Article Text

Abstract
Objectives: To provide nationally representative data on trends in HIV testing in primary care and to estimate the proportion of diagnosed HIV positive individuals known to general practitioners (GPs).
Methods: We undertook a retrospective cohort study between 1995 and 2005 of all general practices contributing data to the UK General Practice Research Database (GPRD), and data on persons accessing HIV care (Survey of Prevalent HIV Infections Diagnosed). We identified all practice-registered patients where an HIV test or HIV positive status is recorded in their general practice records. HIV testing in primary care and prevalence of recorded HIV positive status in primary care were estimated.
Results: Despite 11-fold increases in male testing and 19-fold increases in non-pregnant female testing between 1995 and 2005, HIV testing rates remained low in 2005 at 71.3 and 61.2 tests per 100 000 person years for males and females, respectively, peaking at 162.5 and 173.8 per 100 000 person years at 25–34 years of age. Inclusion of antenatal tests yielded a 129-fold increase in women over the 10-year period. In 2005, 50.7% of HIV positive individuals had their diagnosis recorded with a lower proportion in London (41.8%) than outside the capital (60.1%).
Conclusion: HIV testing rates in primary care remain low. Normalisation of HIV testing and recording in primary care in antenatal testing has not been accompanied by a step change in wider HIV testing practice. Recording of HIV positive status by GPs remains low and GPs may be unaware of HIV-related morbidity or potential drug interactions.
Statistics from Altmetric.com
HIV prevalence has increased in the UK over the last decade with an estimated 73 000 individuals living with HIV by 2006 of whom 21 000 remained undiagnosed.1 HIV patients’ medical care has historically been managed by stand-alone HIV specialist services of which the larger provide some primary care services.2 The number of HIV positive individuals requiring these services has increased threefold since the mid-1990s as a consequence of new diagnoses and improved survival following the introduction of highly active antiretroviral therapy (HAART) around 1996.1 While HIV services can ensure a high quality of HIV care for diagnosed individuals, GPs report anecdotally that overall clinical care may be compromised where a general practitioner (GP) is unaware of their patient’s HIV status and other treatments.3 There is evidence that close liaison between specialist HIV services and primary care can shorten admissions and improve the standard of health care in this group generally.4
Primary care remains a relatively under-used resource for the delivery of sexual health services other than contraception. England’s National Strategy for Sexual Health and HIV proposes enhancement of sexual health services in general practice, including HIV testing, in order to reduce high mortality rates among individuals diagnosed late and to reduce transmission associated with undiagnosed infection.5 Universal offer of HIV testing to pregnant women began in 20006 as it became clear that neonatal transmission is preventable and uptake of antenatal testing practitioner-dependent.7 8 While the success of this policy demonstrated the feasibility of HIV testing in a non-specialist setting,9 no framework existed for delivering HIV testing in the wider population until recent recommendations for testing in primary care and in other health settings.10 11 Many patients diagnosed with acute12 and established13 HIV infection consult prior to diagnosis in primary care and often miss opportunities for earlier diagnosis.
In this study we aimed to provide the first nationally representative estimates of testing rates and recording of positive HIV status in primary care.
Methods
Briefly, HIV testing rates and prevalence of recorded HIV in primary care were estimated using disaggregated data from a large primary care database, the General Practice Research Database (GPRD), broadly representative of the UK population and containing 2.8 million current patients in 2005. Incidence of HIV testing in males, and females with and without antenatal screening, was estimated. The prevalence of recorded HIV positive status in the GPRD was compared with a denominator of all HIV positive individuals reported to the surveillance dataset SOPHID (Survey of Prevalent HIV Diagnosed). This allowed us to estimate the proportion of all HIV positive individuals whose status was coded in their general practice record.
Population and sampling
The GPRD is a large anonymised primary care database derived from computerised clinical records produced during consultations in primary care. It contains anonymised data on 4.7% (2.8 million in 2005) of the UK population. The Medicines and Healthcare products Regulatory Agency (MHRA) holds the licence for the database and undertakes checks on the quality and completeness of data, which have been collected continuously since 1988. The GPRD is broadly demographically representative of the UK population, although there is a slight under-representation of inner London and Scotland. It has been used and validated for many pharmacoepidemiological, epidemiological and public health uses,14 with a denominator of 296 098 person-years of observation available to us for 2005. GPs enter medical diagnoses and symptoms using Read codes15 or the similar but now superseded Oxmis (Oxford Medical Information Systems) codes. Read and Oxmis codes are alphanumeric hierarchical codes that have an associated text description, which are used to summarise information on diagnoses, symptoms, examination and referral in UK primary care in coded form. Their scope is more diverse than International Classification of Disease (ICD)-10 disease codes and some are ambiguous (for example, “chlamydia”) or non-specific (“unspecified chronic viral infection”). In addition, investigations, prescription data, and consultation data, age, gender and Strategic Health Authority (SHA) of residence are recorded for each registered individual.
Practice level quintiles of Index of Multiple Deprivation for 2004 (IMD 2004) score were used as a proxy for the level of deprivation but ethnicity data were not available. Individual level linkage to other datasets was not available.
We classified GPRD practices as rural or urban at super output area level (a small area geographic boundary) in England, Wales and Northern Ireland, and by NHS region in Scotland, using data from national statistics providers.
Definitions of HIV testing and recorded HIV positive status
In total, 33 codes were identified denoting a definite HIV test (see online supplementary material Appendix 1) and 61 codes referring to HIV status, of which 56 codes denote a definite HIV positive status (see online supplementary material Appendix 2 for details). Individuals who had any medical code recorded in the GPRD denoting definite HIV positive status were subsequently defined as having recorded HIV positive status. An HIV test was considered to be “antenatal” if it occurred within 6 months of any medical code indicating a current pregnancy.
Estimation of HIV testing rate in primary care
We estimated the incidence of HIV testing during the time period 1995–2005 for males and females, including and excluding antenatal tests, using the GPRD registered population as denominator for person-years at risk. Survival analysis was used to calculate person-years-of-exposure at risk of HIV testing. Poisson regression was used to calculate 95% confidence intervals (CIs) and incidence rate ratios (IRRs). Testing rates (excluding antenatal tests) were estimated by age group, gender, SHA, IMD and rural/urban category, and area of residence (London vs outside London) for 2005.
We restricted counts of patients’ HIV test records to at most one test in any 90 day period. HIV test events are often duplicated in the GPRD due to the nature of data recording in general practice. For example, a patient may have an HIV test in general practice recorded in their medical records, while the corresponding laboratory test result may be recorded in their test records 2 weeks later. In addition, current surveillance from specialist clinics reports only one test in each 3 month period.1 This approach also allows for one test only within the “window period” of 90 days after exposure to HIV, which can be regarded as a single episode of testing. Therefore, we have used the same definition of a 3-month period to allow for comparisons with other work. (Our data show that in 2005, 5.4% of all male and 2.2% of all female tests were recorded within this 90 day period with little evidence of change over time.)
Recorded HIV positive individuals were removed from the denominator for HIV testing incidence calculations as they are no longer “at-risk” of HIV infection or testing.
Estimating the prevalence of HIV recorded in primary care
Prevalence of recorded HIV in primary care was calculated for the years 1995–2005 for males and females with a more detailed breakdown by age and demographic characteristics for 2005 only. The proportion of all diagnosed cases recorded in the GPRD was estimated by comparing recorded prevalence in the GPRD population as numerator, with age and sex-specific reports to the SOPHID surveillance system (see below) as denominator.
In the GPRD, prevalence of recorded HIV infections in general practice was calculated using the number of patients registered as at 30 June (mid-year) as the denominator. HIV infection is most commonly diagnosed in genito-urinary medicine (GUM) clinics or elsewhere in secondary care settings after which HIV positive patients may or may not inform their GP.16 Practice software allows separate recording of the date of a diagnosis and the date of a first consultation relating to that diagnosis. Therefore, the GPRD patient record may in some cases give two different dates for first HIV diagnosis: an “event date” (for example, the date on which the diagnosis was made elsewhere), which could precede the “consultation date” (for example, date of first consultation in primary care when HIV was discussed and recorded by the GP). For this analysis we used the first date on which HIV positivity was recorded in the primary care record.
SOPHID is an annual survey of all persons attending at least once for HIV care in specialist services across the UK and represents the best available estimate of the diagnosed prevalence of HIV in the UK.17 It was used as the denominator from which to estimate the proportion of HIV cases recorded in the primary care record. Individual anonymised data are collected and analysed by the Health Protection Agency. Mid-year population estimates were obtained from the UK’s Office of National Statistics (ONS) as the denominator for UK HIV prevalence estimates.
Other
For all analyses we defined the population of London as the five pre-2006 SHAs with all other UK regions classed as outside the capital using data provided by the ONS.
Data analysis was performed using STATA (version 9.0).
Results
A total of 13.8 million person years of observation was available for males and 13.9 million for females. We identified 28 447 HIV tests in the GPRD during the study period 1995–2005. In 1995, 147 males and 45 females contributing data were recorded as HIV positive by the end of the year and by 2005 this had risen to 776 and 413, respectively.
HIV testing in primary care
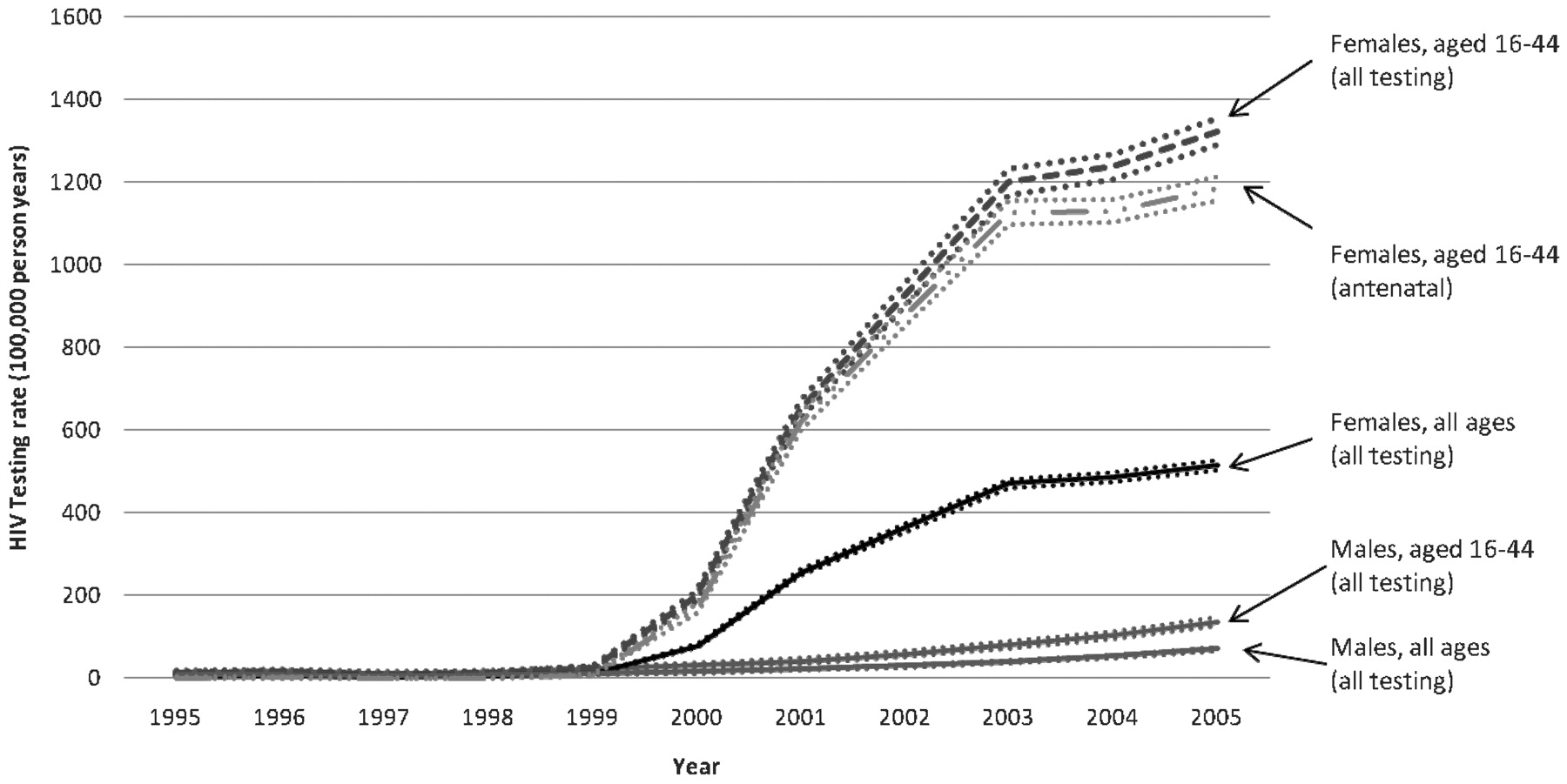
Figure 1 summarises trends in HIV testing during the study period with rates for the age groups 16–44 and non-antenatal testing shown separately. The period 1995–2005 saw an 11-fold increase in HIV testing rates among males and a 129-fold increase in all women reaching 514.5 per 100 000 women in 2005. However, when antenatal tests were excluded, the increase among females reduced to 19-fold, and annual testing rates remained lower in females (61.2 per100 000 person-years) than in males (71.3 per100 000 person-years) in 2005 (exact numbers are given in table 1 of the supplementary online material).
{kind=link}
HIV testing in general practice, all ages and ages 16–44 years by gender, and antenatal testing rates among females 16–44 years between 1995 and 2005 with 95% CI.
Tables 1A and 1B show HIV testing by age, sex and demographic characteristics. In 2005, testing incidence (excluding antenatal) among patients living in London was more than double the rate seen elsewhere in the UK in both sexes (IRR 2.1; 95% CI 1.8 to 2.4) and 2.2 (95% CI 1.9 to 2.6) for males and females, respectively. Outside London, testing rates were highest among adults aged 25–34 in both sexes (156.2 and 162.3 per 100 000 person-years, respectively). However, in London, testing was higher among both male and female adults aged 35–44 years (263.9 and 271.9 per 100 000 person-years, respectively). Among females testing varied by level of deprivation with more testing in deprived settings. Individuals in non-urban areas were less likely to test.
Rates (per 100 000 person-years) of HIV testing recorded in general practice in 2005 by age group, deprivation level and rural/urban indicators, stratified by London versus outside of London, males
Rates (per 100 000 person-years) of HIV testing recorded in general practice in 2005 by age group, deprivation level and rural/urban indicators stratified by London versus outside of London, females, excluding antenatal tests
Prevalence of recorded HIV positive status in primary care and how it compares with SOPHID data
Table 2 shows trends in the prevalence of recorded HIV positive status in the GPRD, separately and as a proportion of SOPHID cases. An estimated 50.7% (95% CI 47.9 to 53.7%) of HIV positive individuals had their status recorded in coded form in their primary care record in 2005—a proportion which changed little in the period between 1995 and 2005. Prevalence of HIV recorded in primary care increased in parallel with HIV diagnosed prevalence in SOPHID, but the proportion of diagnosed individuals having their HIV status recorded in primary care remained relatively constant. Throughout, recording remained lower in London than elsewhere, with the proportion declining to 41.8% in 2005, by contrast with an increase to 60.1% outside the capital city.
Prevalence of diagnosed HIV (SOPHID), HIV recorded in primary care (per 100 000 persons) and the proportion of HIV recorded in primary care between 1995 and 2005 in London and outside London
Table 3 shows estimates of recorded positive status by age, sex and demographic characteristics in 2005. Recording was less likely for men and women aged 25–34 years (36.4% males and 40.0% females) than older adults (61.0% males and 73.2% females over 45 years) or children less than 16 years (table 3).
Prevalence of recorded diagnosed HIV in primary care (per 100 000 persons) and the estimated proportion of HIV recorded in primary care in 2005 among males and among females by age group
Discussion
HIV testing increased substantially (11-fold in males and 19-fold in non-pregnant females) in the primary care setting between 1995 and 2005. These increases were small in comparison with increased antenatal testing.
Only half of all HIV positive individuals are recorded as such in the primary care records. This proportion remained consistently lower in London than elsewhere and did not change despite rising prevalence over the decade.
This study provides the first nationally representative estimates of testing rates and recording of positive HIV status in primary care. Only a small proportion of HIV tests have traditionally been taken in primary care. Chadborn and colleagues estimated that 6.6% of tests in London and 13.0% of tests outside London were taken in this setting in the decade to 2000.16 A number of studies have confirmed that many late presenters, who face increased mortality, have consulted in primary care in the 12 months prior to diagnosis.18 19 Our data demonstrate that while a large number of antenatal HIV tests are routinely documented in primary care, expansion of antenatal testing has not been accompanied by a wider step change in testing patterns.
The steady rates of recording in primary care, during a period in which HAART has transformed prognosis and increased prevalence, are surprising, particularly in London. Lower recording in London may relate to lower disclosure rates, to patients’ difficulties in accessing primary care or fear of disclosure among migrants who continue to form a high proportion of all HIV cases and are often resident in London.1 However, earlier studies demonstrated high rates of GP registration and consultation even among these vulnerable groups,20 21 and this does not fully explain the low recorded rates seen in the capital. No data are available on patterns of computerised coding practice for HIV in primary care and these may have changed over time.
While benefiting from nationally representative data, our study has a number of limitations. We may be underestimating HIV testing and disclosure in primary care, particularly in earlier years before widespread implementation of electronically recorded laboratory results, which are more likely to lead to a recorded test code than paper results. Antenatal testing may also be underestimated since women can be tested elsewhere (for example, a hospital or community antenatal visits) and negative results may not appear in the primary care record. We have not sought to match our estimates to antenatal HIV testing surveillance for this reason. Not all cases of HIV disclosed to GPs will be coded as such in the notes—“euphemism” codes such as “chronic viral illness” may be used, information may be hidden in non-coded free text or not recorded at all. Recorded HIV diagnoses are a combination of HIV incidence and prevalence, with patients registering, presenting and disclosing to GPs and then GPs entering this onto the clinical record. Anecdotal information sought from GPs during the study suggests that recording practice has been variable but that precise coding is more likely in recent years.
We also cannot reliably determine a true “incident” date of HIV diagnosis nor which cases were diagnosed in primary care. Initial HIV positive tests from a laboratory are normally notified to a GP by telephone for confirmatory testing (which may then be conducted in GUM settings). These do not automatically generate a coded entry and so cannot be distinguished from cases diagnosed elsewhere.
The lack of ethnicity data in the GPRD means that we cannot reliably interpret the relationship between our findings and recent demographic changes in the UK HIV epidemic. We were not able to explore the extent to which non-recording is concentrated in different ethnic groups and in particular among black Africans who may have concerns about migration and healthcare entitlements, which discourage disclosure to the GP. Sexual orientation may not be known to the GP and we are unable to estimate recording or testing rates among men who have sex with men from our data. Finally, biases introduced by under-representation of London practices cannot be accurately assessed.
It is increasingly recognised in UK policy that normalisation of HIV testing in primary care, on the scale already seen in the context of antenatal care, will be required in order to reduce the pool of undiagnosed prevalence,22 23 and national guidelines aimed at achieving this have recently been published.10 The Center for Disease Control and Prevention (CDC) in the USA recommends opt-out HIV testing for all adults attending any healthcare facility, aimed at decreasing late presentation with symptomatic HIV/AIDS and onward transmission.24 Given that a third of HIV infected individuals are undiagnosed, and a third of all those newly diagnosed present late in the course of their infection,1 25 there is a need to expand HIV testing in primary care as well as other healthcare settings.
Surveillance of HIV testing in the primary care setting is essential to measure uptake and to ensure its feasibility, acceptability and cost-effectiveness. Our data demonstrate the feasibility of using large primary care databases to monitor testing rates at national level. Further work is needed on the mechanisms required to deliver increased HIV testing in primary care. Detailed studies that explore barriers to the recording of positive HIV status in primary care and its relationship to the delivery of care to HIV positive individuals could contribute to the planning of services for this group.
Key messages
Little is known about HIV testing in primary care, or the extent of disclosure of HIV positivity to GPs, despite the importance of early diagnosis.
HIV testing rates in primary care increased slowly but remained low in the decade to 2005 and were highest in young adults.
GPs test for HIV more in London and other urban areas.
Less than half of all HIV positive individuals are recorded as such by their GPs and with a lower proportion in London where HIV is concentrated.
REFERENCES
Supplementary materials
Web Only Data sti.2008.034801
Files in this Data Supplement:
Footnotes
▸ Additional materials are published online only at http://sti.bmj.com/content/vol85/issue7
Funding This work was funded by the Medical Research Council, with funding allocated from the Health Departments, under the aegis of the MRC/UK Health Departments Sexual Health and HIV Research Strategy Committee.
Competing interests None.
Ethics approval No study specific ethics approval was required. The protocol was submitted to the Independent Scientific Advisory Committee for the GPRD who approved it under delegated authority.
The Medical Research Council has had no role in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper publication. The views expressed are those of the authors and not necessarily those of the MRC or the Health Departments.
Contributors: JC had the original idea for the study and developed a detailed proposal for funding alongside CM, GR, MGB, VD, AMJ, SS, GH, TW and IP. Code lists were developed and refined by all members of the team, particularly MH, MGB, GH and JC. HE undertook all analyses under the supervision of CM and JC, with input from all other members of the team. VD and TC led the provision, use, analysis and interpretation of SOPHID data. HE wrote the first draft and all authors contributed to and commented on subsequent versions. JC acted as guarantor.
Provenance and Peer review Not commissioned; externally peer reviewed.