.
We will establish a list of all patients who have been admitted to the Lausanne University Hospital or outpatient clinic with a diagnosis of type 2 diabetes and a documented smoking status. Patients will be invited to participate to the study by letter. We will also post the information about study recruitment on the outpatient clinic website and on screens located in the waiting rooms. For participants recruited from pharmacies and private practices of generalists and/or specialists, flyers will be proactively distributed to potentially eligible patients by healthcare providers or local staff.
Analysis plan
Analyses for the primary outcome and secondary outcomes on smoking cessation will be done on an intention-to-treat basis. Participants lost to follow-up will be considered continuing smokers.
Primary analyses
Continuous smoking abstinence between weeks 12 and 52 will be compared between the intervention and the control group by using a Pearson χ2 test with a significance level of p<0.05. Analysis on the primary endpoint will be done by the research statistician, who will be blind to study groups. Similar analyses will be performed for other smoking cessation outcomes.
Stratified analyses for sex will be performed, with a χ2 test for analysing association between intervention and smoking cessation outcomes separately for each sex.
A logistic model for all smoking cessation (dichotomous) outcomes will be performed. The last (equivalent to the χ2 test in the unadjusted case) will allow us to:
Adjust for the type of smoking cessation treatment or help used by participant and not included into the study programme (participants will be free to use any smoking cessation treatment or help).
Test the effect of the interaction between intervention and sex on smoking abstinence for all outcomes, in order to explore if the intervention acts differently for the two sexes on the chances to stop smoking.
A longitudinal (generalised estimating equation) model will be used to compare abstinence trajectories between control and intervention groups, also adjusting for sex.
Secondary analyses
For metabolic outcome analyses on the nested metabolic cohort, the data will be used as a cohort and comparisons will be made between smokers who have managed to quit and continuing smokers.
A change in HbA1c levels from baseline will be compared between quitters and continuing smokers at 6 and 12 months by using t-tests with a significance level of p<0.05 after verification of normality. Among quitters, we will perform supplementary analyses creating subgroups of quitters according to time since quitting (long-term vs short-term quitters).
The prevalence of diabetes control, defined as HbA1c levels of <7%, will be compared between quitters and continuing smokers at 6 and 12 months. Stratified and adjusted analyses for sex will be performed to assess whether there is a differential metabolic impact of smoking cessation between men and women (interaction sex/smoking cessation in a logistic model for diabetes control).
We will assess the potential role of mediating factors in the association between smoking cessation and glycaemic control (HbA1c continuous) or diabetes control (HbA1c levels of <7%) such as weight gain, waist circumference and high-sensitivity C reactive protein. To assess the potential role of these mediating factors, we will enter them in turn in a logistic or linear models and evaluate their potential influence on the estimate (potential mediating effect if we observe a >10% change in the estimate).
Similar analyses will be performed for other laboratory variables (lipid profile, microalbuminuria, thyroid-stimulating hormone).
Descriptive statistics will be performed to compare changes in faecal microbiota from baseline to 4, 8 and 26 weeks between quitters and continuing smokers. Analyses will be adjusted for the intervention group, baseline body mass index, change in weight, waist circumference, age, sex, change in diabetes therapy and other treatments, and use of nicotine. In addition to the classic phylum-level analysis, we will also assess the impact of smoking cessation on diversity by using various indexes such as Shannon and on the presence or absence of various species-, genus- and family-level lineages. This analysis will first imply an assignment of the reads and then a subsequent description of the species, genus and family that are present in large amounts at baseline. A description of the variations of these specific species-level, genus-level and family-level lineages will then be assessed.
Substudy analyses
For the substudy, we will cross-sectionally (at w52) explore the association between social stigma (using EDS) and diabetes health outcomes (SDSCA and HbA1c levels), as well as between depression (PHQ-9) and the same health outcomes. To explore the hypothesis that social support may decrease social stigma, perceived stress and depression, and ultimately diabetes outcomes, we will further explore the path models between social support (diabetes support groups and/or motivational interview) and diabetes outcomes by using a structural equation modelling (SEM) approach87 (hypothetical model as online supplemental material). We will develop a theory-driven SEM model (path diagram) using the constructs represented by latent factors (eg, social stigma, SDSCA) based on the literature and hypotheses. We will then, in an exploratory step, use study data for model respecification and fit testing, ensuring meaning of items and factors is maintained and theoretically explained.
Supplemental material
Data management
Data will be collected by using electronic case record forms (Research Electronic Data Capture (REDCap) software) that will be securely stored for 10 years. Stata V.16.0 (StataCorp) and R (R Foundation for Statistical Computing, Vienna, Austria) will be used for statistical analyses.
Ethics and dissemination
Before the study started, the protocol, patient information and consent form, as well as other study-specific documents, were submitted to the appropriately constituted CEC (ie, Commission cantonale d’éthique de la recherche sur l’être humain du canton de Vaud, CER-VD), in agreement with local legal requirements, for formal approval. Approval was obtained on 28 December 2017. The study started in March 2018 and is ongoing. Any amendment to the protocol will be sent to the CEC for approval.
The study will be carried out in accordance with the protocol and with the principles in the current version of the Declaration of Helsinki,88 the guidelines of Good Clinical Practice issued by the International Conference on Harmonization,89 90 Swiss law91 and the requirements of the Swiss regulatory authority.92 93 The CEC will receive annual safety and interim reports and be informed about study stop/end in agreement with local requirements.
Risk-based monitoring will be performed by the Clinical Trial Unit, Lausanne (Switzerland).
The results of the study will be communicated and disseminated through conference presentations in national and international congresses of general internal medicine, endocrinology and tobacco research fields and through peer-reviewed manuscripts published in open-access journals. Depending on the results, we will propose implementing a smoking cessation intervention programme based on our model in diabetes clinics and in ambulatory care of our sanitary region (French part of Switzerland).
Acknowledgments
We thank the patients and healthcare providers for their help in the creation of this study and for providing us with their knowledge and valuable collaboration.Protocol version 5, 12.102019
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study concept and design: CC and JJP; Acquisition of data: AA, PB, JS; Draft of manuscript and statistical analysis: CC, AA, JS, PB, IL, AZ, GG, IJ-S and JJP; Revision of manuscript: All authors read and approved the manuscript for final publication. CC has the primary responsibility for the final content.
Funding This work was supported by a grant from the Swiss National Science Foundation (SNSF PZ00P3_154732) and a grant from the 'Fondation Pierre Mercier pour la Science', personally awarded to CC.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval has been obtained by the Competent Ethics Committee (CER-VD 2017-00812).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.