Rising to the challenge: will the NHS support people with long term conditions?
BMJ 2005; 330 doi: https://doi.org/10.1136/bmj.330.7492.657 (Published 17 March 2005) Cite this as: BMJ 2005;330:657
- Tim Wilson, general practitioner (tim.wilson{at}gp-k84036.nhs.uk)⇑1,
- David Buck, economic adviser2,
- Chris Ham, professor3
- 1Mill Stream Surgery, Wallingford OX10 6RL
- 2Department of Health, London SW1A 2NL
- 3Health Service Management Centre, University of Birmingham, Birmingham
- Correspondence to: T Wilson
The NHS is waking to the challenge of chronic diseases. Three researchers who have worked in the Department of Health discuss how the NHS might rise to the challenge of better supporting people with long term conditions
Introduction
The health gains experienced over the past 50 or so years are now presenting health systems around the world with a new challenge: how best to support people with long term conditions. An ageing population is testimony to improvements in public health through improved housing, sanitation and diet, and better health services—resulting in more patients surviving previously fatal events like serious infections but creating increasing numbers with long term conditions (fig 1). Over the past few years the British government has responded to issues that are foremost in the minds of the electorate, such as access to specialist services, especially in patient waiting times. This has evidently paid off.1 Now the NHS is waking to the challenge of chronic diseases. The NHS Improvement Plan, launched in June 2004, outlined the importance of supporting people with long term conditions. In the foreword, John Reid, the secretary of state for health, outlines how a “major investment in services closer to home will ensure much better support for patients who have long-term conditions, enabling them to minimise the impact of these on their lives.”2 We discuss how the NHS might rise to this challenge.

Percentage of respondents to general household survey 2002 (n=13 000) reporting a chronic condition. Data from 1998 onwards are weighted
{kind=link}
The scale of the problem
Analysis of the British household panel survey (2001), the health survey for England (2001), and general household survey (2002) has given us a great insight into how long term conditions affect people in England.3–5 The data show that:
Around 6 in 10 adults in the household population report some form of chronic health problem;
People with chronic health problems are significantly more likely to see their general practitioner (they account for about 80% of consultations), more likely to be admitted as an inpatient (on average about twice as likely given a particular problem, but up to seven times more likely for cancer), and use more inpatient days than those without (fig 2);
Health care utilisation intensifies with the number of problems reported (the 15% of people with three or more problems account for almost 30% of inpatient days);
Some people are highly intensive users of inpatient services: 10% of inpatients account for 55% of inpatient days, and within this are the very high intensive users, with 5% of inpatients accounting for 42% of inpatient days (fig 3);
People with any long term problem are about twice as likely to be intensive users than those without. Intensive users on average have three chronic problems, and are likely to be found among older people.
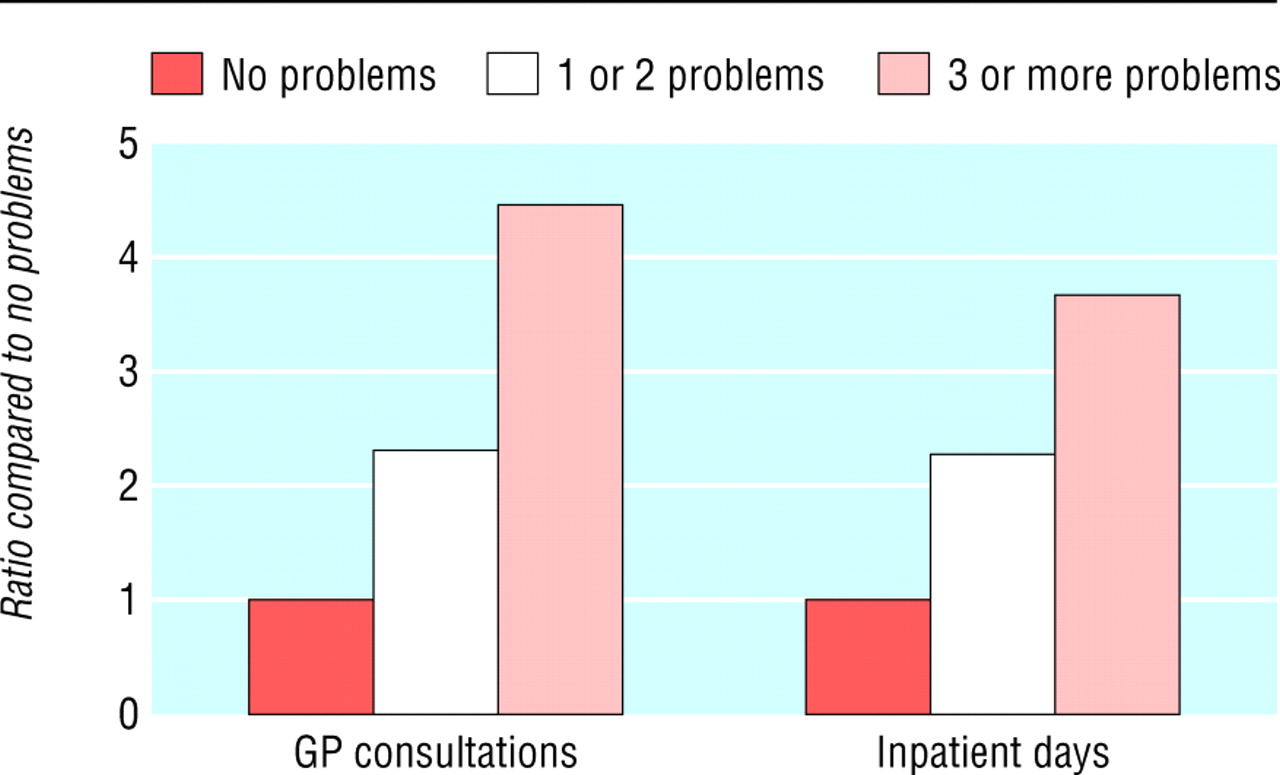
Likelihood of respondents to British household panel survey 2001 (n=5500) with chronic problems needing to use health services
{kind=link}

Cumulative days in hospital spent by patients admitted as inpatients. Source: analysis of British household panel survey 2001
{kind=link}
From this we can deduce three clear messages. Firstly, as does the rest of the world, the United Kingdom has many people with chronic disease—and we need an NHS that supports them. Secondly, people with chronic disease are disproportionate users of the health system. Thirdly, a group of patients, who tend to be older, have multiple long term problems and are spending disproportionate periods in hospital.
The commonest reported problems are those of the musculoskeletal and cardiovascular systems (table 1). Chronic diseases, although often associated with older adults, also affect children. In the United Kingdom, 15% of the under 5s and 20% of the 5-15 age group are reported to have a long term condition. The likelihood of a long term problem increases according to socioeconomic circumstances (fig 4).
Prevalence of chronic problems in the British household panel survey, 2001

Percentage of respondents to general household survey 2002 (n=13 000) with a longstanding problem
{kind=link}
NHS reform and the challenge of long term conditions
The NHS is undergoing a remarkable period of transformation.6 The reforms are backed by record levels of investment, with health spending in Britain expected to rise on average 7.4% a year in real terms for the next five years.7 This 43% real-terms increase will raise total UK health spending from 6.8% of gross domestic product in 1997 to an estimated 9.4% in 2007-8, near the upper end of current European levels. With the knowledge, therefore, that a reformed NHS needs to be able to better support people with long term conditions, how will the current reforms, backed by resources, match up to the chronic care model created by Wagner and colleagues?8
To promote better support of long term conditions. the Department of Health has entered into a public service agreement with the Treasury.9 This agreement to reduce emergency bed use by 5% in 2008 has led to an emphasis on case management of 250 000 very high intensive users. The anticipated fall in bed use will come from a mix of reduced length of stay and prevention of avoidable admissions; the former is likely to have a greater impact, given the incentives for acute trusts to discharge patients and the penalties faced by local authorities for delayed discharges.
Organisation of health care
Some features of the NHS sustain support for people with long term conditions. These include well established primary care teams (including community nurses and general practices) and a network of other community providers, including pharmacists and therapists. Crucially, having patients registered with a general practice offers great opportunities for supporting those with long term conditions and also provides patients with an unparalleled certainty about who will coordinate services and act as the final repository of care. For those with more than one condition, this is fundamental.10 However, the variations in care for people with chronic diseases by general practice are currently unsupportable,11 and changes in policy are seeking to reduce these variations.
The NHS is moving towards a system that is highly dependent on the effective commissioning of services by primary care trusts; in effect they are charged with ensuring that patients receive the support they need. As primary care trusts build their skills to more effectively commission care, they can ensure that financial incentives and mechanisms result in delivery of the best care for patients with long term conditions. To support trusts in their commissioning role are a series of financial incentives. Perhaps most significant is the new general practitioner contract, which includes the quality and outcomes framework, a reward system for the management of 10 important chronic diseases. Using an automated payment system based on the electronic patient record, this provides strong incentives for better clinical management of these conditions.
Another financial incentive is payment by results. This fee for service payment mechanism could affect patients with long term conditions in four ways:
Providers of specialist services are more likely to respond quickly to the needs of patients with long term conditions who need episodic care (such as an outpatient visit, cataract surgery, or joint replacement)
Money previously locked in hospital systems can be released for the benefit of community based services; research on the benefits of investing in ambulatory sensitive conditions (like heart failure or chronic obstructive pulmonary disease) indicates that this results in considerable benefit12
Acute trusts will make savings by reducing the length of stay, especially for those patients who occupy beds the longest, who are generally people with long term conditions
It might also have a perverse incentive: encouraging hospitals to increase (or maintain) activity inappropriately or face financial deficits.
The twin issues of reduced length of stay, and the incentive of hospitals to increase activity for patients with long term conditions, means that primary care trusts will have to work hard to balance investment between community based health and social care services, who pick up early discharges, and hospital departments, who see activities decreasing. The trusts can of course engage clinicians in the commissioning process to ensure that patients with long term conditions get the most appropriate care, most notably by giving practices an indicative budget. Another mechanism is to encourage networks of generalists and specialists to become involved in the commissioning process for particular disease areas.13 We are learning more about the importance of involving patients in the commissioning process; patients as co-designers of the healthcare system are potent allies for primary care trusts.
The trusts' ability to commission care effectively, including care for people with long term conditions, continues to be debated. Primary care trusts were established in 2002 and are still relatively immature organisations. Many have yet to make the most of their control of around 80% of the NHS budget. The balance of power within the NHS has resided with the providers of acute services, and the independence of these providers is being reinforced by the creation of NHS foundation trusts, a new kind of organisation managed at arm's length from the NHS. Primary care trusts in many parts of the NHS have found it difficult to negotiate on equal terms with acute services providers, in part because they lack the expertise and information to challenge the people running hospital services. Collaborative commissioning, in which neighbouring primary care trusts agree to work together to negotiate with providers, is being used in some places to address this issue. In parallel, the government is encouraging the trusts to devolve their budgets to general practices so that practices can commission some services directly. These developments have created uncertainty about the future of the commissioning function in the NHS.
Design of the delivery system
In the United Kingdom, medical specialists work in hospitals and generalists in communities, a demarcation that fragments primary and secondary care.14 The gap is even more pronounced between health care and social care, with little contact between community based teams. Efforts at bringing together primary health and social care organisations, such as the establishment of care trusts and joint commissioning of services, often miss the point as they represent managerial integration, whereas it is the staff who work with patients who need to cooperate. Fully integrated health and social care teams remain the exception rather than the rule.
The ability of primary care trusts to encourage and commission new ways of delivering care to people with long term conditions has been improved by the creation of a series of highly flexible primary care contracts. Initially designed to create more general practice services, they can also be used to provide specialist services, either as an add-on to general practice (enhanced services) or as stand alone specialist providers (specialist PMS (personal medical service) contracts). Effective exploitation of these contracts for the benefit of patients with long term conditions is not yet widespread, again raising questions about the capabilities of primary care trusts.
Central to effective working of the delivery system is what the national clinical director of diabetes, Sue Roberts, calls the three Rs; registration, recall, and review. Although the NHS has the virtue of a registration system, whether it is exploited to anticipate the needs of patients and stratifies them according to their risk is debatable. The delivery of planned and structured encounters through recall systems is improving, especially in practices that are actively improving care for the 10 long term conditions covered in the quality and outcomes framework of the new general practitioner contract. Preparation of patients for their review is far from optimal (in that they often do not know what is expected, what questions to ask, or how to get the most out of the encounter), and the extent to which prompts and reminders are used systematically across the whole NHS is unknown. As data become available from the quality and outcomes framework's electronic monitoring system this will become clearer. Finally, the review process must involve the systematic application of guidelines. Again, the new contract and the quality and outcomes framework, supported by computerised decision support and information systems, will address this issue for the diseases covered, but are unlikely to change care for those areas not addressed.
As we have outlined, case management for very high intensive users is receiving considerable emphasis. Various models of case management exist—for instance, SIPA in Canada, Evercare in the United States and United Kingdom, and Castlefields Practice in Runcorn. The results from these models suggest that the planned introduction of case management for 250 000 patients through the appointment of more than 3000 community matrons will certainly have an impact.1516 The exact size and nature of this effect is the subject of some debate, and the best methods to identify patients who will benefit is only beginning to be understood.1718 An iterative approach through formative evaluation seems critical.
Information systems
The development and use of guidelines will be facilitated in due course by the large investment in the National Programme for IT (information technology). A patient record, accessible across every part of the NHS, will go a long way towards overcoming some of the potential divisions in a pluralistic delivery system. Many other aspects of better support for long term conditions will also be facilitated by the programme: better planning for populations of patients, identifications of their needs, and support for commissioning, including easier monitoring of contracts. These will not be universal for some time, and the implementation will be difficult if the experiences of other healthcare IT programmes are repeated.19
Decision support
Variations in health care lead to overuse and underuse, not least for people with long term conditions. Some standardisation of care, especially corrections for underuse, will come from the quality and outcomes framework of the general practitioner contract. This is made possible by the extensive computerisation of primary care in the United Kingdom, a feature that is likely to increase given that payments are generated from data extracted directly from the clinical record. However, it means that a strong incentive system is influencing clinical decision making in general practice, something that has benefits and problems.20
Supported self care
The evidence base backing the use of generic programmes to support patients, like the expert patient programme and disease specific self management programmes for conditions like diabetes or chronic obstructive pulmonary disease, is strong.21 Although the expert patient programme is showing mixed results, it is clearly having a major impact on many patients.22 The challenge for the NHS is how to move from a programme that has trained 12 000 patients to one that can support the many millions of patients who might benefit. This poses three questions. Firstly, does the capacity exist to deliver the expert patient programme or disease specific self management programmes on this industrial scale? Secondly, with its limited resources, the expert patient programme has spare capacity (personal communication, Harry Cayton, National Director for Patients and the Public at the Department of Health, England); what will make the “prescription” of self care as routine as the prescription of a statin in heart disease? Further, will routine self care for all be as effective as it is now, in groups who have volunteered? Thirdly, little is known about the sustained effect of these programmes on life long conditions; what reinforcement is necessary?
Community resources and policies
One way of “industrialising self care” is through local communities and voluntary agencies. A notable example is the Healthy Communities Collaborative and the falls programme run by the National Primary Care Development Team (seewww.npdt.org/). Although formal evaluations are awaited, early results suggest that by harnessing the power of the communities themselves the collaborative process can be used to harness community resources. Communities and voluntary organisations often contain the necessary energy and enthusiasm required to make a difference. Evidence from other countries supports this, especially where primary care providers have linked to work with communities and non-governmental organisations.23 Primary care trusts need to work beyond the formal notions of joint planning and patient involvement to engage with a range of community groups. This can have dramatic effects on a whole community, improving a range of measures, including the care of long term conditions.24
Conclusion
Major reforms in the English NHS—including a massive investment in the NHS as a whole, the potential of effective commissioning, and opportunities opened up by the National Programme for IT—offer obvious benefits to patient with long term conditions. Challenges remain: ensuring commissioning is indeed effective, using incentives such as payment by results, avoiding the risks of NHS foundation trusts pursuing their own interests at the expense of the wider system, and achieving closer integration of service provision. These reforms could benefit patients who have long term conditions, but they carry tensions that could create problems if not properly applied or regulated (table 2).
Effects of system changes in the NHS on people with long term conditions
Case management is a target for the Department of Health. If the full potential of the current policy emphasis on chronic diseases is to be obtained, the NHS will need to link case management to more consistent disease management and self management in what amounts to nothing less than a paradigm shift in the way in which services are provided. At the heart of this shift is the need to move away from the acute care model, in which health services rescue patients when they become ill in an episodic manner, to a chronic care model, in which the resources of the healthcare system and communities are harnessed to provide high quality care over time.
Summary points
As the number of people with long term conditions in the United Kingdom rises, the NHS needs to adapt so it can respond to their needs
The NHS is experiencing investment and reform
Programmes already in place (especially case management by community matrons) are supporting people with long term conditions
Many reforms will create tensions in the NHS that, if managed well, will reap benefits for patients with long term conditions
The NHS must carefully monitor progress on supporting people with long term conditions so that it can learn, adapt, and make best use of the available opportunities
TW has been a senior policy analyst in the Department of Health strategy unit and CH has been its director. This article represents the opinions of the authors alone and does not constitute official Department of Health policy.
Footnotes
Contributors TW did much of the literature search and some analysis, brought together the evidence, and was the lead author of this article; DB did the most of the data analysis and epidemiological work; CH organised and planned the work on long term conditions in the Department of Health and helped write this article.
Competing interests DB is employed by the Department of Health. CH and TW are occasionally paid to speak and advise on policy matters, including the support of long term conditions