Article Text

Abstract
Objective: To develop a scoring system for risk stratification and evaluation of the effect of an early invasive strategy for treatment of unstable coronary artery disease (CAD).
Design: Retrospective analysis of a randomised study (FRISC II; fast revascularisation in instability in coronary disease).
Setting: 58 Scandinavian hospitals.
Patients: 2457 patients with unstable CAD from the FRISC II study.
Main outcome measures: One year rates of mortality and death/myocardial infarction (MI).
Methods: Patients were randomly assigned to an early invasive or a non-invasive strategy. From the non-invasive cohort independent variables of death or death/MI were identified.
Results: Seven factors, age > 70 years, male sex, diabetes, previous MI, ST depression, and increased concentrations of troponins and markers of inflammation (interleukin 6 or C reactive protein), were associated with an independent increased risk for death or death/MI. In patients with ⩾ 5 of these factors the invasive strategy reduced mortality from 15.4% (20 of 130) to 5.2% (7 of 134) (risk ratio (RR) 0.34, 95% confidence interval (CI) 0.15 to 0.78, p = 0.006). Death/MI was also reduced in patients with 3–4 factors from 15.7% (80 of 511) to 10.8% (58 of 538) (RR 0.69, 95% CI 0.50 to 0.94, p = 0.02). Neither death nor death/MI was reduced in patients with 0–2 risk factors.
Conclusion: In unstable CAD, this scoring system based on factors independently associated with an adverse outcome can be used shortly after admission to the hospital for risk stratification and for selection of patients to an early invasive treatment strategy.
- CAD, coronary artery disease
- CRP, C reactive protein
- FRISC, fast revascularisation in instability in coronary disease
- MI, myocardial infarction
- RITA, randomised intervention trial of unstable angina
- TACTICS, treat angina with Aggrastat and determine cost of therapy with an invasive or conservative strategy
- TIMI, thrombolysis in myocardial infarction
- unstable angina
- myocardial infarction
- randomised study
- revascularisation
- risk stratification
Statistics from Altmetric.com
- CAD, coronary artery disease
- CRP, C reactive protein
- FRISC, fast revascularisation in instability in coronary disease
- MI, myocardial infarction
- RITA, randomised intervention trial of unstable angina
- TACTICS, treat angina with Aggrastat and determine cost of therapy with an invasive or conservative strategy
- TIMI, thrombolysis in myocardial infarction
Unstable coronary artery disease (CAD)—unstable angina or non-ST elevation myocardial infarction (MI)—can be treated with an early invasive or a primarily non-invasive regimen. In the FRISC (fast revascularisation in instability in coronary disease) II, TACTICS (treat angina with Aggrastat and determine cost of therapy with an invasive or conservative strategy), and RITA (randomised intervention trial of unstable angina) III trials primary end point rates were reduced by the early invasive strategy.1–4 Subsequently, treatment recommendations have been changed and revascularisation procedures have increased substantially. However, not all patients with an episode of unstable CAD will benefit from this treatment, which is both expensive and associated with an inherent procedural risk. Thus, a means for selecting patients is needed. Several univariable risk indicators5,6,7,8,9,10,11,12 and multivariable risk scores have been used for risk stratification.13–16 However, a score focusing on treatment effect would be even more helpful in a clinical setting.17,18 The objective of this study was to develop a scoring system (the FRISC score) consisting of clinically relevant and accessible factors that may be used to select patients for an early invasive strategy.
METHODS
Patients
In the FRISC II trial 2457 patients were randomly assigned to an invasive or a non-invasive regimen.1 Patients with unstable angina or non-ST elevation MI were eligible for the trial. Inclusion criteria were increasing or rest symptoms of cardiac ischaemia associated with either ST depression ⩾ 0.1 mV or T wave inversion ⩾ 0.1 mV in at least one lead or increased biochemical marker of myocardial damage.
The study complied with the Declaration of Helsinki and all local ethics committees approved the protocol.
Randomised treatment
The patients gave informed, written consent and were randomly assigned to an early invasive or early non-invasive strategy and to short or long term treatment with dalteparin. In the early invasive group coronary angiography and if appropriate revascularisation was to be performed within seven days. Revascularisation was recommended for all patients with a ⩾ 70% diameter obstruction in any artery supplying a significant proportion of the myocardium. In the non-invasive group coronary angiography or revascularisation was recommended in case of recurrent angina and severe ischaemia during a pre-discharge exercise test or with (new) MI.
All patients received open label dalteparin for at least five days and always until a scheduled revascularisation procedure. Thereafter, the patients continued long term treatment with dalteparin or placebo. As long term dalteparin treatment had no significant effect on 12 months’ outcome, the dalteparin and placebo groups have been combined in the present report.
Data collection
Blood samples and biochemical analyses
At randomisation blood was collected in tubes containing EDTA or citrate and centrifuged at each site. The plasma was frozen in aliquots and stored at −70°C until the analysis. Troponin T, troponin I, C reactive protein (CRP), fibrinogen, and interleukin 6 were measured at the department of clinical chemistry, Uppsala University, without knowledge of the patients’ randomisation or clinical outcome. The total cholesterol concentration was analysed at the local hospital laboratory.
Electrocardiography
Twelve lead ECGs were obtained on admission and evaluated at a core laboratory, without knowledge of the patients’ randomisation and clinical outcome. ST depression was considered present if the ST segment was horizontal or downsloping and at least 0.05 mV below the isoelectric level.6
Coronary angiography
All coronary angiograms recorded within six months were evaluated locally and recorded in accordance with the American Heart Association committee report on CAD from 1975.19 Stenoses ⩾ 50% were considered significant. Also, the occurrences of visible thrombus and TIMI (thrombolysis in myocardial infarction) flow were evaluated.
Follow up and outcome events
Patients were followed by outpatient visits for six months. The 12 month follow up was performed by telephone interview and, if appropriate, by evaluation of the patients’ hospital record.
MI has been defined previously and was based on the presence of two of the conventional three criteria: typical chest pain, diagnostic ECG, or increased biochemical markers of myocardial damage twice the upper limit of normal.1 Only new Q waves were used for the diagnosis of MI in association with coronary artery bypass grafting. For percutaneous coronary interventions the biochemical criterion was three times the upper limit of normal.
Baseline characteristics
On the basis of previous experiences with risk stratification in stable and unstable CAD, variables at baseline that can predict a worse prognosis were selected (table 1). All variables were dichotomised. In this study patients older than 70 years had a higher incidence of death/MI, whereas in the group between 65–70 years end point rates were similar to those below 65 years (data not shown). Therefore, for age, 70 years was chosen as the cut off level. For body mass index, cholesterol, and fibrinogen no clear cut off level could be identified and the median level was chosen as the cut off. Troponin T concentration, which was available for 95% of the population, or troponin I, for patients without available troponin T, was used to define the occurrence of increased concentration of biochemical marker of myocardial damage. In previous reports from FRISC II, troponin T ⩾ 0.03 µg/l9 or troponin I ⩾ 0.03 µg/l20 identified patients with increased risk, which therefore were used as cut offs. Increased inflammatory activity was based on the interleukin 6 concentration or, if this was not available, the CRP concentration. Based on previous experiences, 5 ng/l and 10 mg/l were chosen as cut off concentrations for interleukin 6 and CRP, respectively.10–12 Interleukin 6 was most efficient for identifying patients with a large benefit from early revascularisation.12 However, this biochemical analysis has not yet reached clinical practice. In this study we therefore combined interleukin 6 and CRP into one variable with two alternatives.
Mortality in relation to risk variables by univariable and multivariable analyses* in the non-invasive cohort
Statistical analysis
Univariable associations between the risk indicators and outcome were evaluated by Pearson χ2 test. Variables achieving a significance level < 0.05 were inserted in a forward stepwise logistic regression model and those independently (p < 0.05) associated with either the rate of death or death/MI were included as components of the FRISC score.
Each factor was given one point regardless of the magnitude of the odds ratio or whether the factor was present as an independent risk for both death and death/MI. Only patients with available data on all the factors in the FRISC score were included in the analyses. Information on vital status at 12 months was available for all of these patients but for three patients in the invasive group, information on MI could not be obtained.
The association between the FRISC score strata and outcome was assessed by χ2 test for trend (Mantel-Haenszel trend test).
We used the Hosmer-Lemeshow test to assess the goodness of fit of the logistic regression models. The predictive value of the FRISC score was evaluated with the C statistic—that is, the area under the receiver operating characteristic curve. All statistical analyses were performed with the SPSS 10.1 statistical program (SPSS Inc, Chicago, Illinois, USA).
RESULTS
Prognostic variables in the non-invasive group
In the non-invasive cohort (n = 1235) one year mortality was 3.9% (n = 48) and the rate of death/MI 14.1% (n = 174). In the univariable analyses, seven and eight variables were associated with an increased risk for mortality and death/MI, respectively, and were selected for the multivariable analyses. Age ⩾ 70 years, male sex, diabetes, previous MI, ST segment depression on admission, and increased concentrations of markers of myocardial damage and inflammation were independently related to mortality or the composite of death and MI. Thus, these seven variables were included in the final FRISC score model. Among these variables diabetes was the strongest independent predictor both for death and for death/MI. Increased inflammatory activity was, after diabetes, the second strongest predictor for mortality (tables 1 and 2).
Death or MI in relation to risk variables, univariable and multivariable analyses* in the non-invasive cohort
The C statistics for the relation between the FRISC score and outcome were 0.77 for mortality and 0.70 for death/MI. Concerning different age cut offs, there were only small effects on the C statistics, ranging from 0.77–0.79 for mortality and 0.68–0.70 for death/MI when age cut offs varied in five year intervals from 60–80 years. Also, when age was used as a continuous variable the C statistics were 0.79 for mortality and 0.70 for death/MI. As interleukin 6 is not yet easily available in clinical practice at many hospitals, we have also analysed the material for only CRP and disregarding interleukin 6 concentrations. The results are similar with a small decrease in C index to 0.76 for mortality and to 0.68 for the combined end point.
FRISC score in relation to prognosis in the non-invasive group
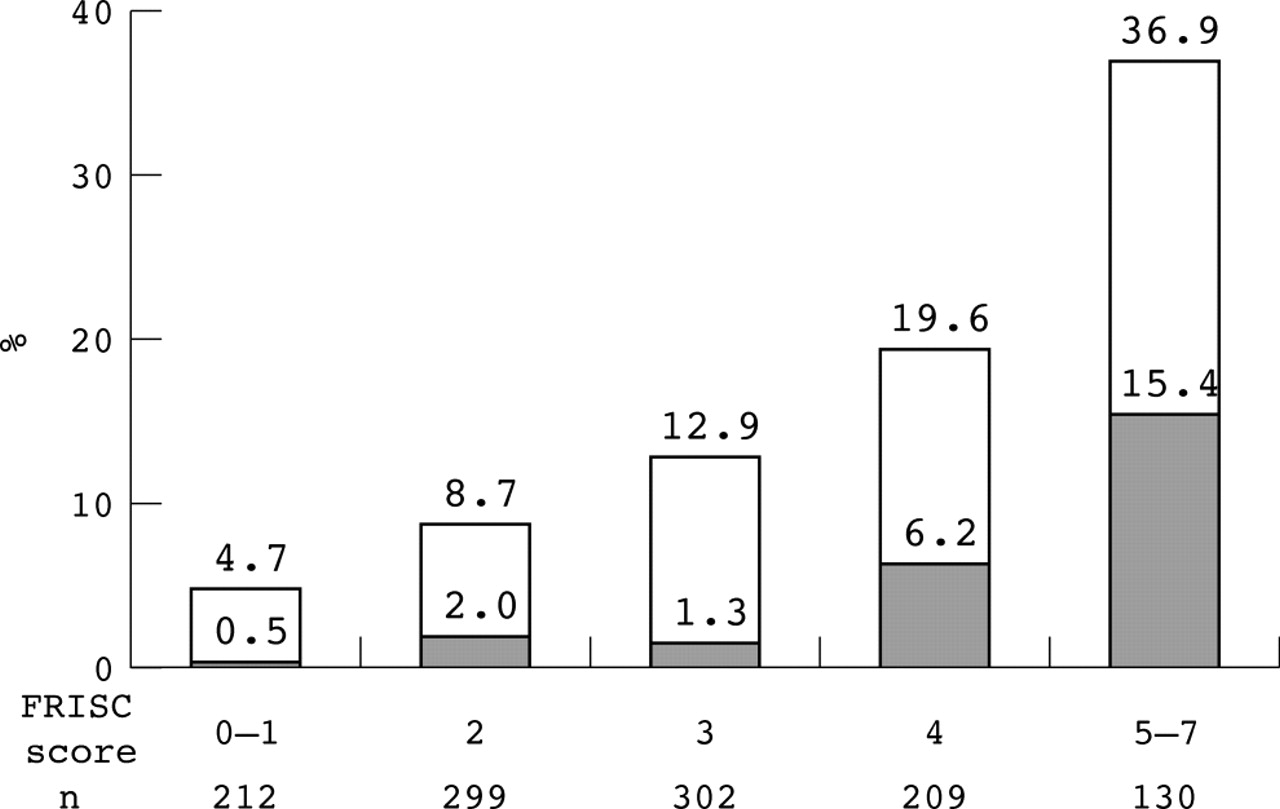
To obtain strata with adequate numbers of patients, groups with no or one risk variable and with ⩾ 5 risk variables were merged. There was a relation between the number of risk variables and the occurrence of death and the combination of death and MI (p < 0.001 for both). In the group with the highest FRISC score (⩾ 5) one year mortality was 15.4% (20 of 130) and the rate of death/MI was 36.9% (48 of 130). The corresponding numbers for the group with the lowest FRISC score (0–1) were 0.5% (one of 212) and 4.7% (10 of 212), respectively (fig 1).

One year death (grey bars) and the composite of death and myocardial infarction (grey + white bars) in relation to FRISC score in the non-invasive cohort. By Mantel-Haenszel trend test, p < 0.001 for both death and death/myocardial infarction.
FRISC score in relation to angiographic findings in the invasive group
In the invasive cohort coronary angiography was performed in 98% (1200 of 1222) of the patients (96%, 1176 of 1222, within seven days). Three vessel or left main disease occurred in more than 60% (80 of 129) of the patients with FRISC score 5–7 and in 11% (20 of 179) of patients with FRISC score 0–1 (fig 2). Also, the proportion of patients with TIMI III flow in all major vessels was related to the FRISC score (fig 3). However, no correlation with the occurrence of angiographically visible thrombus was observed.
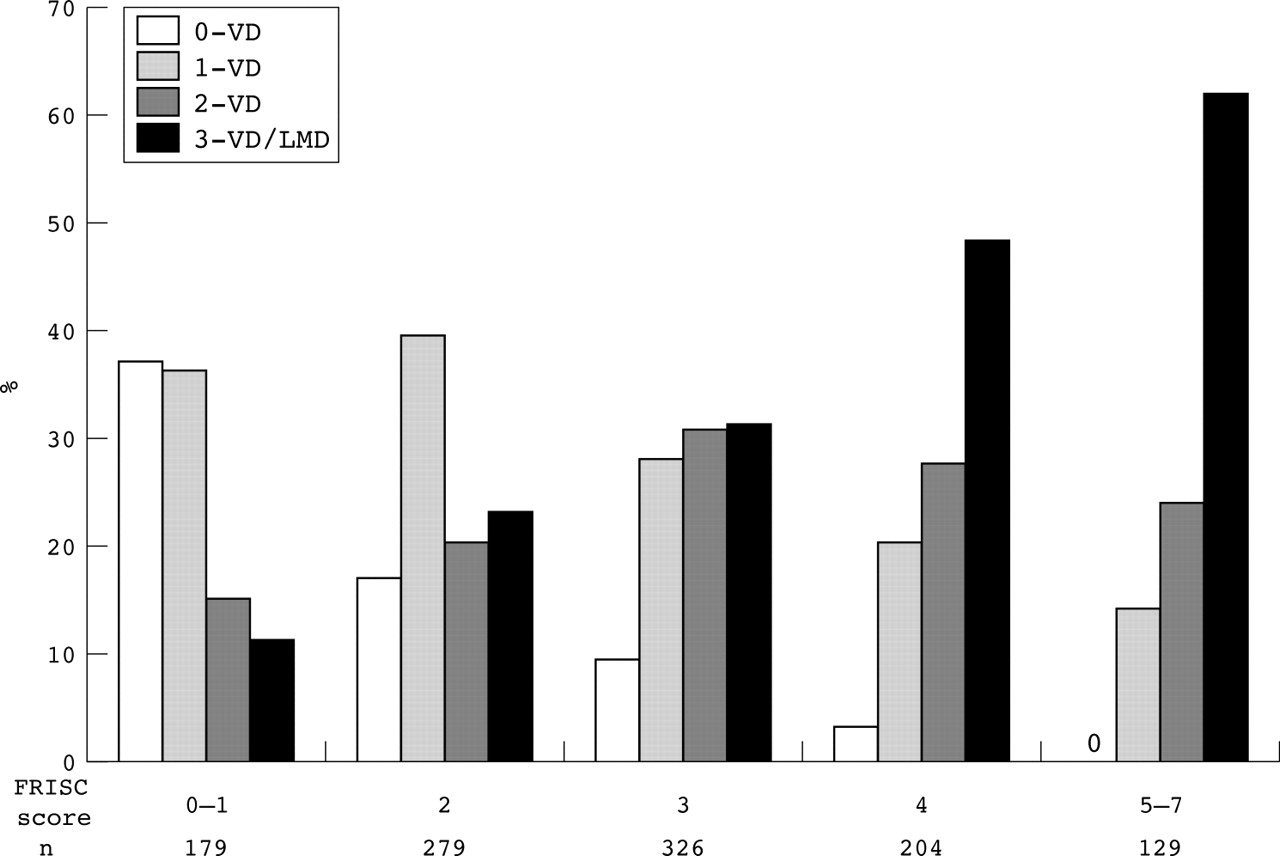
Distribution of severity of coronary artery disease at angiography in relation to FRISC score in the invasive cohort. 0 vessel disease (VD) = no significant stenosis. LMD, left main disease.

Number of patients with TIMI III flow in all major vessels in relation to FRISC score in the invasive cohort. By Mantel-Haenszel trend test, p < 0.001.
FRISC score in relation to effect of the invasive strategy
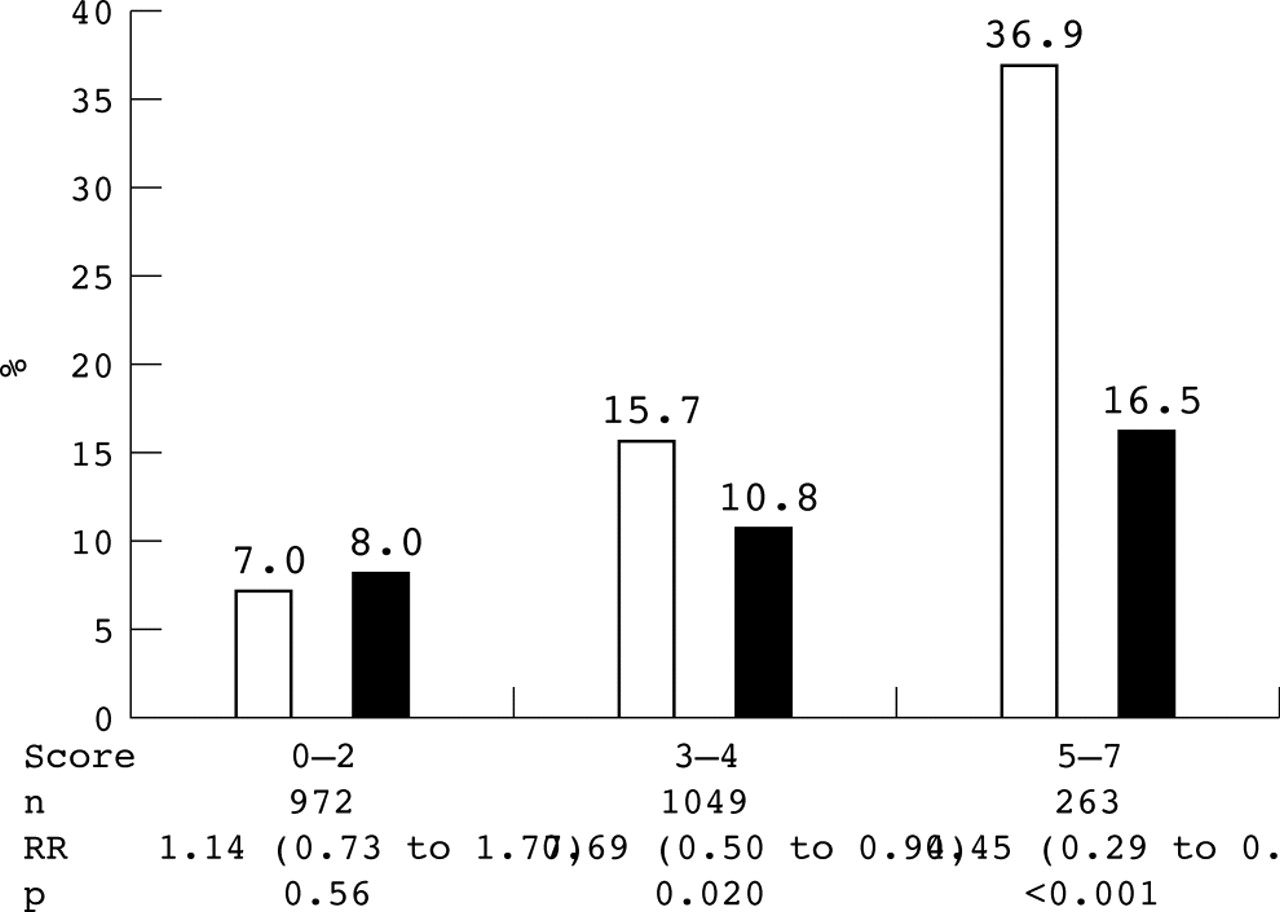
To evaluate the treatment effect the patients were categorised into low, intermediate, or high risk based on the FRISC scores 0–2, 3–4, or 5–7. In the high risk group, which constituted 12% (264 of 2287) of the population, the invasive strategy reduced mortality from 15.4% (20 of 130) to 5.2% (seven of 134) (fig 4). The composite of death and MI was reduced in the intermediate and high risk groups, whereas in the low risk group no significant reduction was observed (fig 5).

One year mortality in relation to treatment strategy and the FRISC score. White bars, non-invasive strategy; black bars, invasive strategy. Risk ratios (RR), confidence intervals, and p values refer to the comparison between the invasive and non-invasive strategies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
One year death or myocardial infarction in relation to treatment strategy and the FRISC score.
DISCUSSION
In patients with unstable CAD the prognosis varies considerably depending on the clinical presentation. ST segment depression on the ECG and increased concentrations of biochemical markers of myocardial damage and inflammation are associated with a worse prognosis.5–9,11,12 Also, other factors such as increased age, hypertension, diabetes, and previous MI indicate a higher risk of future events.21,22 Although most studies have adjusted for other factors by multivariable analyses, the main analyses have focused on just one of these factors. However, in a clinical setting, more comprehensive risk stratification is needed and more than one factor has to be considered. In the TIMI risk score seven clinical parameters were identified for risk stratification in unstable CAD on the triple end point death, MI, or urgent revascularisation.17 On the basis of the FRISC II study, in which the early invasive approach reduced both death and death/MI, we now present an alternative scoring system that may be used both for risk stratification and for selection of patients who would benefit most from early revascularisation.
Is there a need for a risk score?
Owing to the large number of and complex relation between risk factors it seems rational to produce a scoring system that, compared with a single risk indicator, further modulates the risk. Various scoring systems have been constructed for unstable CAD .13–18 However, the variables used in these studies vary considerably. A major problem when constructing a risk score is which parameters to choose and their relative importance. A risk score should be simple, contain readily available parameters, and preferably also identify patients who would benefit from a certain treatment.
Choice of variables in the risk score
When constructing a scoring system for risk stratification it seems logical to identify variables independently associated with outcome. In this study seven variables remained as independent predictors for death or death/MI and were included in the final model. A far more complex issue is how to construct a scoring system for evaluation of treatment effect, which was the primary objective. In this study we also used the multivariable risk evaluation to identify patients with the most beneficial treatment effect. Thus, we assumed that patients with the highest risk also had the largest reduction of events by the invasive strategy. In the univariable analyses of treatment effect this was confirmed (data not shown). Furthermore, the finding of a relation between the FRISC score and the occurrence of three vessel or left main disease in this study supports the correlation between subsequent risk and effect of invasive procedures, which are especially efficient if this angiographic finding is present.23
For six of the variables, there was a strong correlation with end point rates in the multivariable analyses (p < 0.001 to p = 0.007). The significance was lower only for male sex (p = 0.049). However, the selection of this variable is also justified because of the interaction observed between sex and the effect of the early invasive strategy in both the FRISC II and RITA III studies, with a far more beneficial effect observed in the male population.4,24
The FRISC score appears to be well balanced with two demographic factors indicating the likelihood of CAD (age, sex), the major metabolic risk factor (diabetes), one factor indicating established CAD or reduced left ventricular function (previous MI), and three factors associated with the acute event: ischaemia (ST depression), myocardial damage or coronary thrombosis (troponins), and inflammation (interleukin 6 or CRP).
Evaluation of prognosis and effect of the invasive strategy
With this method a scoring system was developed in which the presence of an additional factor implied a higher risk. However, these retrospective findings need to be tested in prospective studies. More important, though, was that the FRISC score also could identify patients in whom early revascularisation was especially effective. The reduction in one year mortality was observed mainly in the high risk population—that is, patients with five or more factors from the FRISC score. In these patients 10 lives and 10 non-fatal MI were saved for every 100 treated, a remarkably high number. Although only about 12% of the FRISC II population was considered to have high risk it is of vital importance to identify these patients. However, the reduction of the composite of death and MI was also seen in the large intermediate risk group. In contrast, there seemed to be no gain in the low risk population, where end point rates were low. Also, in the TACTICS trial, which as end point also included rehospitalisation for an acute coronary syndrome, the most beneficial effect was seen in those who, based on the TIMI score, were regarded as medium and high risk patients.3 In the TIMI IIIB trial, which used another risk score, death/MI was reduced in the high and very high risk patients, although the overall study did not reach significance.25
Study limitations
The FRISC study selected only patients with objective signs of myocardial ischaemia, thus mostly patients with medium and high risk. This study may not be fully applicable to low risk patients. In the majority of the patients of the present study the interleukin 6 concentration was used to indicate inflammatory activity. However, CRP determination is more generally available, which is a limitation of the study.
In the proposed score only factors present on admission are included. However, during the hospital stay other risk factors, such as the occurrence of ischaemic episodes with continuous ECG monitoring26 or the results of an exercise test, may modify the initial judgement.27
This risk score is based on a retrospective analysis of a previous study and should be confirmed in a prospective study. Furthermore, the study was confined to Scandinavian patients and few had prior revascularisation.
Conclusions
In unstable CAD, the FRISC score, based on the seven factors age ⩾ 70 years, male sex, diabetes, previous MI, ST depression on admission, and increased concentrations of troponins and interleukin 6 or CRP, is readily available and highly useful both for risk stratification and for selection of patients for an early invasive strategy. For patients with three or more of these factors an early invasive strategy is recommended, whereas for those with 0–2 factors event rates are low regardless of strategy.
Acknowledgments
We gratefully acknowledge biostatisticians Johan Lindbäck and Niclas Eriksson at Uppsala Clinical Research Centre for their statistical advice.
REFERENCES
Footnotes
-
Sources of support: The Pharmacia & Upjohn Company and the Swedish Heart-Lung Foundation.