Article Text

Abstract
Aim: To analyse mutations in the gyrA and parC genes leading to possible increase in ciprofloxacin resistance (high MIC values for ciprofloxacin) in clinical isolates of Neisseria gonorrhoeae in Delhi, India.
Method: MIC of ciprofloxacin for 63 clinical isolates of N gonorrhoeae were examined by the Etest method. Subsequently, gyrA and parC genes of these isolates were amplified and sequenced for possible mutations.
Results: Out of the 63 clinical isolates tested, only five (8%) isolates were found to be susceptible to ciprofloxacin (MIC <0.06 μg/ml). DNA sequence analysis of the gyrA and the parC genes of all these isolates (n = 63) revealed that all isolates which were not susceptible to ciprofloxacin (n=58) had mutation(s) in gyrA and parC genes. 12 isolates (19%) exhibited high resistance with an MIC for ciprofloxacin of 32 μg/ml. Two out of these 12 isolates (UD62 and UD63), harboured triple mutations (Ser-91 to Phe, Asp-95 to Asn and Val-120 to Leu) in the gyrA gene. The third mutation of Val-120 to Leu, lies downstream of the quinolone resistance determining region (QRDR) of the gyrA and has not been described before in gonococcus. In addition, both these isolates had a Phe-100 to Tyr substitution in the parC, a hitherto unknown mutation.
Conclusions: Emergence of ciprofloxacin resistance with high levels of MIC values (up to 32 μg/ml) in India is alarming. Double and triple mutations in gyrA alone or together in gyrA and parC could be responsible for such a high resistance.
- ciprofloxacin
- Neisseria gonorrhoeae
- novel mutations
- gyrA gene
- parC gene
- India
Statistics from Altmetric.com
N eisseria gonorrhoeae, a common causative agent of sexually transmitted diseases (STD), is still prevalent in high numbers in developing countries.1,2 Owing to the emergence of penicillin and tetracycline resistant strains of N gonorrhoeae, CDC and WHO recommended third generation cephalosporins and fluoroquinolones for the treatment of gonococcal infections worldwide, including India.3,4 However, the decreased susceptibilities of N gonorrhoeae to fluoroquinolones has recently been reported from a large number of countries.5–12 Ciprofloxacin, a fluoroquinolone, inhibits DNA replication by targeting DNA gyrase and topoisomerase IV.13,14 In laboratory mutants of N gonorrhoeae, mutations in the gyrA and gyrB genes of DNA gyrase and in the parC gene of topoisomerase IV, associated with decreased susceptibilities to quinolones, have been identified.15–18 An amino acid change in the GyrB tends to confer a low level resistance to nalidixic acid.16 Alterations in the ParC have been identified only in strains having GyrA mutations and had a complementary role in further decreasing susceptibility of N gonorrhoeae to fluoroquinolones.11,15,17,18
The present study was performed to examine the susceptibility to ciprofloxacin of N gonorrhoeae isolated from clinical samples (n = 63) collected from patients visiting Safdarjung Hospital, Delhi, India, from January 2000 to March 2001. The studies were further extended to understand the sharp increase in ciprofloxacin resistance, observed in Delhi, and to find out a correlation between mutation patterns in gyrA and the parC genes and the level of ciprofloxacin resistance.
MATERIALS AND METHODS
Gonococcal isolates
A total of 78 male patients with signs and symptoms of acute gonococcal urethritis attending the STD Teaching and Research Centre of Safdarjung Hospital in New Delhi, India, from January 2000 to March 2001 were investigated for the presence of Gram negative intracellular diplococci in their urethral discharge. A total of 63 samples were smear positive. Specimens from these smear positive patients were inoculated directly onto Thayer-Martin selective agar (Hi Media, India), and incubated for 24–48 hours at 35oC in a humid atmosphere containing 5–10% CO2 (candle extinction jar).19 The culture positive isolates were further confirmed as N gonorrhoeae by colony morphology, Gram staining, oxidase test, and carbohydrate degradation test.19 Post-treatment isolates or repeat isolates from the same patients were excluded in this study.
Susceptibility testing
The MIC of ciprofloxacin was determined by the Etest method in all the culture positive isolates (63 cultures) using the steps suggested by the manufacturer (AB Biodisks, Solna, Sweden). An inoculum of 107 cfu/ml was allowed to grow on chocolate agar medium for 24 hours in a candle extinction jar.19 Based on MIC values, the strains were labelled as susceptible (MIC <0.06 μg/ml), intermediate resistant (MIC 0.06 μg/ml to 0.75 μg/ml), and resistant (MIC ≥1 μg/ml).20 WHO A-E, H, and J strains were used as controls.21
Molecular study
The gyrA and parC genes of each of the gonococcal isolate were amplified using oligonucleotide primers as reported by Tanaka et al.11 These primers amplified gyrA gene from nucleotides 160–438 (278 bp product), corresponding to the amino acids 54–146. The 255 bp amplified product of parC gene represented the nucleotides 166–420, which corresponds to amino acids 56–140.15 Chromosomal DNA was extracted by standard methods22 and the PCR amplification was performed in 50 μl of a reaction mixture which contained 5 μl of 10x Taq polymerase buffer (500 mM KCl, 100 mM TRIS-HCl (pH 8.3), 15 mM MgCl2, 0.1% gelatin), 25 pmol of each of the two primers (reverse and forward), 200 μM of each of the four deoxynucleoside triphosphates (New England Biolabs, Inc, USA), 1.5 U of Taq DNA polymerase (BangaloreGenei India Pvt Ltd, India), and 100 ng of template DNA. Thirty five cycles were performed for each reaction. Each cycle consisted of 30 seconds at 93°C, 1 minute at 52°C, and 1 minute at 72°C. The amplified PCR product was separated by electrophoresis on agarose gel and eluted from agarose by using a DNA isolation kit from Biological Industries, Israel, as in the manufacturer’s instructions. The purified DNA was air dried and suspended in 12–15 μl of sterile water. Gel purified PCR amplified product (100 ng) of gyrA gene was digested with Hinf1 (1 unit) in a final volume of 10 μl for 2 hours at 37°C. The digests were subjected to electrophoresis on 1.5% agarose gel and visualised by ethidium bromide staining. Purified PCR amplified product of gyrA (corresponding to 160–438 nucleotides) and parC (corresponding to 166–420 nucleotides) genes of all the isolates as well as WHO reference strains A, H, and J, were subjected to DNA sequencing using PCR primers (forward primer) with a Taq-Dye Terminator cycle sequencing kit and a Model 377A autosequencer (Applied Biosystems) as in the manufacturer’s instructions. The region sequenced includes the quinolone resistance determining region (QRDR) of the GyrA protein (amino acids 55 to 110) and the ParC protein (amino acids 66–119). DNA sequences were analysed using the blast program.
RESULTS
Susceptibilities of clinical isolates to ciprofloxacin
Table 1 shows the MIC values of ciprofloxacin for the 63 gonococcal isolates. The susceptibility pattern of N gonorrhoeae isolates was based on criteria proposed by Knapp et al.20 Only five isolates (8%) were found to be susceptible to ciprofloxacin with an MIC <0.06 μg/ml. Out of the 58 quinolone resistant N gonorrhoeae (QRNG) isolates, 23 (36%) isolates were exhibiting intermediate resistance towards ciprofloxacin (MIC values ranging from 0.06–0.75 μg/ml), while 35 isolates (56%) were resistant to ciprofloxacin with a wide range of MIC (1–32 μg/ml). Among these 35 resistant isolates, 12 isolates (35%) exhibited high levels of resistance with an MIC for ciprofloxacin of 32 μg/ml.
Susceptibility to ciprofloxacin of Neisseria gonorrhoeae isolated in India and the number of GyrA and ParC alterations
Hinf1 digestion to screen mutations in gyrA gene
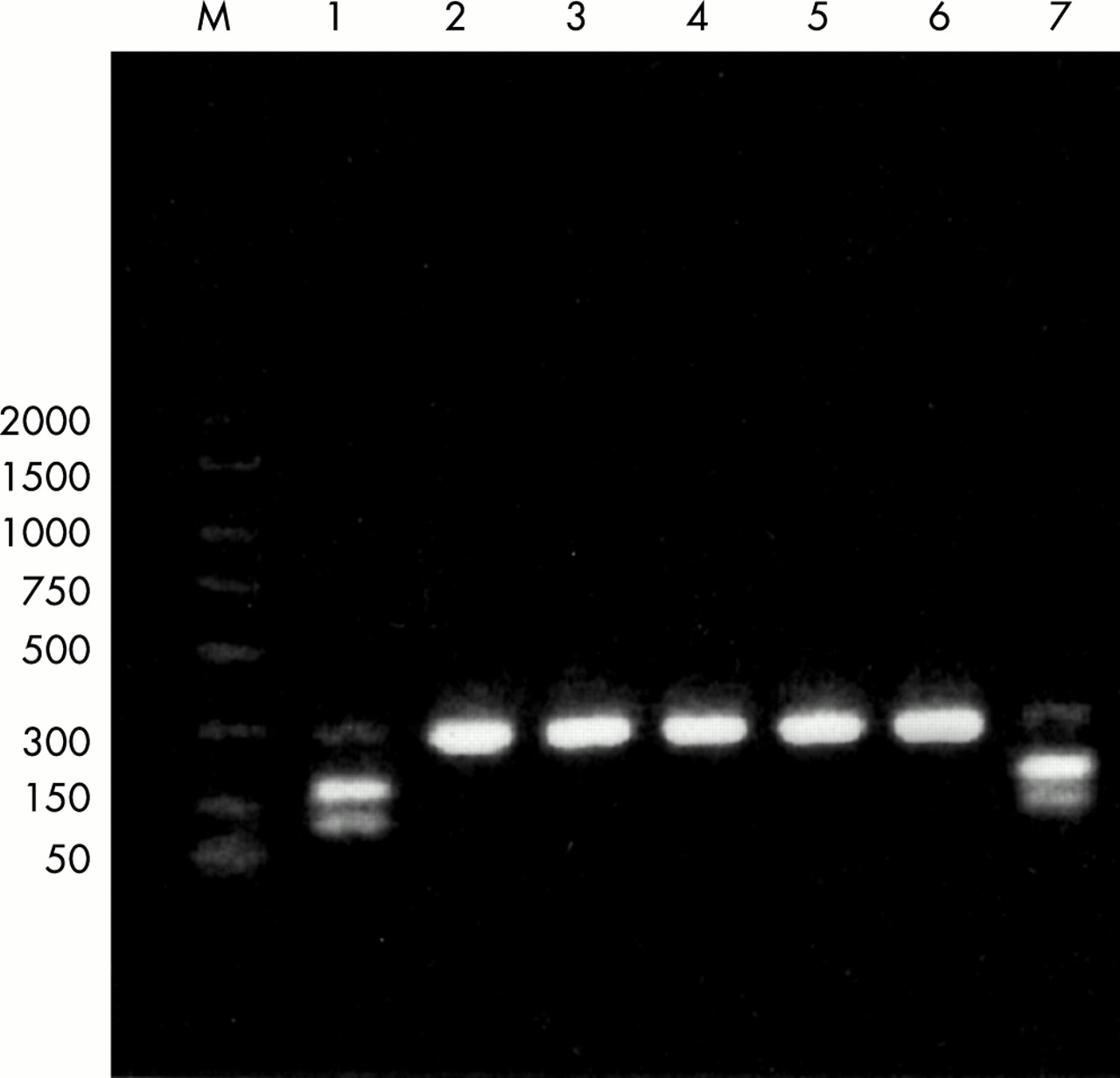
Quick screening of all the isolates, for the mutation at the Ser-91codon in gyrA gene, was done by Hinf1 restriction endonuclease digestion. PCR amplified gyrA gene product (278 bp) of all the isolates, which were susceptible to ciprofloxacin, when digested with the Hinf1 restriction endonuclease enzyme gave two bands of 165 bp and 113 bp on the agarose gel (fig 1). However, PCR products of gyrA gene, amplified from all other isolates, were not digested with Hinf1. The amplified products of the gyrA gene of WHO reference strains H and J (resistant to ciprofloxacin) were also resistant to digestion with the Hinf1 enzyme while that of WHO strain A (sensitive to ciprofloxacin) gave two bands of 165 bp and 113 bp (fig 1). Thus, all the gonococcal isolates, resistant to ciprofloxacin (n=58), were found to be mutated at Ser-91 position within QRDR of GyrA protein.

{kind=link}
Hinf1 restriction fragment length polymorphism. Region spanning QRDR of gyrA gene of Neisseria gonorrhoeae was amplified and subjected to Hinf1 restriction enzyme digestion. Ciprofloxacin susceptible isolates (lane 1; susceptible clinical isolate, lane 7; WHO reference strain A) with no mutation produced two fragments of 165 bp and 113 bp on Hinf1 digestion. The ciprofloxacin resistant isolates (lanes 2–4; QRNG clinical isolates, lane 5; WHO reference strain H, lane 6; WHO reference strain J) remain undigested as Hinf1 cleavage site is lost because of the C to T transition at nucleotide position 272 (Ser-91 to Phe). Lane M; 100 bp molecular weight standard.
Novel mutations in gyrA and parC genes in isolates showing high resistance to ciprofloxacin
DNA sequencing of the PCR amplified region of the gyrA and the parC genes from the ciprofloxacin susceptible isolates (UD1–UD5), revealed no alteration in either of the genes (table 2). However, multiple mutations were observed in the PCR amplified region of gyrA and the parC genes from the QRNG isolates (n = 58). All these isolates had mutation in the codon 91 of the gyrA leading to Ser-91 to Phe substitution. Single mutation, at position 91 of GyrA, was observed in only one isolate, exhibiting intermediate resistance towards ciprofloxacin with an MIC of 0.1 μg/ml (table 2). All other QRNG isolates (n = 57) had atleast two mutations in the gyrA gene along with parC mutation(s). The most frequent mutations (in 81% of QRNG isolates) are the Ser-91 to Phe and Asp-95 to Asn substitutions in the GyrA protein. Among the 12 isolates with MIC for ciprofloxacin of 32 μg/ml, 10 isolates (UD52 to UD61) had an Asp-95 to Gly substitution along with the Ser-91 to Phe in the gyrA gene. The other two isolates, UD62 and UD63, had three point mutations in the gyrA gene resulting in three amino acid substitutions (Ser-91 to Phe, Asp-95 to Asn, and Val-120 to Leu) in the GyrA (table 2). Interestingly this third mutation (Val-120 to Leu) lies outside the so far recognised QRDR (amino acids 55 to 110 of N gonorrhoeae GyrA protein).15 WHO strain A, which is sensitive to ciprofloxacin (MIC of 0.016 μg/ml), had no mutation in the gyrA gene while WHO strain H (MIC of 2.0 μg/ml for ciprofloxacin) and WHO strain J (MIC of 8 μg/ml for ciprofloxacin), had two mutations leading to Ser-91 to Phe and Asp-95 to Gly substitutions.
Mutation patterns in the GyrA and ParC proteins of Neisseria gonorrhoeae isolates
Sequence analysis of the parC gene demonstrated a variety of mutations at codons 91, 100, 104, 109, and 131 (table 2). The isolates (UD7–UD28), exhibiting intermediate resistance to ciprofloxacin (MIC from 0.06–0.75 μg/ml), had only silent mutations at the parC locus. The most common substitution of Glu-91 to Gly in the parC gene was found in 33 QRNG isolates (57%). The two isolates (UD62, UD63), having a novel mutation in the gyrA gene, also possessed a hitherto undescribed mutation at the parC, resulting in the substitution of Phe-100 with Tyr. Along with this mutation, two silent mutations at codon 104 (Tyr) and 109 (Gly) were also observed in the parC gene of these two isolates. The silent mutation at the codon 109 has also not been described before. WHO strain A (MIC of 0.016 μg/ml) had no mutation in the parC gene while WHO Strain H (MIC of 2.0 μg/ml for ciprofloxacin) and WHO strain J (MIC of 8 μg/ml for ciprofloxacin) possessed a single mutation at the codon 88 (Ser-88 to Pro) and 86 (Asp-86 to Asn) respectively.
DISCUSSION
During the past few years, an overall increase in resistance to various antimicrobial agents have been observed in N gonorrhoeae.6,10,23,24 Despite a high prevalence of gonorrhoea in India, a systematic study regarding resistance to various antimicrobial agents is limited.7,10,23,25 In the present study, an increase in the number of QRNG isolates (92%) as well as the level of resistance to ciprofloxacin (MIC up to 32 μg/ml) was observed in N gonorrhoeae isolated from patients visiting STD Centre, Safdarjung Hospital, India. A significant proportion of high level QRNG (63%) has also been reported from Philippines.2 Almost 90% of isolates in China and Hong Kong were QRNG and about half of these isolates possessed high level of resistance.2 In Japan, although the overall percentage of resistant strains has not changed appreciably in past 2 years, there was a gradual increase in level of resistance (MIC >1.0 μg/ml).11 Decreased susceptibility to ciprofloxacin and ofloxacin has also been reported from Bangladesh (11.7% were resistant and 26.6% had reduced susceptibility).9 This widespread emergence of ciprofloxacin resistance in South East Asia is rather alarming.
Mutations in the gyrA and the parC genes leading to amino acid changes in GyrA (especially at Ser-91 and Asp-95) and ParC proteins are significantly associated with ciprofloxacin resistance.5,11,15,17,18,26–28 Mutation at codon 91 of the gyrA gene results in the loss of natural Hinf1 site. Direct Hinf1 digestion of PCR amplified gyrA gene has been used to screen gyrA mutations in N gonorrhoeae.27,29 Another restriction endonuclease site (Alw1) spans the novel mutation (Val-120 to Leu), identified by us. Double digestion with Hinf1 and Alw1 would result in release of a fragment from the wild type but not mutated gyrA gene and may be used to check for mutations at these two loci.
Since QRNG isolates (intermediate and resistant) exhibit a wide range of MIC for ciprofloxacin (0.1–32 μg/ml), mutation pattern in gyrA and parC genes was checked in all the isolates. Double and triple mutations in the QRDR region of gyrA and the parC genes appear to be the major contributors to the high level of ciprofloxacin resistance. It is significant to note that the most common gyrA mutations (in 75% of the isolates) found by us were Ser-91 to Phe and Asp-95 to Asn, while only 16% isolates showed change of Asp-95 to Gly along with Ser-91 to Phe. None of the isolates sequenced in this study had tyrosine at position 91 in the gyrA gene.11,12,28 We also did not observe any isolate carrying mutation at Ala-67, Ala-75, and Ala-84 in the gyrA, as reported in some of the isolates from Japan.11 Isolates (UD7-UD28), with low MIC for ciprofloxacin (0.25–0.75 μg/ml), had silent mutations at the parC locus, while all other isolates (MIC of 1–32 μg/ml), except UD62 and UD63, had Glu-91 to Gly substitution. This supports the earlier observations that mutations in parC have a complementary role in decreasing susceptibility to ciprofloxacin.11,15,17,18,26,27 Alterations at the Gly-85, Asp-86, Ser-87, Ser-88, or Arg 116 residues, in parC, as reported in the earlier studies,11,17,27 have not been found in any of the clinical isolates in the present study. Instead, two isolates (UD62 and UD63) with high MIC for ciprofloxacin had a Phe-100 to Tyr substitution along with the triple mutations in the QRDR of the GyrA protein (Ser-91 to Phe, Asp-95 to Asn, and Val-120 to Leu). The third mutation observed in these two isolates has not been reported so far. Though close to QRDR in the GyrA subunit, this novel mutation is present downstream of the identified QRDR. Additional mutations in the gyrA gene, about 20–30 amino acids away from Ser-83 in Escherichia coli and Thr-83 in Pseudomonas aeruginosa, leading to quinolone resistance, have also been reported in E coli (Gln-106 to Arg, Gln-106 to His) and P aeruginosa (Asn-116 to Tyr) respectively.30,31 Acknowledging that transformation studies need to be performed for confirmation, these results suggest that triple mutations in gyrA along with the Phe-100 to Tyr substitution in the parC may have some bearing on the action of ciprofloxacin in N gonorrhoeae.
The results of our study clearly indicate that resistance to ciprofloxacin, which was introduced as first line therapy only in 1990, has increased rapidly with an alarming high level of MIC values and new mutational patterns in N gonorrhoeae. Unless continued monitoring of antimicrobial sensitivity patterns of gonococcal strains circulating in a community is carried out, treatment failures may occur and lead to prolonged infection and spread of multiple drug resistant strains of N gonorrhoeae.
Key messages
-
Emergence of ciprofloxacin resistant Neisseria gonorrhoeae
-
High percentage of isolates have high level of MIC for ciprofloxacin
-
Characterisation of novel mutations in the QRDR region of gyrA and parC genes of Neisseria gonorrhoeae
-
Rapid screening of ciprofloxacin resistant isolates by Hinf1 digestion of the gyrA amplified product.
Acknowledgments
We are grateful to the director, Centre for Biochemical Technology, for extending their facilities for DNA sequencing to us. We thank Ms Leelamma Peter for excellent technical assistance. One of us (UC) is grateful to CSIR for the award of senior research fellowship.
CONTRIBUTORS KR (head, STD laboratory) and MB collected the clinical samples and conducted the drug sensitivity for Neisseria gonorrhoeae; UC carried out PCR and analysis of mutations in the QRDR region of gyrA and parC genes; DS instigated the project, designed the study, and analysed the data; DS and UC wrote the manuscript.