Article Text

Statistics from Altmetric.com
The shift from surveillance to promotion requires paediatricians to play several roles in a larger multidisciplinary and multi-agency team
Child health surveillance programmes aim to prevent disease, detect physical and developmental abnormalities, and promote optimum health and development. There is growing evidence over the past decade that early intervention can change the life course for disadvantaged children. The emphasis has shifted from detecting developmental problems to preventing them and, in recognition of this change, the term “child health surveillance programme” has given way to “child health promotion programme”. Putting this programme into practice calls for awareness of the evidence as to what works. The evidence supports the need for a universal preschool service for all families and targeted intensive home visiting for high risk children. Preschool intervention and education benefit all children but particularly those at risk of educational failure. Children’s Centres may offer the opportunity to provide a more effective integrated service. The shift from surveillance to promotion requires paediatricians to play several roles in a larger multidisciplinary and multi-agency team, contributing to health promotion as well as facilitating early identification and providing expert diagnostic and management services.
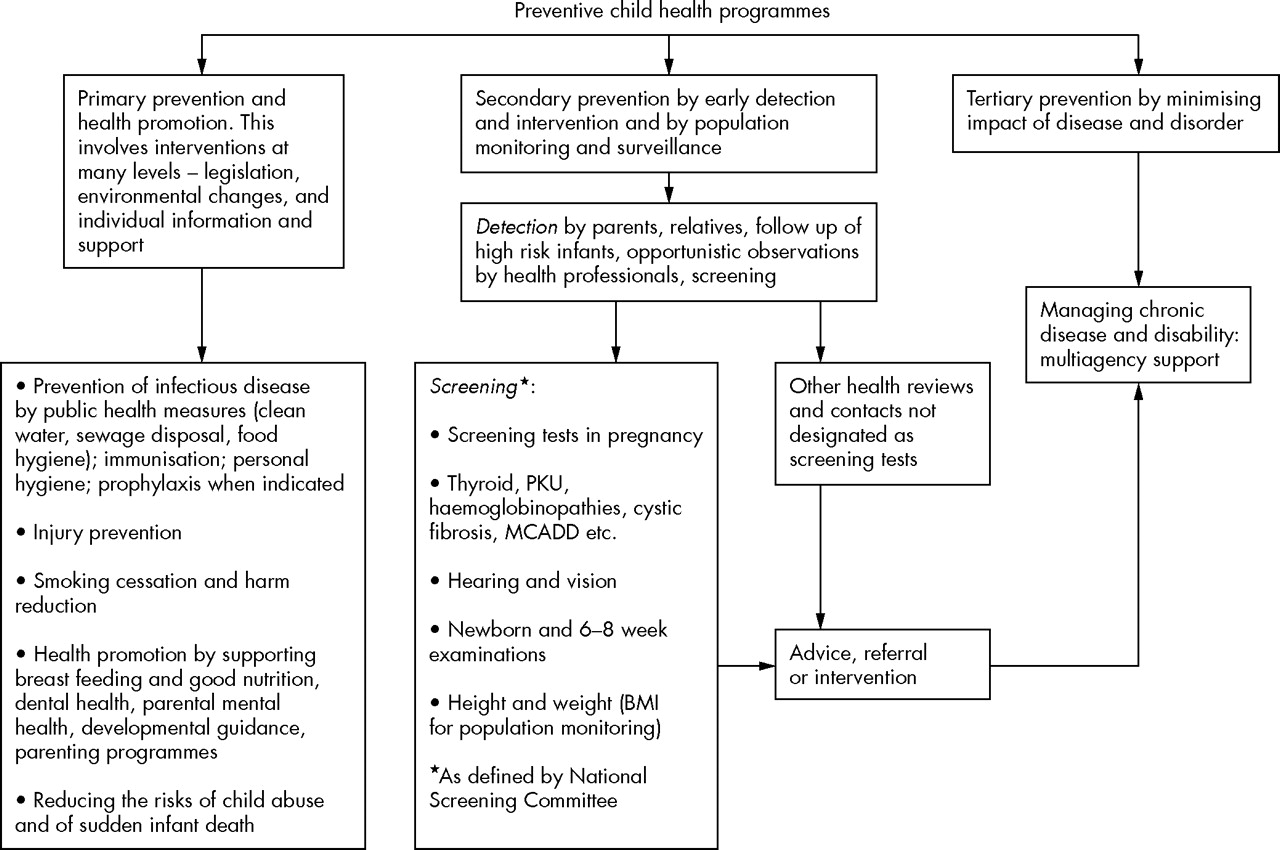
The current interest and investment in the promotion of optimum health and development for children is the result of emerging evidence that outcomes and life chances can be improved by preschool intervention programmes, coupled with growing concerns about health inequalities, educational under-achievement, juvenile crime, and social exclusion.1 Such concerns are not new; efforts to address their root causes date from the 19th century when there was a major public investment in sanitary reform and other environmental improvements. In the first half of the twentieth century, the major health concerns were nutritional deficiencies and infectious diseases. As these scourges came under control, more attention could be devoted to child rearing issues, behavioural problems, chronic disorders, and preventive medicine.2 Routine well-child examination schedules evolved that also included nutritional advice and immunisation; the whole package was designated the Child Health Surveillance (CHS) programme.3 Its focus was on the under-5s and the three main aims were disease prevention, health promotion, and early detection and intervention for physical and developmental abnormalities (fig 1).

Components of preventive child health programmes. *Details of the National Screening Committee can be found at http://www.nsc.nhs.uk/ch_screen/child_ind.htm.
Over the past 20 years the content of the CHS programme has been reviewed and updated four times by the UK Joint Working Parties on Child Health Surveillance.4 Their reports take an evidence based approach and argue that, while these three aims are as important as ever, the investment in routine examinations to detect occult disorders should be rationalised and reduced, whereas health promotion deserves a much greater commitment. This analysis is endorsed by the National Service Framework for Children, Young People and Maternity Services (NSF),5 published in 2004 by England’s Departments of Health and of Education and Skills, which proposes that the term CHS be replaced by “Child Health Promotion Programme”. The details of this new programme are set out in Standard One of the NSF.
The NSF programme emphasises the importance of implementing what is already known about prevention, early detection, and health promotion. Screening procedures are kept under regular review by the UK National Screening Committee, while many aspects of health promotion have been extensively studied and some have been the subject of systematic review. Examples of effective interventions include immunisation, promotion of breastfeeding, campaigns to reduce the risk of sudden infant death, injury prevention programmes, and support for depressed mothers. Although much remains to be learned about how to ensure that parents and children benefit from all these advances, there is little controversy about their relevance or the improvements that would result from their wider application.
In contrast, the identification of atypical or abnormal development or behaviour in children, and the opportunities to change educational outcomes and the life course, do attract controversy and have been the subject of intensive research. This paper aims firstly to summarise how emerging knowledge and changing concepts in these areas underpin the shift of emphasis from “Child Health Surveillance” to “Child Health Promotion”; it will then consider the obstacles that may be encountered and how the aims of the new programme might be achieved.
HEALTH SURVEILLANCE OR HEALTH PROMOTION?
Early identification of disability by CHS
Parents value early identification of any disabling condition in their child, as this facilitates emotional adjustment, educational planning, and other major life decisions. Developmental screening and examination procedures were introduced to facilitate early diagnosis in an era when there was little public and professional awareness of childhood disability, and children at risk of disability were not effectively identified or monitored.6 Disabling conditions such as cerebral palsy, severe visual impairment, classical autism, and many dysmorphic syndromes are now better understood and are more likely to be recognised at an early stage. The routine developmental examinations which for many years formed a major part of CHS programmes currently make little contribution to the identification of these children.7,8 This is not to deny a role for professional expertise and observation, but rather to suggest that early detection can be achieved in different ways—a point that we will return to later.
High prevalence problems in children
The disabling conditions mentioned above usually have an unequivocal biological basis and their recognition may be aided by physical signs or stigmata. They are individually and collectively uncommon. In contrast, difficulties in speech and language development, general and specific learning disabilities, and coordination problems are common, as are emotional and behavioural disorders. The overall prevalence of such problems is probably between 10% and 20% and calls for a public health perspective on root causes and prevention.
Changing concepts of child development
The child health surveillance model has not been effective in addressing these high prevalence problems. There are many reasons why this is so. In most cases they lie on a continuum of ability rather than reflecting a specific deficit or defect, so it is difficult to define what does or does not constitute a problem. The high prevalence of these difficulties, the uncertainty as to which children benefit from intervention, and the capacity needed to manage the workload all raise questions about the appropriate professional response to such children. Nevertheless, these difficulties are potentially soluble. There are some more fundamental reasons why a different approach is needed, arising from two main lines of research which can be categorised as developmental and interventional.
Developmental research
-
A child’s developmental progress, temperament, and behavioural patterns are not biological givens “hard wired” in the brain—they are the result of an interaction between the child’s genetic endowment and environmental influences within the family, neighbourhood, and school.9 For example, the concept of “specific language impairment”, as something a child either has or does not have, has given way to a more complex model in which genetic factors contribute significantly in the slowest developing 10% of the population, whereas in the rest a variety of potentially modifiable environmental factors play a more substantial role.10
-
Brain development and neural structures are permanently affected both by positive social experiences, and by abuse and neglect, in the first few years of life.11 Children can recover fully from short term exposure to grossly abnormal early environments but prolonged exposure thorough early childhood may result in permanent cognitive and emotional deficits.
-
Parental mental health problems impact significantly on child development. Depression in particular is associated with slower developmental progress, with boys affected more than girls. Although most research has focused on mothers, fathers’ depression is also a significant factor.12 These findings suggest the need to consider a child’s development in the context of the whole family, rather than in isolation.
-
There is a substantial social class gradient for most developmental and behavioural problems, with the lower social groups having a higher prevalence than the most prosperous.13 For example, the norm for speech and language development in the poorest areas of the UK is far below what is expected for middle class children. The amount of speech to which children are exposed varies widely.14 There are enormous differences in numbers and quality of social interactions and in proxies for early literacy, such as the number of books in a household.15
-
Life course research shows how early disadvantage is often compounded throughout life.16 Poverty is associated with sub-optimal pregnancy outcomes. Children with a temperamental tendency to aggression are more likely to become aggressive adults if they grow up in poor violent families and live in unattractive violent neighbourhoods.17 Parents who have little support or interaction with other people may be more at risk of neglecting their children, with adverse effects on learning, behaviour, and brain development. Life chances are already reduced at school entry, if children have fewer basic skills than their more fortunate peers. Early difficulties with language acquisition and behaviour are followed by failure to master reading and basic numeracy, conduct problems in school, educational failure, low earning capacity, and increased criminality. Morbidity and mortality are increased compared to more fortunate families. Brief interventions focused on single problems are unlikely to protect the child against these cumulative negative factors that persist all through childhood and into adult life.
Interventional research
-
Interventions to promote development and health in the early years can change life trajectories.18 For example, significant gains have been reported as a result of home visiting programmes for preschool children. Children who have participated in American Headstart programmes show improvements in many measures of adult function, for example higher income, reduced criminality, and more stable relationships. Economic analyses show these interventions to be a highly cost effective investment.
-
Preschool education has a significant impact on progress and performance in school; the magnitude of benefit is related to several factors including starting at an early age, a structured educational approach, qualified and well trained staff, and the quality of the home environment.19
-
Parents can be taught strategies that accelerate language development; for example, expansion and recasting of children’s utterances into a different or more complete linguistic form, commenting on the child’s focus of interest, and following the child’s lead rather than trying to direct their play. Parenting styles significantly affect both the immediate and the longer term behavioural patterns and emotional health of their children; parents who have difficulty in managing their young children’s behaviour benefit from parent education programmes.20
-
Approaches to bring about change in whole communities as opposed to individuals—“community development” programmes—are also reported to have beneficial results for children and families.21
The case for promoting early child health and development
The current enthusiasm for promoting children’s health and development arises from the convergence of these developmental and interventional strands of evidence, from a range of disciplines with radically differing perspectives and research methodologies. Early intervention can change life trajectories; an integrated multidisciplinary approach involving health, education, and social services expertise is needed to apply this knowledge and to address the obstacles to optimum child development—the social and mental health issues affecting parents and carers, the difficulties that many adults have in understanding the needs of young children, and the poverty of learning opportunities experienced by many children.
RESEARCH INTO PRACTICE
Programmes like England’s Sure Start were intended to implement these research findings. The NSF supports these aims in the new Child Health Promotion Programme. Three main difficulties have been encountered in implementing such programmes.
Engaging families: inverse care
The most disadvantaged children would have the most to gain from targeted interventions but early intervention programmes illustrate the inverse care law—most children do benefit, but those families who might benefit the most are the ones least likely to access such help. Traditional CHS programmes experience a steady decline in the uptake of routine health and development checks as children get older; this decline is steeper in the poorest social groups (fig 2). It was hoped that the local community focus and increased investment associated with programmes like the American Head Start or England’s Sure Start would be more successful in reaching all the eligible families, but many families remain hard to reach and engage in any intervention or service.22,23 Interviews with parents who do not take up services offered to them provide some insight into the reasons24,25 (see box 1).

{kind=link}
{kind=link}
Proportion of children seen at each preschool review in relation to the child population by deprivation quintiles. Data derived from the 10 Health Boards in Scotland who report to the CHSP-PS and the ISD Scotland. In spite of a policy of regular universal reviews, the coverage declines at each successive health check, but declines more steeply for the more deprived social classes.
Box 1: Why is it difficult to engage some families in preschool programmes?
Professional issues
-
Shortages of well trained staff
-
Professional ambivalence about use of time and worries about “no access” visits
-
Professional fear of being too intrusive or of uncovering problems that have no solution
-
Inaccurate record systems (data entry errors, parents changing their or their baby’s name), high mobility of young families (multiple changes of address)
Practical obstacles: parental issues
-
Changes of address concealed to escape debts or a violent partner
-
Parents returning to work, leaving their baby with a minder
-
Lifestyles that don’t fit within the hours of the professional working week
-
Parents working long or unsocial hours (too exhausted to contemplate any additional activities with their children)
-
Transport to children’s facilities is expensive for those on low incomes
Attitudinal issues
-
Low level of trust in, or respect for, the heath professionals they know
-
Previous conflicts with health professionals; arguments about smoking or weaning
-
Perception of professionals as superior, authoritarian, and out of touch
-
Feelings of inadequacy about entering the territory of middle class health professionals
-
Phobia of social encounters at children’s clinics or health centres
-
Ethnic, cultural, and linguistic barriers
-
Fear of exposing poverty, poor quality child care, abuse, or domestic violence to “prying eyes” of professionals
-
Embarrassment over poor reading ability
-
Parental mental illness, domestic violence, or substance abuse
-
Not seeing any need for professional advice about their children
Not only do the most needy families fail to engage in and benefit from early intervention opportunities, but a small proportion may actually show a decline in their children’s performance relative even to their own deprived district.26 The reasons for the decline are not fully understood, but the risk factors that characterise these very vulnerable parents include teenage parenthood, poor education, poverty, substance abuse, mental illness, and domestic abuse and violence. These parents have no reserve of personal resources or support to improve their and their children’s lives. The result is that inequalities can widen—the opposite of what was intended.27
Difficulty in tracking children
The most needy children are often also the most mobile. As yet few areas have multi-agency databases that could simplify tracking of all children, minimise attrition and dropout from early intervention programmes, and facilitate measurement of coverage and outcomes, nor do they have staff with the public health expertise and leadership qualities to utilise such data effectively.
Programme quality and degradation
The third difficulty in implementation is in maintaining the standards of the demonstration projects that showed intervention could be effective, when these are taken to a national scale. Adherence to an agreed programme of proven effectiveness is crucial in generalising interventions and calls for sound training, strong leadership, and continued monitoring. Staff with a lower level of training and professional expertise, working in a programme whose quality and content have been reduced, will not deliver the same results as in the original project.28 This applies both to centre based approaches and to home visiting programmes.
THE NEW CHILD HEALTH PROMOTION PROGRAMME
The NSF programme of child health promotion calls for collaboration involving health, education, and social services. The recurring dilemma is the need to provide on the one hand access to universal services for every parent and child, but on the other to increase investment and provision for families whose children are at risk of future educational and behavioural problems because of their circumstances—and to do this without stigmatising parents or appearing to criticise their child rearing skills.
A universal service in the first year of life
There are four reasons why the existing universal service should continue:
-
There are some screening and health promotion procedures of established value that should be undertaken with every child.
-
Many problems of early childhood, notably developmental disorders, and vision and hearing defects, are often first suspected by parents, so all parents need to know about the services and support that are available if they have any concerns, and how they can access these.
-
Without a universal service it is impossible to locate and engage with all those parents who may have difficulty in accessing routine health care. Developing a family service plan for such parents needs face to face contact. Checklists and “problem scores” have sometimes been introduced by managers to identify high risk families,29 but their apparent efficiency is illusory as such methods take no account of parental wishes, attitudes, or supportive networks of relatives and friends.
-
A service that is provided for everyone is likely to be more acceptable than one perceived as being targeted just at “bad parents”.
A universal service does not imply that every family has the same needs; rather, that it aims to determine what services and support each individual family requires and will use. The NSF proposes:
-
A “family services plan” to be agreed jointly by the family and health professional, and completed by the child’s first birthday
-
A more targeted approach thereafter with fewer “routine” health professional contacts, releasing staff to offer intensive educational and social support for those who need it
-
Clear goals and objectives based on an agreement both with individual families and the community as a whole
-
All staff who work with preschool children to have a common core training.30
A targeted service
For the most needy families, initial engagement and early intervention might be achievable by means of more intensive targeted home visiting.31 The key to success seems to lie in creating a high quality supportive and therapeutic relationship which will give parents the confidence to access other services.32 “Quality” implies continuity of care from pregnancy and through at least the first year or two of the child’s life; a willingness to listen to the parental agenda and not impose a professional one; the ability to switch between practical problems and sensitive personal issues in response to parents’ cues; and an extensive repertoire of professional skills and knowledge relevant to child development, child rearing, and parents’ mental health.
An integrated multi-agency approach
“Children’s Centres” build on the Sure Start experience and aim eventually to serve all families with preschool children. This approach may help to solve the dilemma of how to engage hard to reach parents without the stigma associated with targeted schemes. They will offer preschool education for all and access to Early Support for children with special needs; in addition, they will give parents a chance to develop their social networks, observe their own and other children, discuss any worries, and receive advice on nutrition, language, pre-literacy skills, and behaviour management, from other parents and from professionals.
Universal access to children’s centres and preschool services will provide opportunities for staff to observe children over a period of days or weeks, rather than just in a single short encounter as in traditional surveillance procedures. Early years staff trained in the normal range of child development and behaviour will advise parents and discuss any worries, opening their eyes to developmental needs and possible problems such as autism spectrum disorders. A similar approach called “Platforms”, based on a structured interview,33 is currently being developed in Australia.
THE POLITICAL RESEARCH QUESTION: WILL CURRENT POLICIES REDUCE THE INEQUALITIES IN OUR SOCIETY?
Between-country comparisons show that in developed countries there is a strong relationship between income distribution and a wide variety of outcome measures including reading and mathematical performance of children, crime, and perceived social cohesion. A more equal distribution of wealth is associated with better outcomes. The big question is whether improved preschool services and educational support, combined with current efforts to eliminate child poverty, will be sufficient to reduce socioeconomic and health inequalities in the UK.
Acknowledgments
We thank Simon Fraser and Jim Chalmers (Scottish Office of Statistics) for the data in fig 2.
The shift from surveillance to promotion requires paediatricians to play several roles in a larger multidisciplinary and multi-agency team
REFERENCES
Footnotes
-
Competing interests: none