Article Text

Abstract
Ischaemic heart disease (IHD), previously considered rare in sub-Saharan Africa, now ranks 8th among the leading causes of death in men and women in the region. Furthermore, the prevalence of IHD and related morbidity may be increasing as a result of adverse behavioural and lifestyle changes associated with urbanisation and the epidemiological transition. The major risk factors for IHD in sub-Saharan Africa include hypertension, smoking, diabetes, abdominal obesity and dyslipidaemia. In the INTERHEART Africa study, these risk factors contributed a population-attributable risk of nearly 90% for acute myocardial infarction. Many cost-effective interventions exist at the individual and population levels, and they are likely to have a significant health impact in Africa. An aggressive approach that combines environmental, policy and legislative interventions for health promotion and primary prevention, coupled with improved access to evaluation, treatment and control of hypertension and other major risk factors, provides the best strategy for averting an epidemic of IHD in sub-Saharan Africa.
Statistics from Altmetric.com
Ischaemic heart disease (IHD), the principal component of cardiovascular diseases (CVD), is the leading cause of death in all regions of the World Health Organization (WHO) except the African region.1 At the turn of the 21st century however, IHD ranked eighth among the leading killers in the region, just behind cerebrovascular diseases in both men and women.2 3 The WHO estimated that in 2005, IHD caused approximately 361 000 deaths in the African region, and current projections suggest that this number will nearly double by 2030.4 Importantly, in people aged ⩾60 years, IHD is already the leading cause of death in men and the second leading cause of death in women in the African region. Considering that IHD was regarded as rare in sub-Saharan Africa barely 50 years ago, these observations are remarkable and highlight the emerging burden of chronic non-communicable diseases that is now superimposed on the huge burden of HIV/AIDS, other infectious and parasitic diseases, and the ravages of famine, malnutrition, and social conflict that constitute Africa’s health challenges today.
In this review, the historical evidence of the rarity of IHD in Africa in the past century is presented, and the factors that have given rise to the increase in the IHD burden are discussed. The current estimates of IHD burden and projections to 2015 and 2030 are also reviewed. The epidemiology of the major risk factors for atherosclerosis that fuel the increase in the IHD burden, including high blood pressure, tobacco use, obesity, diabetes mellitus, and dyslipidaemia, are presented and their contribution to the population risk of IHD discussed. Current national and international strategies for preventing and controlling IHD are reviewed. An aggressive approach that combines policy and environmental change with a focus on primordial and primary prevention of IHD is proposed as the best strategy for averting an epidemic of IHD in sub-Saharan Africa.
HISTORICAL PERSPECTIVES
There are ample data from Western, Eastern, Central, and Southern Africa suggesting that coronary heart disease was rare up until the mid-20th century.5–10 In their extensive reviews of data on the evolution of CVD in Ghana (then the Gold Coast), Pobee11 and Biritwum et al5 noted that the Annual Medical and Sanitary Reports (AMSR) sent regularly to the Colonial Secretary in London by the Gold Coast government showed that coronary heart disease was distinctly rare from 1898 to 1960. During that same period, however, the AMSR increasingly mentioned rheumatic fever, rheumatic heart disease, congenital heart disease, valvular disease, myocarditis, endocarditis and apoplexy or stroke, and they also noted an increasing prevalence of rheumatic heart disease and stroke beginning in the 1930s.5 The AMSR from Nigeria during this period mentioned a similar spectrum of CVD but did not mention any coronary heart disease.6 Subsequent studies, mostly hospital based, showed the continuing rarity of coronary heart disease in Nigeria.12 In a 10-year period (1961–70), Falase et al identified only 26 patients who had a myocardial infarction, yielding an incidence of 1 in 20 000 hospitalised adults in Nigeria.12 Nine of their patients had a coronary embolism rather than atherosclerotic coronary occlusion.
Coronary heart disease was also deemed rare in Uganda, as demonstrated in the analysis reported by Cooke7 just over a century ago and by Shaper and Shaper8 in 1958. Although CVD constituted 6–8% of medical admissions in both of these studies from Uganda, the major CVDs encountered were syphilitic heart disease, endomyocardial fibrosis, hypertension and rheumatic heart disease.7 8 In the 1940s in South Africa, Becker found only a single death from coronary heart disease in an autopsy study on a series of 352 adult Africans.9 Several other studies conducted up to three decades later in Johannesburg and Durban found coronary heart disease to be rare among blacks in South Africa, especially in rural areas.10
The general notion about IHD in Africa at the time, as expressed by Walker and Sareli,10 was that “as long as Africa remains impoverished, a major rise in CHD is unlikely”. Although Africa is still home to about three-quarters of the world’s poorest countries, and nearly half of the region’s population still lives in extreme poverty, the most recent indicators suggest that Africa is making economic progress.13 For example, annual economic growth for all of sub-Saharan Africa, which averaged only 2.4% in the 1990s, increased to 4.0% in 2004, and most recent estimates show a rate of 4.3% for 2005.13 Almost inevitably, however, with these economic improvements comes the epidemiological transition, which involves a rise in chronic diseases of lifestyle such as IHD.
THE EPIDEMIOLOGICAL TRANSITION IN AFRICA
The concept of an epidemiological transition, originally proposed by Omran14 and subsequently modified by other investigators,15 16 states that a transition occurs in the relative frequencies of major causes of death as human societies undergo industrialisation and economic development. Over time, the epidemiological transition results in a shift in the major causes of death and disability from infectious diseases and nutritional deficiencies early on to an eventual predominance of chronic degenerative diseases such as CVD and cancer.14–16 This epidemiological transition, which has now been well documented in most regions of the world, confirms the principle that the health status and disease profile of populations are linked to their level of economic development, industrialisation and globalisation. In sub-Saharan Africa, data for the existence of an orderly shift from one stage of the transition to the next are scanty; however, evidence of a changing disease profile with coexistence of infectious diseases, nutritional deficiencies and non-communicable chronic diseases is becoming more common.
Important lessons we have learnt include the observation that various countries and regions experience different stages of the transition at different times, and the speed with which they pass from one stage to the next varies widely. In fact, within a particular country, various subgroups may undergo this transition at different rates depending on the speed at which economic development and industrialisation occur and on the magnitude of changes in lifestyles and health behaviours. In general, the epidemiological transition is occurring in a more compressed time frame in sub-Saharan Africa and other developing countries than was the case in the developed countries of North America and Western Europe.17 18 The implications of the transition for promoting health and preventing disease in Africa and most developing countries are substantial and essentially call for renewed emphasis on population-based approaches to health promotion and primary prevention.
Table 1 shows that the proportion of total deaths attributable to CVD is relatively low (5–10%) in the first stage of the transition (“the age of pestilence and famine”).14–16 As infectious diseases are controlled in the second stage (“the age of receding pandemics”), however, the proportion of deaths attributable to CVD more than doubles (to 10–35%).14–16 It should be emphasised, however, that this is not simply the result of proportional changes in mortality (the decrease in the proportion of deaths from infectious diseases means that the proportion of deaths from non-infectious diseases must increase); it also reflects an increase in CVD deaths because risk factors created by adverse lifestyle choices and behaviours are more prevalent.19 For example, in the second stage of the epidemiological transition, the prevalence of high blood pressure and associated complications of haemorrhagic stroke and hypertensive heart disease increases, a phenomenon now being seen more frequently in some urban and semi-urban areas in sub-Saharan Africa.18 20 21
Sub-Saharan Africa, like many rural parts of India and South America, is predominantly in the earliest stage of the epidemiological transition. Thus, IHD is not yet a major burden even though it is no longer rare. Data from many urban areas in sub-Saharan Africa suggest a pattern of adverse lifestyle choices and health behaviours that are now leading to a rising prevalence of the major coronary risk factors. A careful assessment of the burden of risk factors, their pattern of distribution, and their social and environmental determinants will be crucial in efforts designed to prevent an epidemic of IHD in this region.
SPECTRUM OF IHD RISK FACTORS IN AFRICA
In their review of the emerging epidemic of CVD in developing countries, Reddy and Yusuf22 pointed out that a better understanding of the epidemiology of the principal coronary risk factors in these countries “will permit the development of more effective public health interventions to forestall future epidemics of coronary atherosclerosis”. Although the principal coronary risk factors in Africa are similar to those identified in other regions of the world, definitive data from Africa on the magnitude of the burden of risk factor, the strength of the associations between the various risk factors, and the incidence of myocardial infarction have generally been lacking.
Risk factors for IHD were directly examined in the INTERHEART Africa study, an international, standardised, case–control study that recruited 578 cases of first-time myocardial infarction and 785 controls from nine sub-Saharan African countries.23 The participants, almost 75% of them men, included 36.3% black Africans, 46.7% coloured Africans, and 17% European and other African people.23 As expected, and as also observed in the main INTERHEART study,24 age and sex were important variables, and men presented with first-time myocardial infarction at an earlier age than women. The mean (SD) age at presentation with a first-time myocardial infarction in the INTERHEART Africa cases (54.3 (11.3) years), however, was significantly younger (by 3.8 years) than in the overall INTERHEART study cases.24
The degree of the association of the major risk factors in the INTERHEART Africa study sample with first-time myocardial infarction was consistent with that observed for the global INTERHEART study. There were no differences between the overall INTERHEART participants and those from Africa when the impact of having three and four risk factors was assessed. Yusuf et al24 had shown earlier that nine risk factors (current/former smoker, diabetes, hypertension, increased ratio of apolipoprotein B (ApoB) to apolipoprotein A-1 (ApoA-1), increased waist-to-hip ratio, irregular intake of fruits and vegetables, no alcohol intake, physical inactivity and psychosocial stress) provided a population-attributable risk (PAR) of 97.4% for the African participants, as a group, in the INTERHEART study.24 The INTERHEART Africa study, however, showed that only five modifiable risk factors (current/former tobacco smoking, self-reported diabetes and hypertension, abdominal obesity measured as waist-to-hip ratio, and elevated ApoB/ApoA-1 ratio) contributed 89.2% of the risk for a first-time myocardial infarction.23 Table 2 presents the prevalence of the five major modifiable risk factors in cases and controls and their associated adjusted odds ratio and PAR in the overall INTERHEART study, the overall African population in that study, and the three African ethnic groups studied in the INTERHEART Africa study.23
Hypertension and diabetes stand out as particularly important in the black African population because of their higher PAR than that observed in the two other ethnic groups or in the overall global INTERHEART study.23 Although the PARs of current/former cigarette smoking, abdominal obesity, and increased ApoB/ApoA-1 are lower in the black African population than in the two other ethnic groups, the corresponding PARs for the overall African population exceed those calculated in the global INTERHEART study.
The INTERHEART Africa study also demonstrated that within the African population, the three ethnic groups studied (black, coloured, and European/other African) are at different stages of the epidemiological transition with regard to the IHD burden and associations with risk factors. Black Africans in the highest tertile for income had a higher risk of first-time myocardial infarction than those in the lowest income tertile (odds ratio = 2.75; 95% confidence interval 1.53 to 4.94; not shown in table 2).23 The direction of the association of income level and risk of myocardial infarction was reversed in Europeans/other Africans, while no differences in risk were noted by income level in coloured Africans. This same pattern was seen for the association of risk with educational attainment in all three ethnic groups.23 These observations are not surprising when viewed within the context of the epidemiological transition that has accompanied the social, economic and nutritional transitions in these countries.13
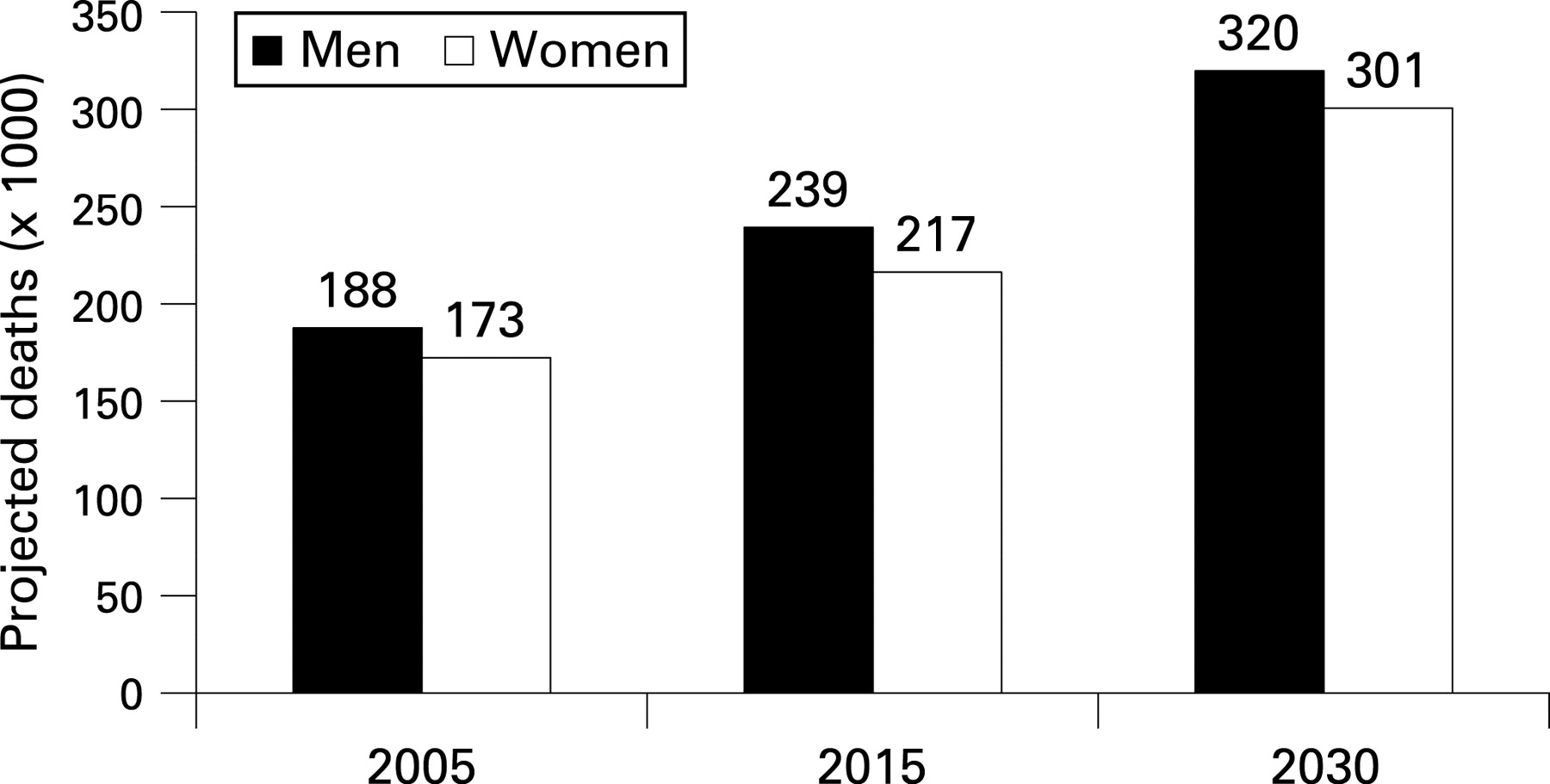
A measure of the current burden of IHD in the African region is shown by the age-standardised mortality rate from total CVD and the number of deaths and age-standardised mortality rates from IHD in men and women (table 3). In general, the mortality rates are higher in men than in women. According to an estimate from the Global Burden of Disease project, between 1996 and 2020, IHD deaths in sub-Saharan Africa will increase by 125% to 263 000 in men and by 141% to 222 000 in women.25 Figure 1 shows that the revised projections (in 2006) by the WHO are 188 000 in men and 173 000 in women in 2005, approximately 239 000 and 217 000 in men and women, respectively, in 2015, with a further increase to 320 000 and 301 000 in men and women, respectively in 2030.4

Even after incorporating a more realistic estimate for the spread of HIV/AIDS than was seen in earlier estimates, more recent projections of mortality and burden of disease suggest that by 2030, IHD will become the leading cause of death in low-income countries, contributing 13.4% of total deaths, versus 13.2% from HIV/AIDS. In addition, IHD is projected to rank fifth among the 10 leading causes of disability-adjusted life years (DALYs) in low-income countries by 2030.40 Table 4 illustrates the attributable mortality, years of life lost because of premature mortality, DALYs, and population-attributable fractions (PAFs) for IHD in sub-Saharan Africa by risk factor, age, and sex.
Taken together with reports of the increasing prevalence of major coronary risk factors in sub-Saharan Africa,5 23 27–29 these landmark findings from the INTERHEART and INTERHEART Africa studies argue for urgent attention to the prevention and control of risk factors and their social and environmental determinants in sub-Saharan Africa. While urban centres and their adjacent peri-urban areas pose the greatest current burden, there are data, especially from South Africa, suggesting that rural areas are also undergoing change and thus deserve attention.28 Strategies that combine environmental, policy and legislative actions for individual- and population-level prevention and control of major risk factors have worked in other regions and are likely to be effective in Africa.
In particular, the prevention and control of high blood pressure, increased physical activity, and increased intake of fruits and vegetables will be crucial in Africa. Figure 2 shows that hypertension, physical inactivity, and low intake of fruits and vegetables accounted for population attributable fractions for ischaemic heart disease mortality of 43%, 20%, and 25%, respectively, in the Africa region, all above the PAF of 15% for high cholesterol.30

{kind=link}
{kind=link}
CURRENT BURDEN AND TRENDS IN ISCHAEMIC HEART DISEASE
A wide variety of studies from Burkina Faso, Ethiopia, Ghana, Kenya, Nigeria, South Africa, Uganda, Tanzania and Zaire suggest that the incidence and prevalence of CVD is increasing, especially in urban and peri-urban areas.27 31–40 For example, in the discussion accompanying the report of an autopsy study of coronary atherosclerosis and myocardial infarction in Ethiopia in 1989, Maru reviewed case reports published in the preceding two decades from Ethiopia, Ghana, Ivory Coast, Kenya, Nigeria, South Africa, Uganda and Zimbabwe and concluded that the burden of coronary heart disease was already on the rise.32
PREVENTION AND CONTROL OF ISCHAEMIC HEART DISEASE IN AFRICA
Fundamental approaches to the prevention and control of IHD are to (a) promote cardiovascular health beginning early in life in order to prevent the development of risk factors (health promotion and primordial prevention); (b) screen for, identify, treat and control modifiable risk factors in order to prevent first-time IHD (primary prevention); (c) treat acute IHD events promptly so as to reduce case fatality and prevent acute complications (acute care and treatments); and (d) apply effective interventions in people who survive first-time IHD events in order to prevent recurrent events and long-term complications (secondary prevention).41 42 These complementary approaches, which embody the population/mass approach (public health model) and the high-risk/individual approach (medical model), are consistent with a strategy of preventive medicine as originally proposed by Geoffrey Rose.43
Increasingly, it has become clear that successful strategies for preventing and controlling IHD must include both specific medical treatments for this disorder and the prevention and control of its major modifiable risk factors. In most industrialised countries in which declines in mortality from coronary heart disease have been carefully examined, reductions in major risk factors have contributed to the declines at about the same level as specific medical treatments and interventions for coronary heart disease.44–48 For example, Ford et al recently showed that about 44% of the decline in US deaths due to coronary heart disease from 1980 through 2000 was attributable to reductions in major risk factors and approximately 47% to evidence-based medical treatments.48
In sub-Saharan Africa, as in many other low-resource settings, the relative lack of access to safe and effective drugs and interventions for IHD and limited national budgets for public health and healthcare require an even greater emphasis on the prevention of risk factors as the cornerstone of strategies to prevent and control IHD. Additionally, increasing urbanisation and adverse behavioural and lifestyle changes call for greater emphasis on population-based approaches.49 50 Although education on healthier lifestyle choices, such as weight reduction, increased intake of fruits and vegetables, smoking cessation and greater physical activity is important as pointed out by Kadiri,50 imparting the skills and resources for effective application of the knowledge is even more crucial.51 52 Individual and population-based interventions and strategies with demonstrated evidence of effectiveness must be emphasised.
Capacity for the promotion of cardiovascular health must be built from the grass roots up and will require national, regional and global partnerships.53 54 Several examples of such capacity-building endeavours already exist, and opportunities to apply lessons learnt over the past decade and a half from the global effort to promote cardiovascular health and prevent CVD can be helpful in adapting best practices for intervening in sub-Saharan Africa. Several international treaties and strategies for dealing with tobacco use, physical inactivity, poor nutrition and the global prevention of CVD and other chronic diseases are now available as valuable resources for the promotion of cardiovascular health.55–61 In particular, the WHO Global Strategy on Diet, Physical Activity and Health,61 the WHO Framework Convention on Tobacco Control (FCTC),57 the accompanying resource on the implementation of the FCTC in the African region,62 and the priority interventions identified in the situational analysis of CVD in Africa provide outstanding guidance and serve as valuable resources upon which the promotion of cardiovascular health and efforts to prevent CVD in Africa can build.
Additionally, an integrated approach within a primary healthcare setting for the control of major risk factors and reduction of total cardiovascular risk will be necessary. The WHO’s CVD risk management package for low- and medium-resource settings is one example of an appropriate guide for sub-Saharan Africa.63 Although this package was designed primarily for the management of CVD risk in people with high blood pressure detected through opportunistic screening, it can be adapted for use with diabetes, tobacco use, obesity and dyslipidaemia.63 Several studies have shown that the use of relatively less expensive generic preparations of CVD drugs, especially in combination with thiazide diuretics and aspirin (when appropriate in patients with high to very high total cardiovascular risk), may be cost effective if society is willing to pay at least $88 per DALY gained).64
An important principle in decisions about medical treatments in these settings is to match the intervention to the level of total cardiovascular risk rather than arbitrarily to set partition values for various risk factors. For example, Gaziano et al have recently shown that strategies based on target levels for risk factors (such as high blood pressure) may be more expensive and less effective than treatment decisions based on a strategy that uses absolute risk of CVD.65 66 Similarly, the use of aspirin and β-blockers as secondary prevention for myocardial infarction survivors (who have a very high 10-year risk of CVD events) would be cost saving in sub-Saharan African settings, such as major urban centres, where there is access to hospitals.30 Gaziano et al have also shown that a secondary prevention intervention made up of a four-drug regimen of aspirin, a β-blocker, an angiotensin-converting enzyme inhibitor and a statin would be cost effective at a ratio of $350/DALY averted, using no secondary prevention as the base condition.67 A more detailed discussion of the cost effectiveness of interventions is presented elsewhere in this journal’s series of reviews on CVD in Africa. In addition, the 2002 World Health Report considers a wide range of strategies to reduce different risk factors, including high blood pressure, cigarette smoking and cholesterol, and it discusses the possible impact of those strategies on costs and effectiveness.68
LIMITATIONS IN MORTALITY DATA FOR IHD
The data on current IHD burden and future projections in sub-Saharan Africa presented in this review are approximations and often embrace substantial uncertainties, especially in the estimation of death by cause. For example, Lopez et al showed that the uncertainty in estimates of all-cause mortality ranged from around 1% in high-income countries to 15–20% in Sub-Saharan Africa, but the uncertainty was greater for specific causes such as IHD.69 For sub-Saharan Africa, the uncertainty in the estimates for IHD in 2001 was around ±30% (versus about 12% for high-income countries).26 This huge degree of uncertainty has been attributed to the meagre database on IHD as a specific cause of death in Africa and to the overall low coverage of vital registration. As the authors of the estimates correctly point out, the uncertainty range is narrower (±15%) for HIV/AIDS deaths in sub-Saharan Africa, reflecting the substantial data base that exists for estimates of these deaths.26 Improving surveillance for IHD morbidity and mortality in sub-Saharan Africa remains an important challenge for research and programme development.
CONCLUSIONS
Africa still faces many daunting challenges in infectious diseases, nutritional deficiencies, and perinatal morbidity and mortality that are often seen as more pressing and deserving of limited health resources than are chronic non-communicable diseases such as IHD. Regardless, the weight of available evidence suggests that IHD is on the rise as a result of adverse behavioural and lifestyle changes associated with a rapidly evolving epidemiological transition. Current projections for burden of disease suggest that IHD will become the leading cause of death in this region by 2030 unless preventive action is taken now. These data should spur into action government agencies, non-governmental organisations, health professionals, patients and their families, communities, schools, worksites, and other settings from multiple sectors at the national and international levels. Given the limited resources in all of the sub-Saharan African countries, it is important that a fine balance be struck between the competing health priorities posed by the unfinished agenda of communicable diseases, nutritional deficiencies and perinatal conditions on the one hand, and the rising prevalence of environmental, behavioural and metabolic risk factors that predispose to IHD, on the other.
Fortunately, effective interventions exist, including many that are low cost or cost effective and they should be explored and supported in Africa. Comprehensive approaches that combine environmental, policy and legislative interventions at the individual and population levels, especially for the prevention and control of high blood pressure, tobacco use, physical inactivity, obesity and diabetes are likely to have significant impact in Africa. Improved access to safe, effective and affordable drugs within the context of strengthened health systems for the delivery of primary healthcare, in general, and primary prevention, in particular, will be essential for averting a future epidemic of IHD in sub-Saharan Africa. We have the knowledge to accomplish all of this. However, as Goethe so aptly put it, “Knowing is not enough; we must apply. Willing is not enough; we must do.” For sub-Saharan Africa and most resource-poor settings, there can be no better time than now to act to prevent IHD from becoming epidemic. The time to do is now.
REFERENCES
Footnotes
Competing interests: None.
See Editorial, p 824
Disclaimer: The findings and conclusions in this manuscript are those of the author and do not necessarily represent the views of the Centers for Disease Control and Prevention.