Article Text

Abstract
Background In haemodynamically stable patients with acute symptomatic pulmonary embolism (PE), studies have not evaluated the usefulness of combining the measurement of cardiac troponin, transthoracic echocardiogram (TTE), and lower extremity complete compression ultrasound (CCUS) testing for predicting the risk of PE-related death.
Methods The study assessed the ability of three diagnostic tests (cardiac troponin I (cTnI), echocardiogram, and CCUS) to prognosticate the primary outcome of PE-related mortality during 30 days of follow-up after a diagnosis of PE by objective testing.
Results Of 591 normotensive patients diagnosed with PE, the primary outcome occurred in 37 patients (6.3%; 95% CI 4.3% to 8.2%). Patients with right ventricular dysfunction (RVD) by TTE and concomitant deep vein thrombosis (DVT) by CCUS had a PE-related mortality of 19.6%, compared with 17.1% of patients with elevated cTnI and concomitant DVT and 15.2% of patients with elevated cTnI and RVD. The use of any two-test strategy had a higher specificity and positive predictive value compared with the use of any test by itself. A combined three-test strategy did not further improve prognostication. For a subgroup analysis of high-risk patients, according to the pulmonary embolism severity index (classes IV and V), positive predictive values of the two-test strategies for PE-related mortality were 25.0%, 24.4% and 20.7%, respectively.
Conclusions In haemodynamically stable patients with acute symptomatic PE, a combination of echocardiography (or troponin testing) and CCUS improved prognostication compared with the use of any test by itself for the identification of those at high risk of PE-related death.
- Echocardiography
- lower limb ultrasound testing
- prognosis
- pulmonary embolism
- troponin
Statistics from Altmetric.com
In the assessment and management of patients with acute symptomatic pulmonary embolism (PE), prognostic information helps to guide therapeutic decision-making. Clinicians use prognostic information (eg, risk of death from PE) to determine the need for escalation of care, such as admission to the intensive care unit (ICU) or the administration of thrombolytic therapy.1 The high risk of death in patients with PE and associated hypotension or shock may indicate the need for treatment more aggressive than standard anticoagulation (eg, thrombolysis).2 Limited data exist regarding the use of prognostic tools (or combination of tools) to identify subgroups of normotensive patients at high risk of PE-related death. Prognostic tools may assist with the identification of high-risk patients who may potentially benefit from escalated therapy.
Bedside echocardiography may detect right ventricular dysfunction (RVD) in patients with acute PE.3 Numerous studies, including two large registries, have demonstrated the prognostic relevance of echocardiography.4 5 However, echocardiographically detected RVD has a low positive predictive value for PE-related inhospital death.6 7 Some studies have thus investigated the prognostic role of the combination of a simple laboratory test (ie, measurement of the levels of a cardiac biomarker) and a non-invasive imaging method such as echocardiography.8–10 The inclusion of only a small number of haemodynamically stable patients in these studies has limited their applicability.
Massive or high-risk PE results whenever anatomical thrombus burden, cardiopulmonary reserve and cardiovascular response interact to produce haemodynamic instability.11 In this pathophysiological cascade, recurrent thromboembolic episodes may play a decisive role by ultimately destabilising a previously normotensive patient. A recent study of patients with acute symptomatic PE supported the thrombus burden poor prognosis hypothesis by demonstrating that those with evidence of concomitant deep vein thrombosis (DVT) had, compared with those without DVT, an increased risk of all-cause death, PE-related death and recurrent venous thromboembolism over 3 months of follow-up.12
This study aimed to investigate if a two-test or three-test strategy that utilises lower extremity complete compression ultrasound (CCUS) testing for DVT, cardiac troponin I (cTnI) testing for myocardial injury, and transthoracic echocardiography (TTE) testing for RVD might offer an advantage compared with each test alone with regard to the identification of high-risk haemodynamically stable patients with an objectively confirmed episode of acute symptomatic PE.
Methods
Patient identification and eligibility criteria
The study eligibility criteria required patients to have objectively confirmed symptomatic PE. The study excluded patients with haemodynamic instability at presentation (defined as cardiogenic shock, systolic blood pressure <90 mm Hg, or the need for inotropic support despite blood pressure measurements), those in whom the attending physician decided to give thrombolytic therapy and those who did not successfully complete the protocol-required troponin, CCUS and TTE testing.
Baseline examinations
The study established the diagnosis of PE in patients by the presence of a high probability ventilation-perfusion (V/Q) scintigraphy,13 a positive contrast-enhanced PE protocol, helical CT14 or, in patients with inconclusive ventilation–perfusion scans or negative CT scans and high subjective clinical suspicion, a lower limb venous compression ultrasonography positive for proximal DVT.15 Patients underwent bilateral proximal and distal lower extremity CCUS of the veins within 48 h after the diagnosis of PE. Trained and certified vascular surgeons, blinded to the patient's clinical information, used a standardised CCUS protocol and Toshiba (linear 4–7 MHz transducer) ultrasound equipment (Toshiba Nemio, Japan) to evaluate for DVT.16 The study used vein incompressibility as the diagnostic criterion for DVT. In patients with a history of DVT and an available CCUS record for review, CCUS diagnosed recurrent DVT by the appearance of a new non-compressible vein segment, or a 4-mm or more increase in the diameter of a thrombus. In patients with a history of DVT but without an available CCUS for review, CCUS diagnosed recurrent DVT if a non-compressible vein segment was accompanied by vein dilatation.
The study required that patients undergo echocardiography (ie, TTE) within 24 h after the diagnosis of PE. Trained and certified echocardiographers used a Phillips ultrasound system (Phillips Sonos Agilent, The Netherlands) and a 3.5-MHz transducer. Patients underwent testing in the left lateral position. A trained and certified cardiologist, blinded to the patient's clinical data, troponin I levels and CCUS results, interpreted each echocardiogram. The study defined echocardiographic RVD as dilatation of the right ventricle (end-diastolic diameter >30 mm from the parasternal view or the right ventricle appearing larger than the left ventricle from the subcostal or apical view), hypokinesis of the right ventricle free wall (any view), or tricuspid systolic velocity greater than 2.6 m/s from the apical or subcostal four-chamber view.17 18
The study required that patients undergo troponin testing within 12 h after the diagnosis of PE. Patients had blood samples collected from an antecubital vein at the time of hospital admission. The laboratory measured cTnI levels quantitatively using a microparticle enzyme immunoassay (Abbot, USA). The analytical sensitivity of 0.08 ng/ml for this cTnI represents the lowest measurable concentration of cTnI that can be distinguished from zero. The study defined cTnI concentrations of 0.1 ng/ml or greater as an indication of myocardial injury.
Each patient's baseline characteristics determined their risk classification according to the criteria for the predictive pulmonary embolism severity index (PESI) model.19 By summing the patient's age in years and the points for each predictor when present, each patient has a total PESI score calculated.
Study outcome measures
The study used PE-related mortality 30 days after the diagnosis of PE as the primary outcome. Investigators assessed mortality using patient or proxy interviews, and/or hospital chart review. Two independent experts (authors DJ and DM), blinded to initial prognostic test results, adjudicated all death causes as ‘definite fatal PE’, ‘possible fatal PE’, or ‘death from other causes’. The adjudicators classified the cause of death as ‘definite fatal PE’ if autopsy deemed PE as the cause of death, or if death followed and was apparently related to a clinically severe PE or an objectively confirmed recurrent event. Adjudicators classified death in a patient who died suddenly or unexpectedly as ‘possible fatal PE’. The study defined the composite outcome of a ‘complicated course’ as PE-related death, haemodynamic collapse, or adjudicated recurrent PE within the 30 days of follow-up.
Treatment and follow-up
Prognostic test results did not mandate treatment options. The clinicians initiated treatment within 24–48 h of PE diagnosis with therapeutic doses of subcutaneous low molecular weight heparin, combined with oral vitamin K antagonist therapy. The clinicians closely monitored the intensity of oral anticoagulant therapy until the international normalised ratio (INR) was stable and between 2.0 and 3.0. Thereafter, patients underwent INR assessment approximately twice a month. The study considered the quality of oral anticoagulation as suboptimal if 30% or more of all measured INR had a value of less than 2.0.20 In patients whose clinical status deteriorated after enrolment, the clinicians administered thrombolytic treatment and/or inotropic support as deemed appropriate.
Statistical analyses
Non-normally distributed (Kolmogorov–Smirnov test) continuous variables are expressed as median with corresponding 25th and 75th percentiles and compared using the Mann–Whitney U test. Baseline characteristics are described with counts and proportions for categorical data. Most continuous variables were dichotomised, and the proportions in each group are described. The analyses used χ2 or Fisher's exact tests to compare categorical data between groups. To estimate the outcomes of time to PE-related death, Kaplan–Meier probabilities were computed,21 and differences between the groups were assessed with the log-rank test. The study used logistic regression to assess whether the variables of troponin (presence or absence of test value >0.1 ng/ml), TTE (presence or absence of echocardiographic RVD) and CCUS (presence or absence of DVT) had an independent association with 30-day PE-related mortality, after adjusting for other variables that had a p value of less than 0.05 in the univariate analyses. A manual backward stepwise approach was used to develop the multivariate models. In the full models, variables with imbalance between the groups at baseline were considered for inclusion. Variables that showed evidence of confounding (ie, the coefficient of the variable group changed by more than 10% when removing that variable from the full model) for the effect of each test (ie, troponin, TTE and CCUS) on the outcome undergoing analysis were not removed from the model. All probability values were two-tailed. We used SPSS version 15.0 to calculate estimated OR and 95% CI from the binomial distribution.
To assess the test and performance characteristics of combinations of cTnI, TTE and CCUS variables, we estimated the positive predictive value and the positive likelihood ratio, as well as the sensitivity, specificity, negative predictive values and negative likelihood ratio for predicting the primary outcome.
Results
Study staff screened 722 consecutive patients with acute PE for eligibility. Haemodynamic instability excluded 38 (5%) patients from participation. Of the remaining 684 haemodynamically stable patients, the study excluded 3.6% (25 of 684 patients) because they did not have troponin levels assessed within 12 h after the diagnosis of PE. Other reasons for exclusion consisted of a technically inadequate or unavailable CCUS (n=28) or TTE (n=61), unavailability for follow-up (n=18) and refusal to give informed consent (n=21). Some patients had multiple reasons for exclusion. We enrolled the remaining eligible 591 patients (254 men and 337 women) (figure 1).
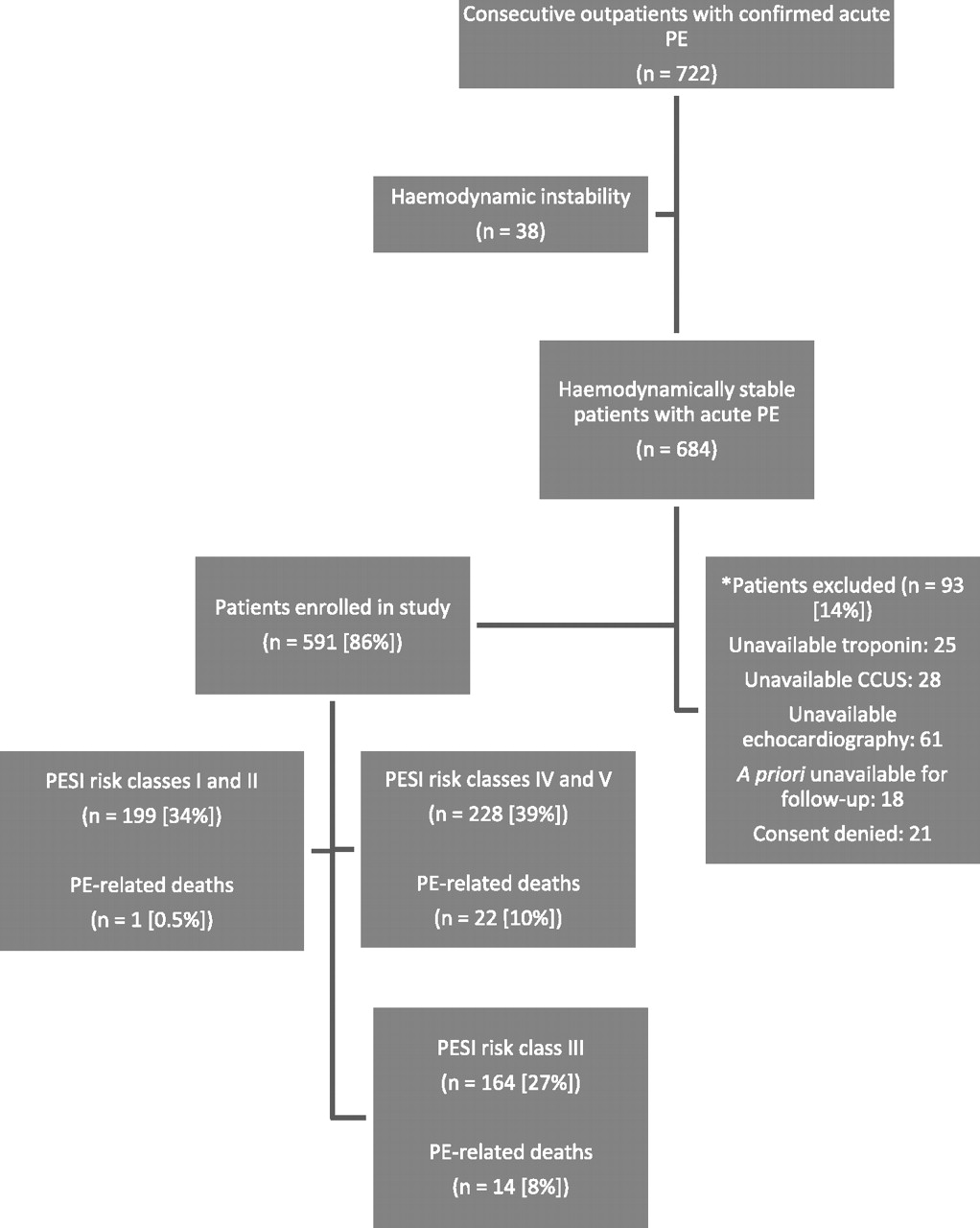
Patient flow diagram. PE, pulmonary embolism; CCUS, lower extremity complete compression ultrasound; PESI, pulmonary embolism severity index.19 *In 36 patients, echocardiography and CCUS were unavailable. In 17 patients, echocardiography and troponin testing were unavailable. In seven patients, CCUS and troponin testing were unavailable.
In the vast majority of patients, PE was diagnosed by a high probability V/Q scan (56%; 331 of 591 patients) or a positive PE protocol CT (47%; 278 of 591 patients). Diagnosis was based partly on CCUS results according to the diagnostic algorithm in 18 of the 591 patients (3.0%; 95% CI 1.7% to 4.4%). Of these 18 patients, eight had a non-diagnostic V/Q scan, four had a negative single-row detector contrast-enhanced helical chest CT, and six had a non-diagnostic V/Q scan and a negative single-row detector contrast-enhanced helical chest CT.
Table 1 shows the patients' clinical symptoms, predisposing conditions and relevant findings at presentation. Of the 591 patients, 120 (20.3%) had echocardiographic RVD, 190 (32.1%) had elevated cTnI levels and 228 (38.6%) had evidence of DVT on CCUS.
Clinical symptoms and relevant findings at presentation in 591 consecutive normotensive patients diagnosed with acute symptomatic PE in the emergency department
Fifty-nine of the 591 (10.0%; 95% CI 7.6% to 12.4%) normotensive patients with acute symptomatic PE died during the 30-day follow-up (table 2). Investigators adjudicated death as ‘definite’ or ‘possible’ fatal PE in 37 of these patients (67.3% of the total deaths; 95% CI 54.9% to 79.7%), corresponding to a cumulative rate of fatal PE of 6.3% (95% CI 4.3% to 8.2%) at 30 days after PE diagnosis.
30-Day clinical events after diagnosis and treatment for 591 normotensive patients with acute symptomatic PE
PE-related mortality within 30 days of diagnosis more frequently occurred in patients with elevated cardiac troponin levels (11% vs 4%; p=0.004), echocardiographic evidence of RVD (12% vs 5%; p=0.008), or CCUS evidence of DVT (10% vs 4%; p=0.009), compared with those without these findings. In the full models, arterial oxyhaemoglobin saturation, cancer and immobilisation were considered for inclusion. For the effect of troponin and TTE on the outcome undergoing analysis, no variables showed evidence of confounding (table 3). Multivariate logistic regression confirmed that CCUS-diagnosed DVT (OR 2.20; 95% CI 1.10 to 4.38; p=0.02) had an independent association with risk of death from PE during 30 days of follow-up, after adjusting for the other significant covariate of cancer at the time of acute PE diagnosis (table 3).
Factors associated with 30-day PE-related mortality in 591 normotensive patients with acute symptomatic PE
The study assessed the test characteristics (table 4) of cTnI, TTE and CCUS for prediction of 30-day PE-related mortality. The use of any two-test strategy had a higher specificity and positive predictive value compared with use of any test by itself. The combination of echocardiographic RVD and evidence of DVT on CCUS had the highest positive predictive value (although not statistically significant) of all two-test strategies. A three-test strategy that combined all three modalities (echocardiography, troponin and CCUS) only had a slight trend towards improvement of the prediction of PE-related death.
Prediction rule test characteristics for 30-day PE-related mortality in 591 normotensive patients with acute symptomatic PE
The PESI classified 228 of the 591 patients (38.6%; 95% CI 34.6% to 42.5%) as high risk (classes IV and V). Of these 228 PESI high-risk patients, 29 (12.7%) had elevated cTnI levels and echocardiographic RVD, 41 (18.0%) had elevated cTnI levels and DVT on CCUS, and 24 (10.5%) had echocardiographic RVD and evidence of DVT on CCUS. The PESI high-risk subgroup had a 30-day mortality of 17.1%. The positive predictive value and the positive likelihood ratio for PE-related mortality in these PESI high-risk patients with elevated cTnI levels and RVD on echocardiography were 20.7% and 2.44, compared with 24.4% and 3.02 in patients with elevated cTnI levels and DVT on CCUS, and 25.0% and 3.12 in patients with RVD on echocardiography and evidence of DVT on CCUS (table 5).
Prediction rule test characteristics for 30-day PE-related mortality in 228 patients deemed high risk by the PESI
Of the two-test strategies, the combination of echocardiography and CCUS had the best test characteristics of positive predictive value and positive likelihood ratio in all study patients and in the high-risk subgroup. Kaplan–Meier analysis confirmed the presence of a significantly higher PE-related mortality in patients with RVD assessed by echocardiography and concomitant DVT compared with those without both positive tests (p<0.001, log rank test; figure 2).

{kind=link}
{kind=link}
Kaplan–Meier survival curves of normotensive patients with acute symptomatic pulmonary embolism, stratified by the presence or absence of right ventricular dysfunction (RVD, by echocardiogram) and concomitant deep vein thrombosis (DVT, by lower extremity complete compression ultrasound) at the time of pulmonary embolism diagnosis. Log rank p<0.001.
Discussion
This study demonstrated that the combination of markers of RVD (by echocardiography) or myocardial injury (using cardiac troponin I testing) and assessment of thrombotic burden (using CCUS) improved the identification normotensive patients with acute symptomatic PE at high risk of 30-day death from PE. In particular, for the identification of high-risk normotensive patients with acute PE, (1) single prognostic tests (ie, troponin, CCUS, or echocardiography) had limited usefulness; (2) the positive likelihood ratio of PE-related mortality doubled with the addition of a second test; (3) a three-test strategy did not have test characteristics much better than the two-test strategy; and (4) the two-test strategies had higher positive predictive values in PESI high-risk patients.
The recent guidelines by the European Society of Cardiology22 proposed to distinguish between high-risk patients with acute PE (ie, clinically evident right ventricular failure with refractory arterial hypotension and shock) and non-high-risk patients with acute PE (ie, the absence of overt haemodynamic instability). For high-risk patients, the more recent guidelines of the European Society of Cardiology22 and the American College of Chest Physicians2 strongly recommend the use of thrombolysis. The guidelines and literature do not provide clear recommendations regarding whether, and by what means, a high-risk group can be identified among normotensive patients with acute PE, and whether this particular group may benefit from more aggressive therapy such as thrombolysis.
Previous studies of patients with acute PE yielded equivocal findings regarding the performance of test combinations for prognosticating PE-related and PE-unrelated short-term adverse events. For example, the study by Kostrubiec et al23 of 100 consecutive, normotensive patients with PE found a positive predictive value of 33% for PE-related death in the subset of patients with elevated troponin and N-terminal pro-brain natriuretic peptide levels. The addition of echocardiographic data to the blood test data did not improve the test characteristics. In the study by Kucher et al9 of 91 stable and unstable patients with acute PE, the combination of troponin I and echocardiography had improved prognostic value compared with each test alone. In the study by Scridon et al10 of 141 patients with acute PE, those with echocardiographic right ventricular enlargement and elevated troponin levels had a 30-day all-cause mortality of 38%. The variability of considered endpoints, lack of an independent adjudication of the outcomes and shortcomings in the study designs may explain the discrepant findings between the previous studies and the current study.
This study showed a positive predictive value for PE-related death with any two-test strategy of approximately 15%, which did not significantly differ from the MAPPET registry positive predictive value of 14% for the PE-related death rate in the study's hypotensive group.5 These two-test strategies thus appear to identify a high-risk subgroup of normotensive patients with acute PE. In the patients with echocardiographic RVD, the detection of residual venous thrombosis by CCUS suggests that an elevated risk of recurrent PE exists. Such a recurrence could destabilise these marginally stable patients. For situations in which clinicians do not have echocardiography available, the use of troponin with CCUS provides a practical alternative. Indeed, in our cohort, the largest number of patients had to be excluded based upon the absence of an available or technically adequate echocardiogram.
The PESI has reliably and accurately identified patients at low risk of death when evaluated over periods of follow-up ranging from 7 to 90 days,24 and studies have suggested that clinicians could use the PESI to identify patients with acute PE who might undergo complete or partial outpatient treatment.25 Alternatively, clinicians should aim to identify the subgroup of haemodynamically stable patients among those classified as high risk according to the PESI who might benefit from more intensive surveillance or more aggressive therapy (ie, thrombolysis). In our study, the combination of right heart dysfunction (by either echocardiography or troponin testing) and residual DVT by CCUS in these high-risk patients had the highest positive predictive value for PE-associated 30-day mortality. The two-test strategy of troponin and CCUS may have more appeal than the combination of echocardiography and CCUS as both strategies had similar positive predictive values.
This prognostic tool validation study demonstrated several strengths that pertain to the identification of high-risk normotensive patients during initial acute PE therapy. The study evaluated a large (n=591) population of consecutive normotensive patients with symptomatic, objectively confirmed acute PE. Study staff collected detailed baseline data on all patients. All patients underwent anticoagulant therapy, irrespective of prognostic markers results. The study used PE-related mortality as the primary outcome in these high-risk normotensive patients because they may have the highest likelihood of benefit from thrombolytic therapy. The study used a priori diagnostic criterion for PE-related deaths. All patients had completed follow-up information available, and an independent committee adjudicated all events.
Some study methodological limitations affect the findings and interpretation of the study. The study could not estimate the potential impact of the intensity of treatment on patient outcomes, because the study staff did not consistently collect this information. The study included only patients who had echocardiograms, CCUS, and troponin testing performed near the time of the PE diagnosis. We cannot exclude that selection bias occurred. Finally, no universally accepted definition of echocardiographic criteria for RVD exists, and our measurements may have differed from those used by other groups.26
In summary, the study demonstrated that a two-test strategy that evaluated normotensive patients with acute symptomatic PE for RVD and concomitant DVT identified a subset of patients at high risk of PE mortality in the 30 days following PE diagnosis. In normotensive patients deemed high risk by the PESI, the two-test strategy had improved prognostic characteristics over a single-test strategy. As the study did not directly assess the impact of risk stratification on the management of PE, the benefit of more aggressive therapy (ie, thrombolysis) for these patients should undergo testing in a prospective, randomised trial.
References
Footnotes
See Editorial, p 2
Linked articles 151316.
Funding This study was supported by a FIS (080200) and a SEPAR (2008) grant.
Competing interests None.
Ethics approval This study was conducted with the approval of the Ramon y Cajal Hospital, Madrid, Spain.
Provenance and peer review Not commissioned; externally peer reviewed.