Article Text

Abstract
Background Epidemiology of spontaneous pneumothorax has been scantily studied. We aimed to assess the incidence of spontaneous pneumothorax and describe patients’ characteristics with respect to age, sex, seasonal occurrence, primary or secondary character, surgical management and rehospitalisations on a large-scale database.
Methods Data from all patients aged ≥14 years and hospitalised with a diagnosis of non-traumatic pneumothorax in France from 2008 to 2011 were retrieved from the National Hospitalisation Database.
Results There were 59 637 hospital stays corresponding to 42 595 patients. Twenty-eight per cent of patients were rehospitalised at least once during the 4-year period. Annual rate of pneumothorax could be estimated at 22.7 (95% CI 22.4 to 23.0) cases for 100 000 habitants. The women to men ratio was 1:3.3. Mean age was significantly higher in women than in men (41±19 vs 37±19 years, p<0.0001). No seasonal variation was observed. A surgical procedure was performed in 14 352 hospital stays (24%). In the group of patients aged <30 years, there was no statistical difference between men and women with regard to type of pneumothorax (primary or secondary), type of hospitalisation unit (surgery vs medicine), treatment modality (surgery or not), intensive care unit (ICU) admission and hospital stay duration. Rehospitalisation was more frequent in women than in men (56% vs 52%, p<0.0001). In the 30–49 years age group, surgery and rehospitalisation were more frequent in women than in men (each, p<0.001). In the 50–64 years age group, surgical procedures and rehospitalisations were more frequent in men than in women (p=0.002 and p<0.0001, respectively).
Conclusions Sex and age are determinant factors in the course of spontaneous pneumothorax.
- Clinical Epidemiology
- Pleural Disease
Statistics from Altmetric.com
Key messages
What is the key question?
Are characteristics of idiopathic pneumothorax different with respect to sex and age?
What is the bottom line?
Sex and age are strong determinants of the occurrence and course of spontaneous pneumothorax.
Why read on?
The largest epidemiological study on spontaneous pneumothorax.
Introduction
Pneumothorax is a frequent disease involving general practitioners, emergency room and intensive care unit (ICU) physicians, chest physicians, as well as general and thoracic surgeons. It is classified as traumatic or spontaneous. Spontaneous pneumothorax is termed primary in the absence of any obvious precipitating factor or secondary if an underlying pulmonary disease is present.1
Very few studies assessed the incidence of spontaneous pneumothorax on a large-scale basis. The first was performed 40 years ago in the USA as part of the Rochester Project.2 Subsequently, data from three national UK registries (General Practice Research Database, Hospital Episode Statistics and Data Science UK) were published in year 2000.3 Interestingly, in this study, all cases of pneumothorax with or without hospital admission were evaluated. The incidence rate of primary and secondary pneumothorax was estimated at 24.0/100 000 years in men and 9.8/100 000 years in women. We found no other large-scale study on the epidemiology of spontaneous pneumothorax, and further knowledge is derived from case series, with often conflicting results.4–9 A female to male ratio ranging from 1:2 to 1:6 has been suggested, but the incidence and distribution of pneumothorax with respect to age and sex are poorly known.2–6 A first peak of incidence occurs at 20–25 years in men (relating to idiopathic pneumothorax) and a second peak is observed in both men and women aged more than 55 years, relating to underlying chronic lung diseases (mostly COPD).3 In women, the epidemiological study by Gupta et al3 found that the first peak is delayed at 30–34 years. The reasons for this gender-related difference are not known, but factors associated with idiopathic pneumothorax in men (active tobacco consumption and anthropometric characteristics) are less frequently found in women.10 ,11 While some case series did not confirm these findings,4 ,9 recent prospective and retrospective surgical series also found a later occurrence of pneumothorax in women and showed that catamenial pneumothorax and endometriosis-related pneumothorax were responsible for approximately half of pneumothorax episodes in women of childbearing age referred for surgery.12–14 To date, no data on non-surgical cases of catamenial or endometriosis-related pneumothorax is available.
Some case series showed that changes in atmospheric pressure and some meteorological events (thunderstorm) were associated with clusters of pneumothorax, regardless of sex, raising the question of a possible seasonal character of the disease.15–17 However, the UK epidemiological study did not find such a seasonal distribution.3
In the present study, we aimed at investigating on a nationwide basis the characteristics, management and course of patients hospitalised with spontaneous pneumothorax. Specifically, analyses were designed to determine the incidence of this condition, age and gender distribution, type of pneumothorax (primary or secondary), proportion of patients undergoing surgery, length of hospital stay and number of hospitalisations, as well as the influence of age, gender and type of pneumothorax on these outcomes.
Methods
Study design and database structure
The study is based on 2008–2011 exhaustive data from the ‘Programme de Médicalisation des Systèmes d’Information’ database (programme for medicalisation of information systems, PMSI) of the national healthcare system, which collects data on all hospital stays, regardless of duration, in French public and private hospitals. In addition to its administrative purpose (monitoring of hospital activity based on the diagnostic-related groups (DRGs) model to inform pricing and strategic decisions by payers and policy makers), the database is also used for epidemiological purposes in several areas.18–22 Data are collected on a real-time basis and analysed yearly and include the ciphered identification of the patient, the main diagnosis leading to the hospitalisation, associated comorbidities and hospital-related complications, as well as other administrative and medical information, including some treatment modalities. Diagnostic coding relies on the international classification of diseases (ICD, WHO) and follows its updates. Coding of medical and surgical procedures is based on the French ‘Classification Commune des Actes Médicaux’ (common classification of medical procedures, CCAM). The main diagnosis is allocated by treating clinicians in charge of the patients immediately after discharge.
Retrieved data
All stays with a discharge diagnosis of non-traumatic pneumothorax were retrieved. The data obtained from each stay included the age and sex of the patient, the primary or secondary nature of the pneumothorax, the type of hospital unit(s) in which the patient was hospitalised (medicine/surgery/ICU), the month of hospitalisation and the duration of hospital stay. All iterative hospitalisations of the same patients during the 4-year study period could be identified.
Statistics
Categorical data were described as numbers (%) and continuous variables as mean (SD). Characteristics were compared (1) between men and women and (2) between idiopathic and secondary pneumothorax, using generalised estimating equation (GEE) to account for multiple hospitalisations of a given patient. For the comparison between male and female, we stratified analyses by age classes (≤30, 31–50 and 51–65 years old). Finally, we assessed which characteristics were associated with length of stay and surgical treatment. For all tests, a p value (two-sided) <0.05 was considered statistically significant. In this exploratory study, we did not correct α risk for multiple testing.
Results
In the national database, among more than 68 million hospitalisations, 60 094 were associated with a main diagnosis of non-traumatic pneumothorax over the period January 2008–December 2011. After excluding 436 hospitalisations related to patients aged less than 14 years and 21 with inadequate coding data, 59 637 hospitalisations were analysed.
Characteristics of patients
The 59 637 hospitalisations corresponded to 42 595 patients. Mean age was 39±20 years. A total of 32 632 (77%) were male, corresponding to a women to men ratio of 1:3.3. Pneumothorax was idiopathic in 85% of patients (n=36 563) and secondary in 15%. A total of 12 084 patients (28%) had more than one pneumothorax-related hospital stay over the 4-year period. There were 44 815 hospital stays during the first 3 years, corresponding to 32 618 patients. Out of these, 8653 (26.5%) had a recurrence within 1 year of the first recorded episode.
Distribution of hospitalisations over the 4-year period
The annual number of hospitalisations for pneumothorax was stable over the study period, with between 14 747 and 15 170 hospital stays yearly. Thus, the annual rate of hospital stay for spontaneous pneumothorax in France (considering a French population of 65.7 million) could be estimated at 22.7 per 100 000 (95% CI 22.4 to 23.0 per 100 000). There was no significant monthly or seasonal variation of distribution: March, October and December accounted each for 9% of hospitalisations, the other months for 8%, while 25% of the cases occurred in winter and spring, 24% in summer and 26% in the autumn (table 1). No significant difference in the seasonal distribution of hospitalisations was observed between men and women or between primary and secondary pneumothorax (data not shown).
Characteristics of hospitalisations for non-traumatic pneumothorax between 2008 and 2011 in France
Characteristics of hospital management
Overall, the median duration of hospital stay was 7 days. Hospitalisations occurred in a medical unit in 73% of cases and in a surgical unit in 27% of cases. In 27% of cases, the management involved intensive or intermediate care. A surgical procedure was performed during 14 352 hospitalisations (24%), mostly through thoracoscopy (76%). The most commonly performed procedures were thoracoscopic resection of blebs with a pleural abrasion in 7529 (52%) cases and a talc pleurodesis in 24% of cases (table 1). Surgery was associated with younger age (mean, 34 vs 39 years, p<0.0001), secondary pneumothorax (p<0.0001) and ICU surveillance (p<0.0001). There was no difference in the type of surgical intervention (especially, thoracotomy vs thoracoscopy) with respect to the type of pneumothorax (data not shown).
Differences between men and women
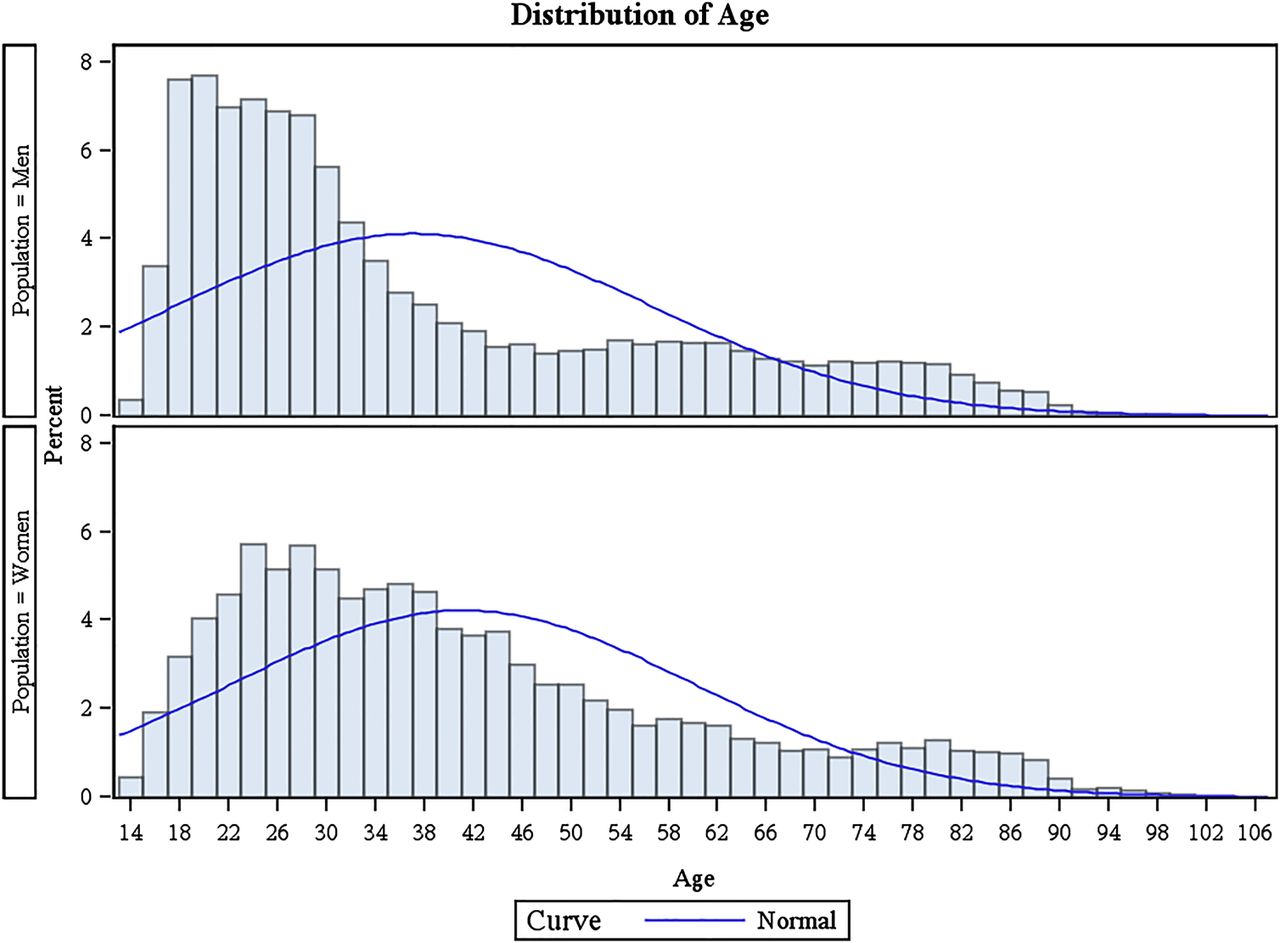
Mean age was significantly higher in women than in men (41±19 vs 37±19 years, p<0.0001). Age distribution showed a different profile between sexes (figure 1), with a more marked peak in young men and a shift towards higher age in women. Secondary pneumothorax was more frequent in men than in women (16% vs 13%, p<0.0001). A surgical procedure was slightly more common in men than in women (24% vs 23%, p=0.02) (table 2). Subgroup analysis showed that age was higher in women with pneumothorax considered idiopathic as compared with men (p<0.0001), but lower in women with secondary pneumothorax (p<0.0001) (table 2).
Comparison of hospitalisation characteristics between men and women

{kind=link}
Distribution of hospitalisations for spontaneous pneumothorax with respect to sex and age class. Each bar represents a 2-year age class.
In patients aged less than 30 years (N=25 156), there was no statistical difference between men and women with regard to type of pneumothorax, type of hospitalisation unit (surgery vs medicine), treatment modality (surgery or not), ICU admission and duration of hospital stay (table 3). Rehospitalisation was more frequent in women than in men (56% vs 52%, p=0.001). Among patients aged 31–50 years (N=15 906), there was a significantly higher rate of hospitalisation in a surgical unit in women than in men (32% vs 29%, p<0.0001) as well as a higher rate of surgical intervention (28% vs 26%, p=0.004). The risk of being hospitalised for pneumothorax more than once during the study period was also significantly greater in women (54% vs 46%, p<0.0001). In patients aged 50–65 years (N=7774), secondary pneumothorax was significantly more frequent in men who were more frequently hospitalised in a surgical unit (p<0.0001) and underwent surgery more often (20% vs 17%, p<0.0001). Hospital stay was longer in men than in women (mean duration 10.1 (14.5) vs 9.5 (14.8) days) (p<0.0001), and rehospitalisations were also significantly more frequent in men (45% vs 38%, p<0.0001).
Comparison of hospitalisation characteristics between men and women stratified by age
Differences between idiopathic and secondary pneumothorax
Mean age was higher in patients with secondary pneumothorax than in those with idiopathic pneumothorax (53±20 vs 35±18, p<0.0001) (table 4). The proportion of men was significantly higher for secondary than idiopathic pneumothorax (80% vs 76%, p<0.0001). In patients with secondary pneumothorax, a surgical procedure was more frequent (33% vs 23%, p<0.001) and, accordingly, more patients were hospitalised in a surgical unit and/or in an intensive or intermediate care unit (36% vs 26%, p<0.0001 and 40% vs 25%, p<0.0001, respectively). Hospital stay was significantly longer (median duration 8 (5–14) vs 5 (3–7) days). In these patients, the risk of multiple hospitalisations for pneumothorax was higher (52% vs 48%, p<0.0001).
Comparison of hospitalisation characteristics between idiopathic and secondary pneumothorax
Characteristics associated with duration of hospital stay
Age (p<0.0001), secondary pneumothorax (p<0.0001), hospitalisation in a surgical unit (p<0.0001), intensive care or continuous surveillance (p<0.0001) and surgical treatment (p<0.0001) were associated with duration of hospital stay (data not shown).
Characteristics associated with multiple hospitalisations
When comparing the characteristics of the patients recorded at first hospital stay during the 4-year period, those who had more than one hospitalisation were younger (35±18 vs 40±20 years, p<0.0001), underwent a surgical procedure more frequently (18% vs 17%, p<0.0001) and were more frequently hospitalised in a surgical unit (21% vs 19%, p<0.001).
Discussion
This analysis of all hospitalisations for adult spontaneous pneumothorax recorded in an exhaustive nationwide database during a 4-year period provides unique data on the epidemiology and management of spontaneous pneumothorax at a population level. Major findings relate to the rather high annual incidence of hospitalisations (22.7/100 000), the lack of seasonality, the strong male predominance (sex ratio: 1:3.3), the younger age and earlier peak of incidence in men, the rate of surgical procedures (about a quarter of the patients) and the high proportion of patients with multiple hospitalisations for pneumothorax (28%). An age-dependent influence of gender on disease's characteristics and outcomes was also demonstrated, suggesting that pneumothorax in men and women are largely different diseases. As expected, secondary pneumothorax also has specific characteristics from epidemiological (older age, greater male predominance), management (more frequent surgery) and outcomes (higher length of stay and number of hospitalisations) perspectives. This could, in part, explain some gender-related differences since secondary pneumothorax is more frequent in men. However, other factors might contribute.
Strengths and limitations of the study
The most obvious strength of this study relates to the high number of cases that could be analysed, permitted by the exhaustive nationwide character of the database with regard to hospitalisations. This allows determining whether findings from case series apply at a population level.
The lack of data on pneumothorax managed in the community could be considered as a study limitation. However, it should be pointed out that national recommendations for the management of spontaneous pneumothorax suggest hospital admission regardless of the character and extent of pneumothorax. A small percentage of asymptomatic patients with a first episode of idiopathic pneumothorax and a minimal apical (<3 cm) pneumothorax are managed on an out-patient basis, provided that (1) the pneumothorax does not aggravate after some hours of observation in the emergency department, (2) the patient lives close to hospital facilities and (3) the patient is not alone at home.23 These patients are not taken into account in this study, which may reduce the estimates of incidence and recurrence. However, they represent only a small fraction of the whole population of spontaneous pneumothorax patients. Other limitations relate to the nature and corresponding structure of the database. The lack of complete clinical data prevents from assessing in more detail the clinical factors associated with demographical features, management and outcomes. Similarly, assessment of recurrences was limited by the lack of data on both history of pneumothorax before and after the 4-year study period and the side of the pneumothorax. Finally, it should be acknowledged that the quality of coding might vary from one hospital to another.
Incidence rates
The annual rate of hospitalisation for non-traumatic pneumothorax is unknown so far in the majority of countries. In our study, the corresponding figure was 22.7 per 100 000. Taking into account rehospitalisations, this rate decreased to 16.2 per 100 000 habitants. These rates are similar to those reported in the study of the Rochester programme in Olmsted County, Minnesota, which showed an age-corrected incidence of 13.7/100 000 for men and 3.2/100 000 for women.4 Interestingly, in the UK study of about 22 000 cases, the overall consulting rates for primary and secondary pneumothorax were 24.0/100 000 years in men and 9.8/100 000 years in women, whereas the hospital admission rates were 16.7/100 000 years and 5.8/100 000 years, respectively.3
We observed a lower incidence of secondary pneumothorax than in previous epidemiological studies.4 However, it should be pointed out that most of these studies involved much lower numbers of cases from limited numbers of centres (in the Rochester study, there were141 cases of spontaneous pneumothorax, of which 77 were considered idiopathic and 64 secondary). Thus, some selection, assessment or reporting biases cannot be excluded. In our study, we cannot exclude that, in some instances, underlying lung disease was not reported in medical records, but this is unlikely and therefore should not affect results. In addition, the amount paid to hospitals by the French National Health System is greater when associated diagnoses are present, which favours adequate reporting of comorbidities.
Seasonality
The seasonal character of pneumothorax remains a matter of debate. It has been previously reported that pneumothorax occurs in clusters and such clusters are thought to be related to changes in atmospheric pressure.15 Likewise, it has been suggested that some particular meteorological events (thunderstorms) are also associated with the occurrence of pneumothorax.16 On the other hand, a possible seasonal character could be explained by the recrudescence of respiratory infections in winter rather than changes in atmospheric pressure.16 In the present study, we did not find any seasonal variations in the occurrence of pneumothorax.
Gender-related specificities
We confirmed the marked predominance of spontaneous pneumothorax in men with a women to men ratio of 1:3.30. Age at hospitalisation was significantly higher in women, an already reported characteristics of spontaneous pneumothorax.3 Additionally, we were able to provide further insight in differences between men and women regarding age distribution (figure 1): in men, the first peak of incidence occurred before the age of 20 and the incidence progressively decreased until about 50 years of age, where it rapidly rose again. This typically reflects the peak of incidence of idiopathic pneumothorax observed in young men and the peak of secondary pneumothorax, mainly related to underlying chronic lung diseases (mostly COPD). Among women, the first peak appears to be delayed and incidence remains stable up to 40 years. Similar to men, a second peak is observed around 60 years (although to a lesser extent than in men), probably also due to COPD-related secondary pneumothorax. Thus, if the second peak of pneumothorax (beyond 55 years) probably shares the same characteristics in both genders, features of pneumothorax at younger age seem markedly different between men and women. Differences are particularly prominent in the 30–50 age group. In this category, women had a higher rate of surgery and rehospitalisation. Although data recorded in the database do not allow any firm conclusion, it can be hypothesised that a significant part of cases occurring in women of this age range relates to thoracic endometriosis syndrome (catamenial pneumothorax, endometriosis-related or not and non-catamenial endometriosis-related pneumothorax).9 ,14 Indeed, pathological studies have underlined that these gender-specific pneumothorax account for up to 40% of pneumothorax in women referred for surgery.14 ,24
Management
Video-assisted thoracoscopic apical resection with pleural abrasion is the more frequent procedure. Other techniques, including talc pleurodesis with thoracoscopic or thoracotomic apical resection, are less frequently implemented.
In conclusion, despite some limitations, this study brings important information on the epidemiology of spontaneous pneumothorax, including incidence, sex ratio, age distribution, as well as surgical procedures performed. Furthermore, this study outlines the differences in clinical presentation and course of spontaneous pneumothorax between men and women at different ages, which could reflect gender-related differences in the occurrence of secondary pneumothorax and gender-specific pathogenic mechanisms of spontaneous pneumothorax in younger patients. The present study highlights that these differences are relevant at a population level and might have implications for management strategies, both from diagnostic (endometriosis diagnostic workup) and therapeutic (decisions of surgery) perspectives. To better answer these questions, it would be useful to set nationwide exhaustive database registries centred on the clinical and pathological aspects of spontaneous pneumothorax.
References
Footnotes
Contributors AB, SB and AD conducted and are responsible for data analysis and drafting of the manuscript. DD, AR and J-FR contributed to the study design. NR contributed to data analysis and performed revision of the manuscript. MA was responsible for study conception and design and contributed to manuscript writing and revision.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.