Too much technology
BMJ 2015; 350 doi: https://doi.org/10.1136/bmj.h705 (Published 16 February 2015) Cite this as: BMJ 2015;350:h705
- 1University College of Gjøvik, PO Box 1, N-2802 Gjøvik, Norway
- 2Centre for Medical Ethics, University of Oslo, Oslo, Norway
- 3Dartmouth Institute for Health Policy and Clinical Practice, Lebanon, NH, USA
- b.m.hofmann{at}medisin.uio.no
- Accepted 10 December 2014
Medical excess has been recognised as a key problem in modern healthcare.1 2 3 4 5 6 7 8 9 Overdiagnosis and overtreatment have been identified in a wide range of diseases,4 10 and medicalisation of ordinary human conditions has been heavily criticised.11 12 We seem to do too much of a good thing. Technology tends to have a crucial role in our propensity to excess.
From the invention of the stethoscope in Paris in 1816 to the whole genome sequencing of fetal cell-free DNA in a pregnant woman’s blood, technology has been a transforming factor in medicine. Technology has played a key part in moving medicine from the 2400 disease entities described in Sauvages’ 1793 Nosologica methodica to ICD-10 with more than 40 000 entries. Medical technology has also been a driving force in the growth of expenditure on health.13 14 15 It by far outweighs other price driving factors, such as an ageing population, increased public demand, income growth, raising prices, and reduced organisational efficiency. Half of the increase in the overall costs in healthcare are attributed to technology.16 Having a new technology raises the clout of hospitals and specialists and spurs a technological arms race.17 Technology is used beyond its benefit and sometimes even when it is harmful.18
No doubt, medical technology is a cornerstone in reducing ailment and improving health. Nevertheless, we need to address the challenges when the tool for improving health makes us diseased and when our means become our ends. Below I identify and analyse the mechanisms and the drivers behind using technology beyond its benefit and suggest measures to handle technology in a reflective and responsible manner.
Self perpetuating loop of diagnostics
The pervasive use of technology in healthcare is driven by a positive feedback loop in clinical diagnostics (fig 1⇓). The expansion of diagnostic technology often starts with a technical improvement—for example, increased spatial resolution of a diagnostic ultrasound machine. Such advances in technical performance may not result in better diagnostics—we may only see better what we already know.19 But sometimes they result in increased accuracy, in terms of improved sensitivity and specificity.19 A shift from ventilation perfusion scintigraphy to computed tomography pulmonary angiography increases the accuracy in diagnosing pulmonary emboli, revealing more cases of pulmonary embolism.20 This is perceived as a success, which results in closer scrutiny of the images and more frequent testing, leading to detection of milder cases21 and a higher diagnostic yield.22 Computed tomography pulmonary angiography increased the detection of pulmonary embolism by 80% from 1998 to 2006.5 Hence, the technological improvement uncovers a hitherto “under-detected” health problem.1 5 This increases the notion of success and the interest in diagnostic technologies.
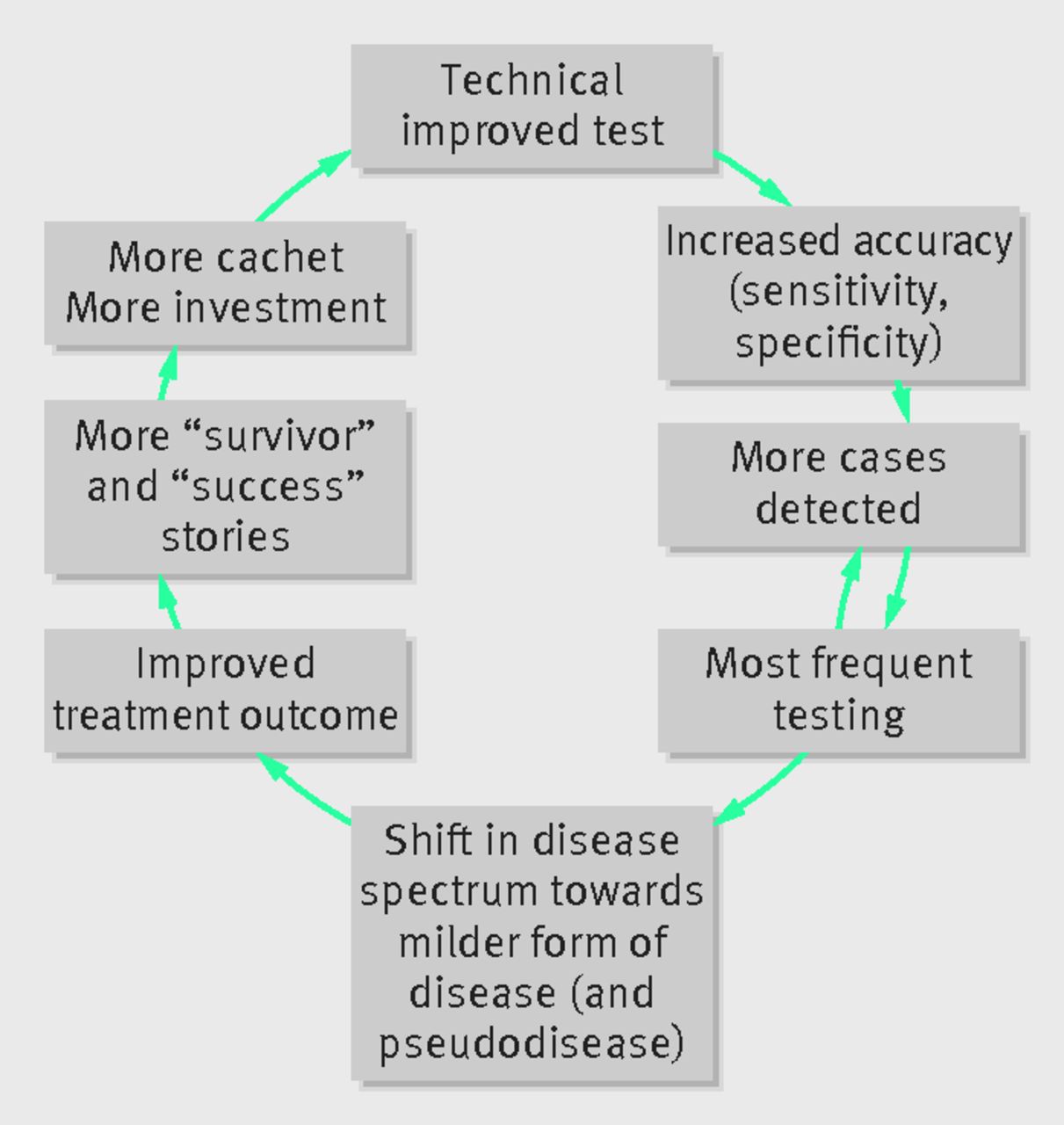
Fig 1 Self perpetuating loop of development in diagnostic technology
{kind=link}
Correspondingly, the increased number of diseased people spurs therapeutic attention. We start treating people who were previously not treated.18 Hence, ever milder cases are treated, as well as cases that would otherwise not have been detected. Computed tomography, magnetic resonance imaging (MRI), and ultrasound guided aspiration of thyroid nodules, for example, have increased the detection (and removal) of small papillary cancers.1 Treating milder cases improves outcomes, enhancing the impression of success, which in turn boosts technological innovation.18 Table 1⇓ gives some other examples where technology has changed the prevalence of disease.
1 Examples of conditions where technology has change detection of disease10
The profession and society seek technology
The pervasive use of technology in healthcare has many drivers (table 2⇓). At the systems level, the supply of technology drives demand.34 35 If an MRI scanner is available it is used. The same goes for blood tests and surgery.35 Technologies are widely used without evidence of their effectiveness, safety, and efficiency18 35 36 37 38 and sometimes even though there is evidence that they are not efficient—for example, pulse oximetry for perioperative monitoring and robot surgery.39 40 Occasionally technologies are used even when we know they are harmful.18 We are more eager to invest in new technology with little evidence than to disinvest in technology with evidence for little or no effectiveness.41 42
2 Examples of drivers of technology implementation in healthcare
Moreover, high tech is associated with high importance43 and high quality.44 Technology is used strategically to attract specialists and patients44 and impels a technological arms race.17 If your competitor has handheld ultrasound machines or a 3T MRI machine, you need to have them as well. Technology transforms from being instrumental to improving health to become a means of power and prestige, or even an end in itself.45 Professionals associate advanced technology with higher prestige both of diseases and specialties.46
Such perspectives are shared by patients, public, and the media, who request high tech interventions. Accordingly, general social myths drive the belief in technology. We believe that the new is better than the old, that the advanced is better than the simple, that more is better than little, that to know is better than not to know, and that to detect early is better than later. If doctors do not order a test, CT, or MRI people think they do not care. This is reinforced by the media. Angry or sad people who did not get the technology they should have hit the headlines, but those who have been overdiagnosed or overtreated are happy to have been “saved.”
Additionally, it has been argued that one of the major drivers is technology itself: there is a technological imperative,47 pushing technological innovation beyond healthcare needs, where technology defines diseases and provides the cures.11 48 This technology push has been explained by technology’s compensation for human deficiencies49 and as technology being autonomous.50 Technology has become an independent and powerful actor driving healthcare beyond its original goals. However, such (deterministic) views make us serfs of technology and reduce our responsibility. Paradoxically, we become servants of the technology we design, produce, implement, and use.51
The self perpetuating loop of diagnostic technologies and the identified drivers are helpful in understanding and addressing the pervasive role of technology in healthcare. However, they miss a basic bond between medicine and technology: how technology constitutes our conception of disease.
Technological construction of disease
Technology is changing the meaning of disease.52 53 More specifically, technology changes our conception of disease at three levels.54 Firstly, it provides the entities that define disease. Technology such as biochemical analysers, cytometers, and DNA sequencers provides access to enzymes, T cells, or specific strands of DNA. Hence, the core elements of diseases we find in definitions in medical textbooks are constituted by technology. Secondly, it is directing and structuring our knowledge of disease. One day our knowledge of myocardial infarction is based on the electrical activity in the heart measured by electrocardiography, the next it is more based on measurement of troponin in the blood. Thirdly, disease is constituted by technology through practice. If we can measure or manipulate something, it tends to become a disease—for example, hypertension and cholesterolaemia would not be relevant to medicine if we could not measure or manipulate blood pressure or cholesterol. Hence, the expansion of technology profoundly extends our conception of disease—for good and for bad.
Implications of pervasive technology
Fig 2⇓ shows some of the implications of the self perpetuating loop of diagnostic technology that are supported by the many drivers of technology and the technological constitution of disease. These include:

Fig 2 Some spin-off challenges from the self perpetuating loop of diagnostic technology
{kind=link}
Enhanced leaps of belief—The apparent success of diagnosing and treating more results in unwarranted enthusiasm among professionals and industry, hyped beliefs and demands among patients and the media, as well as unrealistic expectations among policy makers. Benefits seem self evident while downsides are veiled or ignored
Good tests become poor—A more accurate diagnostic test may result in poorer outcome if the test is used for ever healthier people. If a diagnostic test increases its sensitivity and specificity from 0.80 to 0.95, the chance that a given positive test result is correct decreases from 0.8 to 0.16 if the prevalence decreases from 1 in 2 to 1 in 100. Hence, technical improvements do not guarantee clinical improvements
Detecting more does not help people—Detection of cases does not mean that more patients are treated or that more lives are saved.1 55 56 Instead, more people become diseased, as disease categories are widened or everyday conditions become recategorised as disease. Technical improvements make us detect cases that would otherwise not have caused symptoms or death—that is, overdiagnosis— which subsequently leads to overtreatment.10 57 58 Hence, our technological endeavours to help become futile or even harmful
Increased activity—Intensified diagnostic activity generates incidental findings. While some “incidentalomas” save lives, many do not—for example, incidental detection of thyroid cancer with CT or MRI does not reduce symptoms or death.1 Follow-up of diagnostic findings produces other incidental findings. Hence, we do more but less with measurable outcomes for people’s health
Increased health anxiety—The raised disease prevalence and increased awareness of health problems make people more concerned and anxious about their health, spurring even more testing and treatment
Increased cost—The increase in screening programmes, diagnostic tests, incidental findings, and follow-up substantially raises health expenditure.13 14 15 This drains resources from areas where technology is really effective and innovations are really needed
Reduced value—When the predictive value of diagnostic tests is low, more people are overdiagnosed and overtreated, and people with social or other problems are given medical labels, the usefulness of healthcare endeavours is deflated
Undermining trust—With increased awareness of excessive healthcare,7 9 53 low value healthcare,59 60 and “not to do” health services,61 people may lose trust—the cornerstone of healthcare provision.
What we can do?
Uncritical implementation and use of technology excites excessive medicine. One reason for this is that technology is deeply ingrained in our conception of disease and our culture. It spurs a series of leaps of faith. Therefore, the first thing we have to do is to get rid of truisms, such as that more is better than less, new is better than old, and advanced is more accurate than simple. We must also acknowledge our responsibility for the development, implementation, and use of medical technology.51 When ordering tests and examinations we cannot evade our responsibility by referring to vague conceptions of technological imperatives, “progress,” or uninformed patients’ demands. We must ensure that we are not overly enthusiastic about new technology and adopt perspectives that grasp our ambivalence towards it, both controlling and feeling controlled. We can do so by understanding how technology expands human agency and perspective but at the same time frames and directs us.62 We also need to acknowledge how technology has become more than a neutral means for a human end,45 63 and how we address it as both an artefact and an actor.64
Although it is important to stimulate innovation we should restrain implementation. Only technology that has shown real benefit should be put into routine practice because access to technology is the most important determinant use in healthcare. 65 Technology assessment and transparent appraisal has to be strengthened to assure benefits for patients.42 Devices must be as critically assessed as drugs.66 67 Patients also need to be better informed about the uncertainties in benefits and risks of technologies, not only about the hyped gains. Their say should be acknowledged in the development, assessment, implementation, and use of technology.
In order to use technology to help and not harm, we need to reflect and to take responsibility. To cultivate and boost its true benefits, we must avoid the allures and acknowledge the limits of technology.We must strive to bring our abilities to contemplate on the use of technologies to match our abilities to produce and use them. This will ensure we avoid becoming tragic heroes, succumbing as a result of our best endeavours.
We believe that the new is better than the old, that the advanced is better than the simple, that more is better than little
Notes
Cite this as: BMJ 2015;350:h705
Footnotes
I thank H Gilbert Welch and two reviewers and the editor for their valuable comments and suggestions. Part of this research has been supported by the Commonwealth Fund through the Harkness Fellowship. The views presented here are not necessarily those of the Commonwealth Fund.
Competing interests: I have read and understood BMJ policy on declaration of interests and have no interests to declare.
Provenance and peer review: Not commissioned; externally peer reviewed.