Article Text

Statistics from Altmetric.com
Although consensus has emerged from the clinical, social science, psychological, and biological literature that psychosocial factors affect asthma morbidity in children, their role in the genesis, incidence, and symptomatology of asthma remains controversial since mechanisms are not well understood. Three recent trends in medical research have led both clinicians and investigators to reconsider the role of psychosocial stress in asthma. Firstly, efforts to define the aetiological risk factors for the development and expression of disease have intensified in the face of rising trends in the prevalence and severity of asthma observed worldwide.1 Thus far, focus on traditional environmental risk factors has not fully explained these trends. Secondly, evidence evolved over the last two decades of important interactions among behavioural, neural, endocrine, and immune processes provides fresh insight into means by which psychosocial stressors may influence the development and expression of inflammatory diseases.2 3 This insight emerged in parallel with our increased understanding of the complex cellular and molecular basis of asthma as a chronic inflammatory disorder.4 Finally, hypotheses about the substantial role of the social environment and social integration in health and disease in general have gained significant emphasis over the last decade.5 6 In particular, prospective epidemiological studies have demonstrated associations between life stress, social position or status, and quality of social relationships—that is, social networks, an individual’s ties to friends, family, work, and community through social and religious groups—and health.6 7 All have led to a paradigm shift that reconsiders the overlap between biological determinates and psychosocial factors in understanding the rising asthma burden.8
This review highlights significant insights into this field from a multidisciplinary (psychoanalytical, behavioural, psychosocial, epidemiological, and immunological) perspective rather than being an exhaustive overview of the subject. We examine behavioural, neural, and immunological pathways, underscoring reciprocal relations that might link psychological factors to both the onset of asthma and exacerbation of established disease. We also focus on stress and psychological factors as indirect, albeit equally important, determinants of asthma morbidity—for example, by influencing how children and their families perceive and manage their asthma. Although no clear causal link between psychosocial stress and asthma has been established, this review provides a multidisciplinary transactional infrastructure that may guide future research priorities.
Historical perspective
The hypothesis of an association between stress and asthma emerges from a wide range of clinical observation and evolving research. The general concept of the role of emotion and the social environment in disease is as old as medicine itself. Early references to the importance of emotional and psychological processes were put forth in a treatise on asthma by Maimonides, an influential medieval Rabbi, philosopher, and physician.9 Sir William Osler referred to asthma as “a neurotic affection” in his medical textbook which served as a cornerstone of medical teaching in the latter part of the 19th century.10 Indeed, before we understood the inflammatory basis of asthma, it was among the disorders believed to be “purely” psychogenic in origin and was commonly referred to as asthma nervosa.
Scientific support for an association between psychological factors and asthma has its beginnings in the first part of the 20th century and derives from research in widely disparate fields. Early research suggesting that asthma had a psychosomatic component was strongly dominated by psychoanalytical theory, an extension of the Freudian idea that symptoms were a symbolic expression of unconscious conflicts and repressed desires.11 The so called specific emotion theory, developed in large part by Alexander and colleagues12 at the Chicago Institute of Psychoanalysis beginning in the 1930s, was among the most influential work of this era. Concurrently, learning theorists argued that particular emotional experiences may have reinforced pulmonary physiological responses, thus increasing the likelihood of them recurring in the same context.13 More recently, published clinical studies have demonstrated the benefit of psychotherapy in treating asthmatic patients,14 and relaxation techniques have been associated with improvement in respiration.15
Eventually, purely psychoanalytical and behavioural formulations gave way to physiological studies providing more objective support for the idea that emotions play an important role in asthma. Stress and psychological factors have been associated with asthma symptomatology16 and with bronchoconstriction and reduction in pulmonary flow rates in asthmatic children.17 When subjected to stressful experiences such as performing mental arithmetic tasks,18 watching emotionally charged films,19 and listening to stressful interactions,20 15–30% of asthmatic subjects respond with increased bronchoconstriction.
Taken together, these data clearly support an association with stress, although mechanisms linking stress and asthma remain poorly defined. To explore potential mechanisms linking stress and asthma, it is helpful first to consider how environmental and social stressors may influence disease in general and, second, to frame these hypotheses within the current asthma paradigm.
Life stress model
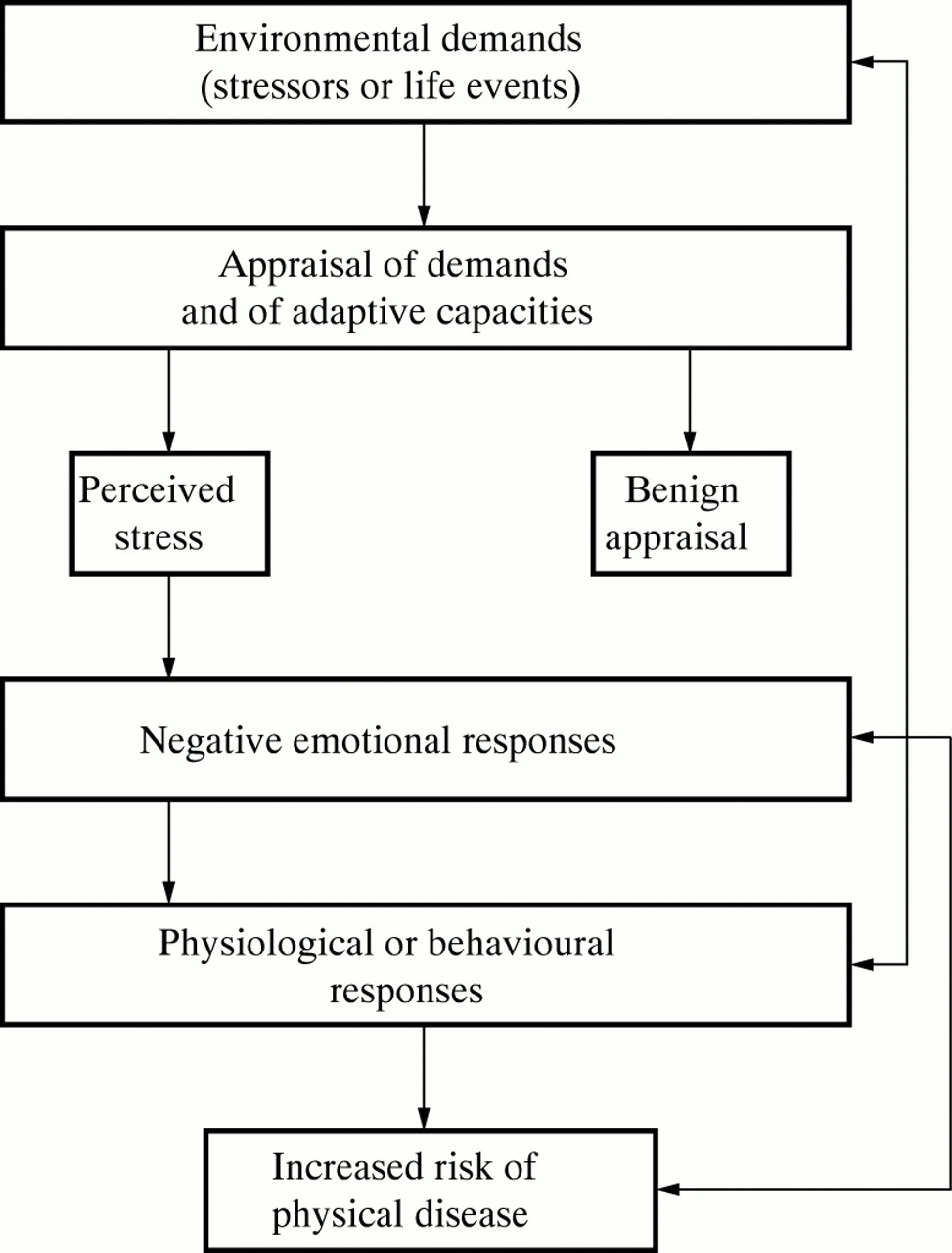
A general model of the link between environmental demands as psychological stressors and health is reproduced in fig 1. When confronting environmental demands, individuals cognitively appraise whether the event is threatening or potentially overwhelming to their existing coping resources.21 If environmental demands are found to be taxing or threatening, and at the same time coping resources are viewed to be inadequate, we perceive ourselves as being under stress. This perception is presumed to result in negative emotional states including fear, anger, anxiety, and depression. Changes in behavioural and emotional states that accompany the perception of, and the effort to adapt to, environmental circumstances are accompanied by complex patterns of neuroendocrine and immunological changes.22

{kind=link}
Biopsychosocial model of the stress process designed to illustrate the potential integration of the psychological and biological effects of environmental demands. Modified from reference22.
Both the duration and the frequency of experienced stress are important determinants of its impact on health and illness.22 23Psychological stress and its biological concomitants can last for a few minutes or for years. Chronicity is to some degree based on the ongoing presence of external stimuli that trigger the stress response—for example, ongoing unemployment, poverty, living in a dangerous environment—but is also dependent on the long term success of individual coping resources. Moreover, events that last a very short time can have very long term stress effects and lasting physiological responses thought to be maintained by recurrent “intrusive” thoughts about past events. Variable response to acute challenges superimposed on chronic stressors may have different implications on disease expression.24
Current asthma paradigm
Asthma is currently defined by the American Thoracic Society as a disease characterised by (1) airway obstruction that is, to a variable degree, reversible, either spontaneously or with treatment, (2) airway inflammation, and (3) increased airway responsiveness to a variety of stimuli.25 Key to recent advances in the field of asthma is an emerging understanding of asthma and allergic disease as chronic inflammatory processes regulated through complicated immune phenomena in which many cells (mast cells, eosinophils, and T lymphocytes) and associated cytokines play a part. Mechanisms of airway inflammation involve a cascade of events that include the release of immunological mediators triggered by both IgE dependent and independent mechanisms. Processes regulated through cytokines of the T helper cell (Th2 phenotype) such as interleukin (IL)-4, IL-5, and IL-13 are thought to promote recruitment of inflammatory cells which may initiate and/or potentiate allergic inflammation and the release of mediators that cause contraction of smooth muscle and influence mucus production.26 The leukotrienes (LTs), including LTC4, LTD4, and LTE4, are known potent constrictors of human airways,27 have been observed to play a part in mucus secretion,28 and are thought to have an important role in asthma. A substantial body of evidence supports the role of complex neural mechanisms and alterations of autonomic nervous system control in the pathophysiology and symptomatology of asthma.29 30Autonomic nerves can impact airway calibre and function via effects on airway smooth muscle, bronchial vessels, and mucus glands. Hormones and neuropeptides released into the circulation when individuals experience stress are also thought to be involved in regulating both inflammatory and airway responses.31 Therefore, consideration of recent advances in the field of psychoneuroimmunology—linking psychosocial stress, the central nervous system, and alterations in immune and endocrine function—provide plausible biological pathways through which stress may impact on asthma expression.32 33
Furthermore, self-management of disease is a cornerstone of current asthma guidelines.34 Poor self-management has been linked to poor asthma outcomes,35 and studies of mediators with a potential adverse impact on asthma management have drawn a great deal of attention. Indeed, the ability of the patient to adhere to a prescribed treatment regimen is viewed as one of the most important pathways through which many risk factors impact on asthma morbidity. Factors important to adherence include asthma knowledge, skills, and management behaviour.36 In addition, these variables are known to be affected by mental health (both adults and children), family functioning, social support, cognitive functioning, the personality and self-concept of the subject, and personal health beliefs and behaviours. Stress and coping may also influence health beliefs, health behaviour, social support, symptom perception, and adherence which, in turn, have an impact on asthma morbidity.
To simplify the discussion we have arbitrarily chosen to review the relations between stress, psychological dysfunction, endocrine function, neural function, immune function, social connectedness, and behaviour separately in order to explore the influence of environmental stress on asthma morbidity. We recognise that this is a rudimentary approach, as contemporary attempts to apply the biopsychosocial model to disease emphasise that a unidirectional model is too simplistic; causality is at least bidirectional or reciprocal and more probably cyclic in complexity.37
Psychological stress and the endocrine system
Psychological stressors have been associated with the activation of the sympathetic and adrenomedullary system and the hypothalamic- pituitary-adrenocortical (HPA) axis. These systems respond to psychological stress with increased output of adrenaline (epinephrine) and noradrenaline (norepinephrine) from the adrenal medulla.38 The hormonal responses of the HPA axis have long been thought to represent a non-specific physiological reaction to excessive stimulation,39 particularly the emotional arousal associated with appraising situations as stressful.40 The hypothalamus produces corticotrophin releasing hormone (CRH) which triggers the anterior pituitary gland to secrete adrenocorticotrophic hormone (ACTH), which in turn activates the adrenal cortex to secrete corticosteroids (primarily cortisol in humans). More recent work suggests that negative emotional responses disturb the regulation of the HPA system. For example, relatively pronounced HPA activation is common in depression with episodes of cortisol secretion being more frequent and of longer duration among depressed than among other psychiatric patients and normal subjects.41 Shifts in the circadian rhythm of cortisol have also been found among persons in stressful situations.42 Chronic stress may induce a state of hyporesponsiveness of the HPA axis whereby cortisol secretion is attenuated, leading to increased secretion of inflammatory cytokines typically counterregulated by cortisol. Some populations with post-traumatic stress disorder (PTSD), for example, have lower mean basal plasma cortisol levels throughout the circadian cycle and lower mean 24 hour urinary cortisol excretion.43 Furthermore, a state of stress induced HPA hyporesponsiveness in some research subjects has been associated with other inflammatory disorders.44 A hyporesponsive HPA axis may explain stress induced exacerbations of asthma in certain subgroups of asthmatics and increased association of asthma with particular psychological states.
Psychological stress activates the HPA axis resulting in the release of cortisol, which has known anti-inflammatory effects. However, other regulatory pituitary (i.e. corticotrophin) and hypothalamic hormones (i.e. CRH and arginine vasopressin (AVP)) of the HPA axis have systemic immunopotentiating and proinflammatory effects. Recently, Theohanides and colleagues have shown that acute psychological stress (immobilization in rats) results in skin mast cell degranulation, an effect inhibited by anti-CRH serum administered prior to stress.45
Although hormones of the sympathetic and adrenal medullary and HPA systems are those most often discussed as the biochemical substances involved in stress responses, alterations in a range of other hormones, neurotransmitters, and neuropeptides found in response to stress may also play a part in the health effects of stress. For example, stressor associated increases in growth hormone and prolactin secreted by the pituitary gland and in the natural opiate β-endorphins and enkephalins released in the brain are also thought to play a role in immune regulation.46
Psychological distress and asthma
Asthmatic subjects frequently have associated underlying psychological distress (depression and anxiety). Development of psychological distress in children has been associated with asthma that is more difficult to manage, requiring higher doses of steroids,47 more frequent and prolonged admissions to hospital,48 and greater functional disability.49 Asthmatics with comorbid psychological symptoms are more often non-compliant.50 Psychological morbidity has been linked to asthmatic mortality.51 52Mechanisms linking psychological morbidity and asthma morbidity and mortality are complex and remain largely undefined.
Asthmatic subjects have been characterised by β adrenergic hyporesponsiveness and α-adrenergic and cholinergic hyperresponsiveness.53 Defects in the function of the autonomic nervous system have also been demonstrated in psychological states including depression, PTSD, and psychomotor agitation.54-56 In depression and PTSD, studies of central mediators in the brain also demonstrate parasympathetic hyperresponsiveness and β adrenergic hyporesponsiveness.56 Whereas increased α adrenergic and cholinergic responsiveness distal from the airway has also been demonstrated in asthmatic patients,57 a similar imbalance to the autonomic nervous system in the central nervous system among asthmatic populations has not been demonstrated. These data raise the question of common biological pathways.
Stress and autonomic control of airways
The argument that psychological stress influences autonomic control of the airways is based primarily on the fact that many of the same autonomic mechanisms thought to play a role in asthma are involved in the activation and regulation of physiological responses to stress. These mechanisms include the release of sympathetic nervous system mediators and the action of adrenergic (sympathetic) and cholinergic (parasympathetic) nerves, and the neurotransmitters and neuropeptides they produce.
The parasympathetic nervous system innervates the airways via efferent fibres from the vagus nerve and synapse in ganglia in the airway wall with short postsynaptic fibres directly supplying the airway smooth muscle and submucosal glands.29 Increased activity of the parasympathetic nervous system was once thought to be the dominant mechanism responsible for the exaggerated reflex bronchoconstriction in asthmatic subjects, although more recent work challenges this idea.58 In the initial phases, narrowing of the airways in asthma is thought to result primarily from inflammation. Current theory holds that bronchial constriction is due to some combination of vagal input plus inflammation, with the relative importance of these factors being dependent upon genetic and environmental influences.
Recent experimental studies in which asthmatic patients are exposed to stressful situations have focused on stress induced vagal reactivity as a mediator of emotionally induced bronchoconstriction.16Preliminary evidence shows that children with asthma who respond to stressful stimuli with high vagal activation (associated with increased cholinergic activity) have greater impairment of airway reactivity in response to methacholine.19
Although human airway smooth muscle is not functionally innervated by adrenergic axons, studies have shown adrenergic innervation of submucosal glands, bronchial blood vessels, and airway ganglia.59 Adrenergic nerves may influence cholinergic neurotransmission via prejunctional α and β receptors.29 Depending on the type of agonist (β or α) involved, these changes can variably affect airway smooth muscle, release of inflammatory mediators, cholinergic neurotransmission, mucus secretion, and possibly mucociliary clearance, resulting in either bronchodilation or bronchoconstriction. Adrenoceptors are regulated by noradrenaline which is released locally from sympathetic nerves, and by adrenaline and noradrenaline secreted by the adrenal medulla. The regulatory effects of adrenaline and noradrenaline on adrenoceptors suggest a plausible mechanism by which stress induced activation of the sympathetic nervous system might influence bronchomotor tone.
It seems paradoxical that activation of the sympathetic nervous system by stress, resulting in release of mediators with a β agonist effect, should relax airway smooth muscle and that acute psychological stress, which is accompanied by a rapid increase in circulating catecholamines, should consequently cause bronchodilation. However, the stress induced response of the autonomic nervous system is more complex and variable. Once the acute stressor is terminated, levels of adrenaline and noradrenaline quickly return to normal or below normal.60 The relative strength of sympathetic versus parasympathetic control in response to certain forms of stress differs with the individual, with some showing a predominantly parasympathetic response. Such individuals may be particularly susceptible to stress induced bronchoconstriction.16 It is possible that sympathetic activation itself might contribute to asthma symptoms. For example, increases in circulating levels of adrenaline and noradrenaline are known to alter a number of immune parameters that might contribute to inflammation of the airways. Some evidence suggests long term increases or potentiation of the catecholamine response with chronic stress.23 Prolonged increases in catecholamine levels under chronic stress may also contribute to asthma severity. Chronic daily use of β agonists by mild to moderate asthmatics with a specific genetic predisposition may increase severity by downregulating β receptors,61 and it is possible that chronically increased stress induced catecholamines do the same among genetically susceptible subgroups. In addition, in those with chronic life stress the physiological response to acute stressors may result in more sustained effects on the immune system, even following sympathetic recovery.24
Collectively, these data showing that stress and psychological dysfunction have been associated with modulation of many of the hormones, neurotransmitters, and neuropeptides involved in autonomic control and inflammation of the airways (potential common biological mediators) suggest potential common underlying biological mechanisms. Further study of the “balance” among functional parasympathetic and functional sympathetic activity in relation to stress and emotional stimuli in asthmatic populations is needed.
Stress and immune function
A focus on the inflammation of the airways in asthma has drawn attention to the possibility that stress induced alterations in immune response have implications for development, exacerbation, and triggering of asthma.8 33 A substantial literature demonstrating that psychological stress can influence cell trafficking, cell function including mitogen stimulated blastogenesis and natural killer cell cytotoxicity, and lymphocyte production of cytokines has been recently reviewed.22 Stress can modulate immune response through nerve pathways connecting the autonomic nervous and immune systems, by triggering the release of hormones and neuropeptides that interact with immune cells, and through the impact on behaviours such as smoking and drinking alcohol that are adopted as ways of coping with stress.62
Subjects exposed to cognitive or social laboratory stressor tasks lasting only a few minutes show suppression of T cell mitogenesis and increased numbers of circulating T suppressor/cytotoxic (CD8) cells and natural killer cells.63 This phenomenon includes stress elicited alteration of the production of the cytokines IL-1β, IL-2, and IFNγ.64 65 These effects are thought to be mediated by the autonomic nervous system because they occur quite rapidly and have been shown to be associated with increased heart rate, blood pressure, and circulating catecholamines,66 and are blocked by administration of an adrenoceptor antagonist.67Living near the Three Mile Island nuclear power plant at the time of the accident, taking care of a relative with Alzheimer’s disease, and taking medical school examinations have all been shown to influence both the numbers and functions of various populations of lymphocytes.
Stress is not expected to have the same effects on immune function in all people. As noted earlier, individual differences in response to stressful events are attributable to interpretation of the event, access to coping resources, and presence of antecedent chronic stress. However, there is also evidence of stable individual differences in immune response that occur independent of psychological response to the stressor. When exposed to multiple acute laboratory stressors over time, some subjects consistently demonstrate stress elicited alterations in immunity, while others do not.68
As highlighted previously, airway inflammation and hyperresponsiveness are thought to be orchestrated by activated T lymphocytes and the cytokines they produce. The T helper cell Th2 cytokine phenotype promotes IgE production with subsequent recruitment of inflammatory cells that may initiate and/or potentiate allergic inflammation.69 Prospective seroepidemiological studies have shown that the newborn period is dominated by Th2 reactivity in response to allergens,70 and it is also evident that the Th1 memory cells selectively develop shortly after birth (at 3–6 months of age) and persist into adulthood in non-atopic subjects.71 For most children who become allergic or asthmatic, the polarisation of their immune system into an atopic phenotype probably occurs during early childhood.72
These findings have sparked off vigorous investigation into the potential influence of early life environmental risk factors for asthma and allergy on the maturation of the immune system, in the hopes of understanding which factors will potentiate (or protect from) this polarisation. For example, Martinez and colleagues73suggest that certain lower respiratory tract infections in early life (primarily croup) enhance the production of IFNγ by non-specifically stimulated lymphocytes, believed to be an expression of the Th1 phenotype. Although there is no direct evidence for the influence of stress on Th phenotype differentiation in the developing immune system, there is evidence that parental reports of life stress are associated with subsequent onset of wheezing in children between birth and one year.74 It has been speculated that stress triggers hormones in the early months of life which may influence Th2 cell predominance, perhaps through a direct influence of stress hormones on the production of cytokines that are thought to modulate the direction of differentiation. Simultaneous investigation of both host susceptibilty factors and the effect of environmental exposures, including psychosocial stressors, on the selection process for immunological memory may provide fresh insight into the pathogenesis of atopic disorders.
Stress and infection
The strongest suggestion from the current literature is that psychological stress may influence the pathophysiology of asthma by increasing the risk of respiratory infections. The role of respiratory tract infection in asthma is fairly well characterised with current evidence indicating that viral, as opposed to bacterial, infections are the most important infectious agents.75 Early life viral lower respiratory infections may be associated with an increased risk of developing asthma.76 Further evidence supports a more complex pathogenetic role for viral infections73 and suggests that the effects of infection may depend on which pathogen infects the host early in immune development.77
A number of mechanisms may be involved in explaining the exacerbation of asthma, especially wheezing and increased airway responsiveness, by viral respiratory infections. Firstly, viral respiratory infections damage the airway epithelium causing inflammation. Another mechanism involves the stimulation of virus specific IgE antibody. Respiratory syncytial and parainfluenza viruses may potentiate the allergic response to allergens by increasing the release of inflammatory mediators from mast cells and the subsequent cascade of inflammatory events characteristic of asthma.78Lastly, viral respiratory infections may also result in the appearance of a late asthmatic response to inhaled antigen.79 Thus there is evidence that viral infections are an “adjuvant” to the inflammatory response and promote the development of airway injury by enhancing airway inflammation.
A potential consequence of stress induced changes in immune response is suppression of host resistance to infectious agents, particularly agents that cause upper respiratory disease. The primary evidence for such effects comes from studies of psychological stress as a risk factor for respiratory infections. Increased incidence of upper respiratory infections under stress in these epidemiological studies may be attributable either to stress induced increases in exposure to infectious agents or to stress induced changes in host resistance. Control for exposure is provided by studies in which volunteers are intentionally exposed to a virus—that is, viral challenge trials. In these prospective studies psychological stress is assessed before volunteers are exposed to an upper respiratory virus and monitored in quarantine for infection and illness. Using this paradigm, psychological stress has been associated with the incidence of infection and illness,80 81 with increasing stress related in a dose response manner to increasing risk of infection.82
In summary, these data provide provocative evidence that stress is associated with reduced host resistance to respiratory infectious agents and implicates this as a possible causal mechanism in the stress-asthma paradigm.
Stress and social connectedness
Ecological views on health promotion underscore the significance of the social context within which individuals live and the importance of social relationships.83 In the study of social relationships and health, the former has been conceptualised in terms of social networks (a person centred web of social relationships) and social support (a measure of the functional content of these relationships). Lack of social relationships has been linked to an array of adverse health outcomes7 and physiological effects including altered immunological functioning.84Social support may reduce or buffer the deleterious effects of stress by altering the perception of a situation or facilitating more appropriate coping.85 Greater social network diversity has been related to less anxiety, depression, and non-specific psychological distress.86 Social supports may operate through influence on health promoting behaviours such as abstaining from cigarette smoking, moderating alcohol consumption, improving diet, exercise, and sleep quality.87 On the other hand, social support can be deleterious as well as health promoting. For example, support that encourages dependency may not have a positive impact.88 Parental attitudes that reflect exaggerated concern in protecting the child’s health89 and overdependency on medical support90 have been demonstrated, especially among severe asthmatic subjects.
For children the family as a support network has significant influence on chronic disease. Family function is an important correlate of health outcomes in general and this has been shown to be the case for asthma as well. The role of disturbed family interaction could be either direct by increasing the psychological stress in the child, or indirect by providing poor methods for coping with stress in the family system.91 Family structure is also an important correlate of health outcomes. Relationships between severity of illness and maladjustment vary significantly within different family structures.92 93 Many of the psychosocial factors implicated in the rise in asthma morbidity and mortality—for example, childhood anxiety and depression, noncompliance, family conflict94 95 —are dependent on family structure and function.
Social support/networks may buffer direct effects of stress on biological functioning and thus impact on asthma. For example, there is evidence that social networks influence the immune system and may play a role in susceptibility of the host to infection. Cohen and colleagues recently demonstrated an association of social ties with reduced susceptibility to the common cold, decreased mucus secretion, more effective ciliary clearance, and less viral shedding.96Furthermore, these authors found that susceptibility to colds decreased in a dose dependent manner with increasing diversity of their social networks.
Social support/networks may facilitate asthma management and general coping which, in turn, may enhance the asthma status and reduce disruptive effects of environmental stressors. Data from the Neighborhood Asthma Coalition (NAC), developed as a collaborative effort to promote community (neighbour to neighbour) support and encouragement of asthma management, more directly suggest that social isolation is important in asthma management and morbidity. These investigators found that children of socially isolated parents (those below the median on both support from family and from friends) were reported to have more frequent days/nights with asthma symptoms, more days of activity limitation, poorer asthma management practices, and more emergency department visits than those of non-isolated parents/care givers.97 Furthermore, subsequent interventions orchestrated through the NAC, which emphasises neighbourhood and community organisation strategies and social support to help asthmatic families, have resulted in reductions in acute care for asthmatic children.98
Future studies which examine the role of a broad range of social ties and diversity of social networks on disease expression and asthma management are needed to understand the influence of social connectedness in this field. Social support and social networks may impact on physical and mental health through various mechanisms. For example, social relationships can be examined as having a direct influence in the causal pathway or may be considered as a buffering system which impacts on the effects of environmental stressors.
Environmental stress and health behaviours
Because self-management is so critical in asthma care, it is important to consider how stress may affect self-management strategies and adherence to prescribed treatment plans. Social learning theory provides a useful model which examines the interaction among individuals, environments, and health behaviours.99Perceived control has been identified among factors that mediate the experience of chronic illness.100 There have been a number of conceptual approaches taken to the individual’s perceived control of his or her own behaviour. Popular among these have been self-efficacy, locus of control, and learned helplessness. Interactions between individuals and the environment are key to the development of perceived control. For example, the experience of positive consequences following task performance leads to self-efficacy.101Individuals repeatedly exposed to aversive events they cannot predict or control—for example, poverty, adverse life events, living in an unsafe or unpredictable environment—may learn to become helpless.102 Both perceived control103 and appraisals of self-efficacy104 are predictive of health outcomes. In animal studies there is evidence that controllable shocks have less deleterious effects on T cell functioning than uncontrollable shocks, which suggests that the controllability of stressors may be critical in modulating immune functioning.105Recently, Katz and colleagues106 have developed a disease specific brief Perceived Control of Asthma Questionnaire (PCAQ) (11 items) to examine the association of perceived control and asthma outcomes. They found that a lower PCAQ score was associated with an increased risk of admission to hospital and frequent activity restriction, which suggests that lower levels of perceived control are associated with more adverse outcomes in this population of adult asthmatic subjects. However, this was not a prospective study and therefore perceived control may have been influenced by the adverse events of the past year associated with the participant’s asthma, such as admission to hospital.
Although the major impact of psychological functioning on adherence has been shown in the context of other diseases,107 108 few studies have examined this issue in asthma. Christiaanse and co-workers109 examined compliance with theophylline therapy in asthmatic children and found that psychological adjustment and level of family conflict versus cohesiveness were predictive of compliance determined by mean theophylline levels. Most work to date has examined the role of family dysfunction in adherence to the medical regimen in asthma management.50 The relationship between stress, feelings of hoplessness or lack of control, and adherence with medical treatment remains virtually unexplored in the field of asthma research. The National Cooperative Inner City Asthma Study (NCICAS), a multicentre study, has launched an initiative designed to examine many domains including psychosocial stress, believed to be important to asthma morbidity, in order to guide more effective asthma intervention programmes in the inner city.110 A preliminary description of the psychosocial factors explored in this study has recently been published.111
Another critical premise of the self-management approach is the ability to identify accurately symptoms and pulmonary function compromise. It has been speculated that accuracy of perceived symptoms in paediatric asthma may be influenced by physiological factors such as disease severity as well as psychological factors such as defensive style, although empirical evidence is scarce.112 113Boxer and colleagues114 found a relationship between paediatric admissions to hospital for asthma and family dysfunction through the lack of symptom recognition and poor management of exacerbations.
As with previously discussed psychosocial factors, lack of perceived control and/or the environmental circumstances which lead to it may therefore act through two pathways. There may be direct effects on biological functions—for example, uncontrollable shock on T cells—or lack of perceived control may undermine symptom perception and disease management efforts.
Life stress, socioeconomic status, and race
In the USA asthma morbidity disproportionately impacts on poor urban minority populations.115 Efforts to identify factors related to these disparities are needed. The adverse association between poverty and ethnic minority status and asthma outcomes may in part be due to differential exposure to and perception of life stress as has been postulated for other health outcomes.116 In a recent review by Taylor and colleagues6 multiple characteristics of community, work, and family environments were considered which may lead to chronic stress in high risk groups. Some unique factors purported to cause chronic stress in communities of low socioeconomic status include poverty, minority ethnicity, the real or perceived threat of crime and violence, and poor transportation and refused services such as taxi and ambulance. Preliminary evidence suggests that exposure to violence is associated with the occurrence of asthma/wheeze syndromes and prescription bronchodilator use among inner city children.117 Frequency of adverse life events and level of perceived stress show an inverse relationship to socioeconomic status, while degree of perceived control and social support decrease as the socioeconomic gradient decreases.116 118 Pervasive life experiences such as racism and sexism may be important life stressors with health implications. Among minority populations, more attention is being given to the study of racism and sexism as stressors that impact on health status.119 120 While there is general consensus regarding the importance of the physical environment in asthma morbidity, the significance of such characteristics of the psychosocial environment has received little attention in asthma research.
Summary
Environmental stressors may impact asthma morbidity through neuroimmunological mechanisms which are adversely impacted and/or buffered by social networks, social support, and psychological functioning. In addition, life stress may impact on health beliefs and behaviours that may affect asthma management. Whereas earlier psychosomatic models have supported a role for psychological stress in contributing to variable asthma morbidity among those with existing disease, a growing appreciation of the interactions between behavioural, neural, endocrine, and immune processes suggest a role for these psychosocial factors in the genesis of asthma as well. While a causal link between stress and asthma has not been established, this review provides a framework in which we can begin to see links between these systems that might provide new insights to guide future explorations. The complexity of these interactions underscore the need for a multidisciplinary approach which combines the idea that the origin of asthma is purely psychogenic in nature with the antithetical consideration that the biological aspects are all important. These distinctions are artificial, and future research that synthesises biological, psychological, sociocultural, and family parameters is urgently needed to further our understanding of the rising burden of asthma.
Acknowledgments
During preparation of this manuscript Dr Wright was supported by a Deborah Munroe Noonan Memorial Fund, Medical Foundation grant. Dr Cohen was supported by a Senior Scientist Award from the National Institute of Mental Health (MH00721). The authors are indebted to the Fetzer Institute and their Psychosocial Factors in Asthma Working Group for the intellectual stimulation and support that led to the writing of this paper. Special thanks are due to Edwin B Fisher for his comments on a preliminary draft.