Article Text

Abstract
Objective: To assess acute tissue plasminogen activator (t-PA) release in vivo in patients with hypercholesterolaemia in the presence and absence of lipid lowering treatment and in matched normocholesterolaemic controls.
Design: Parallel group comparison and double blind randomised crossover.
Setting: University hospital.
Patients: Eight patients with hypercholesterolaemia (> 7.8 mmol/l) and eight matched normocholesterolaemic controls (< 5.5 mmol/l).
Methods: Blood flow and plasma fibrinolytic factors were measured in both forearms during unilateral brachial artery infusions of the endothelium dependent vasodilator substance P (2–8 pmol/min) and the endothelium independent vasodilator sodium nitroprusside (1–4 μg/min).
Interventions: In patients, measurements were made on three occasions: at baseline and after six weeks of placebo or pravastatin 40 mg daily administered in a double blind randomised crossover design.
Main outcome measures: Acute release of t-PA.
Results: Compared with patients, in normocholesterolaemic control subjects substance P caused greater dose dependent increases in forearm blood flow (p < 0.05) but similar increases in plasma t-PA antigen and activity concentrations. During pravastatin treatment in patients, total serum cholesterol fell by 22% from a mean (SEM) of 8.1 (0.3) to 6.4 (0.4) mmol/l (p = 0.002) and substance P induced vasodilatation was no longer significantly impaired in comparison with controls. However, despite reproducible responses, pravastatin treatment was not associated with significant changes in basal or substance P induced t-PA release.
Conclusions: Hypercholesterolaemia and lipid lowering treatment cause no demonstrable effects on acute substance P induced t-PA release in vivo. This suggests that the preventative benefits of lipid lowering treatment are unlikely to be mediated by improvements in endogenous fibrinolysis.
- fibrinolytic factors
- hypercholesterolaemia
- lipid lowering treatment
- ELISA, enzyme linked immunosorbent assay
- FBF, forearm blood flow
- Hct, Haematocrit
- LDL, low density lipoprotein
- PAI-1, plasminogen activator inhibitor type 1
- t-PA, tissue plasminogen activator
- WOSCOPS, west of Scotland coronary prevention study
Statistics from Altmetric.com
- ELISA, enzyme linked immunosorbent assay
- FBF, forearm blood flow
- Hct, Haematocrit
- LDL, low density lipoprotein
- PAI-1, plasminogen activator inhibitor type 1
- t-PA, tissue plasminogen activator
- WOSCOPS, west of Scotland coronary prevention study
Hypercholesterolaemia impairs endothelial cell function,1–3 predisposes vessels to damage, and contributes to vascular occlusion.4 Previous studies have shown that endothelium dependent nitric oxide mediated vasodilatation is impaired in patients with hypercholesterolaemia,1–3 an effect that is reversed by lipid lowering treatment.5–7 Although other endothelial cell markers have been described,8,9 the fibrinolytic factor tissue plasminogen activator (t-PA) and its inhibitor, plasminogen activator inhibitor type 1 (PAI-1), are potentially important markers that are intimately linked to the risk of atherothrombosis.10,11
Endothelial cells in the precapillary arterioles and postcapillary venules12 synthesise and release t-PA and PAI-1 both basally and in response to various coagulation factors and stimulants. The rapid mobilisation of t-PA from the endothelium is crucial if endogenous fibrinolysis within the arterial circulation is to be effective, with thrombus dissolution being much more effective if t-PA is incorporated during, rather than after, thrombus formation.13,14 The importance of endogenous t-PA release is exemplified by the high rate of spontaneous reperfusion in the infarct related artery after acute myocardial infarction, which occurs in around 30% of patients within the first 12 hours.15
Epidemiological studies examining total plasma t-PA and PAI-1 concentrations in patients with ischaemic heart disease have observed a positive correlation with coronary events.10,11 It would be anticipated, however, that high t-PA concentrations would protect against subsequent coronary events rather than the reverse. This paradoxical association is, in part, explained by the concomitant increase of PAI-1, which complexes with t-PA and therefore causes an overall reduction in free t-PA “activity”.16,17 It is this free and unbound t-PA that is physiologically active and central to endogenous fibrinolysis. However, the capacity of endothelial cells to release t-PA from intracellular storage pools and the rapidity with which this can be mobilised may not necessarily be reflected in the basal circulating plasma concentrations of t-PA antigen or its activity.18,19 We have recently described an in vivo model to assess the acute release of t-PA in the forearm of humans.20 Using intrabrachial infusions of substance P, we have shown a dose dependent release of t-PA without causing a significant release in PAI-1. Moreover, we have also reported21 that t-PA release is inhibited by nitric oxide synthase inhibition with l-NG-monomethylarginine, suggesting that endothelial dysfunction may impair the release of t-PA.
Given that substance P induced vasodilatation has been reported to be impaired in patients with hypercholesterolaemia,3 the aims of the present study were to determine whether there is also an impairment of t-PA release in patients with hypercholesterolaemia and whether treatment with pravastatin5 could enhance t-PA release in these patients.
METHODS
Patients and control subjects
Eight patients with primary hypercholesterolaemia were recruited from the clinic if their serum cholesterol concentrations exceeded 7.8 mmol/l (> 296 mg/dl). Following screening with clinical examination, repeated questioning for symptoms, clinical chemistry screen (liver enzymes, electrolytes, urea, and creatine), haematology screen (full blood and differential counts), urinalysis, and 12 lead ECG, patients were excluded if they had diabetes mellitus, hypertension, ischaemic heart disease, peripheral vascular disease, an abnormal resting ECG, or other clinically significant disease. Patients were matched with normocholesterolaemic (< 5.5 mmol/l; < 209 mg/dl) healthy control subjects for age, sex, and smoking habit. All studies were undertaken with the approval of the local research ethics committee and in accordance with the Declaration of Helsinki. The written informed consent of each subject was obtained before entry into the study. None of the subjects was receiving vasoactive or non-steroidal anti-inflammatory drugs in the week before each phase of the study, and all abstained from alcohol for 24 hours and from food, tobacco, and drinks containing caffeine for at least nine hours before each study. All studies were performed in a quiet temperature controlled room maintained at 23.5–24.5°C.
Intra-arterial administration and drugs
The brachial artery of the non-dominant arm was cannulated with a 27 standard wire gauge steel needle (Cooper's Needle Works Ltd, Birmingham, UK) under 1% lignocaine (Xylocaine; Astra Pharmaceuticals Ltd, Kings Langley, UK) local anaesthesia. The cannula was attached to a 16 gauge epidural catheter (Portex Ltd, Hythe, UK) and patency was maintained by infusion of saline (0.9%; Baxter Healthcare Ltd, Thetford, UK) through an IVAC P1000 syringe pump (IVAC Ltd, Basingstoke, UK). The total rate of intra-arterial infusions was maintained constant throughout all studies at 1 ml/min. Pharmaceutical grade substance P (Clinalfa AG, Läufelfingen, Switzerland) and sodium nitroprusside (David Bull Laboratories, Warwick, UK) were administered following dissolution in saline.
Forearm blood flow and blood pressure
Blood flow was measured in both forearms by venous occlusion plethysmography using mercury in silastic strain gauges applied to the widest part of the forearm.22 During measurement periods the hands were excluded from the circulation by rapid inflation of the wrist cuffs to a pressure of 220 mm Hg using E20 rapid cuff inflators (DE Hokanson Inc, Bellevue, Washington, USA). Upper arm cuffs were inflated intermittently to 40 mm Hg for 10 s in every 15 s to achieve venous occlusion and obtain plethysmographic recordings. Analogue voltage output from an EC-4 strain gauge plethysmograph (DE Hokanson) was processed by a MacLab analogue to digital converter and Chart version 3.3.8 software (AD Instruments Ltd, Castle Hill, Australia) and recorded on to a MacIntosh Classic II computer (Apple Computers Inc, Cupertino, California USA). Calibration was achieved using the internal standard of the plethysmograph.
Blood pressure was monitored in the non-infused arm at intervals throughout each study using a semiautomated non-invasive oscillometric sphygmomanometer (Takeda UA 751, Takeda Medical Inc, Tokyo, Japan).23
Venous sampling and assays
Venous cannulae (17 gauge) were inserted into large subcutaneous veins of the antecubital fossa in both arms. Ten millilitres of blood was withdrawn simultaneously from each arm and collected into acidified buffered citrate (Biopool Stabilyte, Umeå, Sweden, for t-PA assays) and citrate (Monovette, Sarstedt, Nümbrecht, Germany, for PAI-1 assays) tubes, and kept on ice before being centrifuged at 2000 g for 30 minutes at 4°C. Platelet free plasma was decanted and stored at −80°C before assay.24
Plasma t-PA and PAI-1 antigen concentrations were determined using an enzyme linked immunosorbent assay (ELISA): Coaliza t-PA25 and Coaliza PAI-126 (Chromogenix AB, Mölndal, Sweden), respectively. Plasma t-PA and PAI-1 activities were determined by a photometric method: Coaset t-PA and Coatest PAI-1 (Chromogenix AB), respectively.27 Plasma PAI-1 activity is determined by a back titration method and represents the total t-PA inhibitory activity of the plasma.27 All fibrinolytic assays were performed in duplicate and the mean value was taken. Intra-assay coefficients of variation were 7.0% and 5.5% for t-PA and PAI-1 antigen and 4.0% and 2.4% for activity, respectively. Interassay coefficients of variability were 4.0%, 7.3%, 4.0% and 7.6%, respectively. The limits of sensitivity of the assays were 0.5 ng/ml, 2.5 ng/ml, 0.10 IU/ml, and 5 AU/ml, respectively. Haematocrit (Hct) was determined by capillary tube centrifugation of blood anticoagulated by ethylene diamine tetra-acetic acid and was obtained from the infused forearm at baseline and at 8 pmol/min of substance P. Serum cholesterol and triglyceride concentrations were determined by an enzymatic colorimetric method (Boehringer Mannheim GmbH Diagnostica, Mannheim, Germany). Low density lipoprotein (LDL) cholesterol was determined by the method of Friedewald and colleagues.28
Study design
All patients attended on each of the three study days: baseline and following six weeks' treatment with placebo and six weeks' treatment with pravastatin 40 mg daily. Placebo and pravastatin treatments were given in a randomised double blind crossover design. Control subjects attended on one occasion only.
On each study day, subjects attended fasted at 0900 and rested recumbent throughout. Strain gauges and cuffs were applied and the brachial artery of the non-dominant arm was cannulated. Throughout all protocols, forearm blood flow (FBF) was measured every 10 minutes. Before administration of substance P and sodium nitroprusside, saline was infused for 30 minutes to allow time for equilibration and the final blood flow measurement during saline infusion was taken as the basal FBF. Substance P was infused at 2, 4, and 8 pmol/min for 10 minutes at each dose19–21 and sodium nitroprusside was infused at 1, 2, and 4 μg/min for 10 minutes at each dose.20 The order of administration of substance P and sodium nitroprusside was randomised.
Data analysis and statistics
Plethysmographic data were extracted from the Chart data files and FBFs were calculated for individual venous occlusion cuff inflations by use of a template spreadsheet (Excel version 5.0; Microsoft Corporation, Redmond, Washington, USA). Recordings from the first 60 seconds after wrist cuff inflation were not used because of the variability in blood flow that this causes.22 Usually the last five flow recordings in each three minute measurement period were calculated and averaged for each arm. To reduce the variability of blood flow data, the ratio of flows in the two arms was calculated for each time point, in effect using the non-infused arm as a contemporaneous control for the infused arm.22 Percentage changes in the infused FBF were calculated22 as follows: where Ib and NIb are the infused and non-infused FBFs at baseline (time 0), respectively, and It and NIt are the infused and non-infused FBFs at a given time point, respectively.
where Ib and NIb are the infused and non-infused FBFs at baseline (time 0), respectively, and It and NIt are the infused and non-infused FBFs at a given time point, respectively.
Estimated net release of t-PA activity and antigen was defined previously19–21 as the product of the infused forearm plasma flow (based on the mean Hct and the infused FBF) and the concentration difference between the infused ([t-PA]Inf) and non-infused arms ([t-PA]Non-inf):

Data were examined, where appropriate, by two way analysis of variance with repeated measures and two tailed paired Student's t test using Excel version 5.0. Reproducibility of the responses to substance P infusion was assessed by comparing the baseline data with placebo treatment study days using the method of Bland and Altman.29 Coefficients of reproducibility were determined for 95% confidence intervals using the Student's t distribution. All results are expressed as mean (SEM). Significance was taken at the 5% level. On the basis of previous data20 the study had 90% power to detect a 20% change in plasma t-PA concentrations between treatment periods at the 5% level.
RESULTS
Table 1 shows patient and control subject characteristics. The groups were well matched for age, sex, body mass index, smoking habit, blood pressure, heart rate, Hct, and FBF. Total cholesterol and LDL cholesterol concentrations were significantly higher in the patient group and fell during pravastatin but not placebo treatment (table 1). On each of the study days in the patient and control groups, blood pressure, heart rate, Hct, blood flow, and t-PA concentrations of the non-infused forearm did not change.
Lipid profile, haemodynamics, absolute forearm blood flow, and haematocrit at baseline and during placebo and pravastatin treatment
Blood flow responses
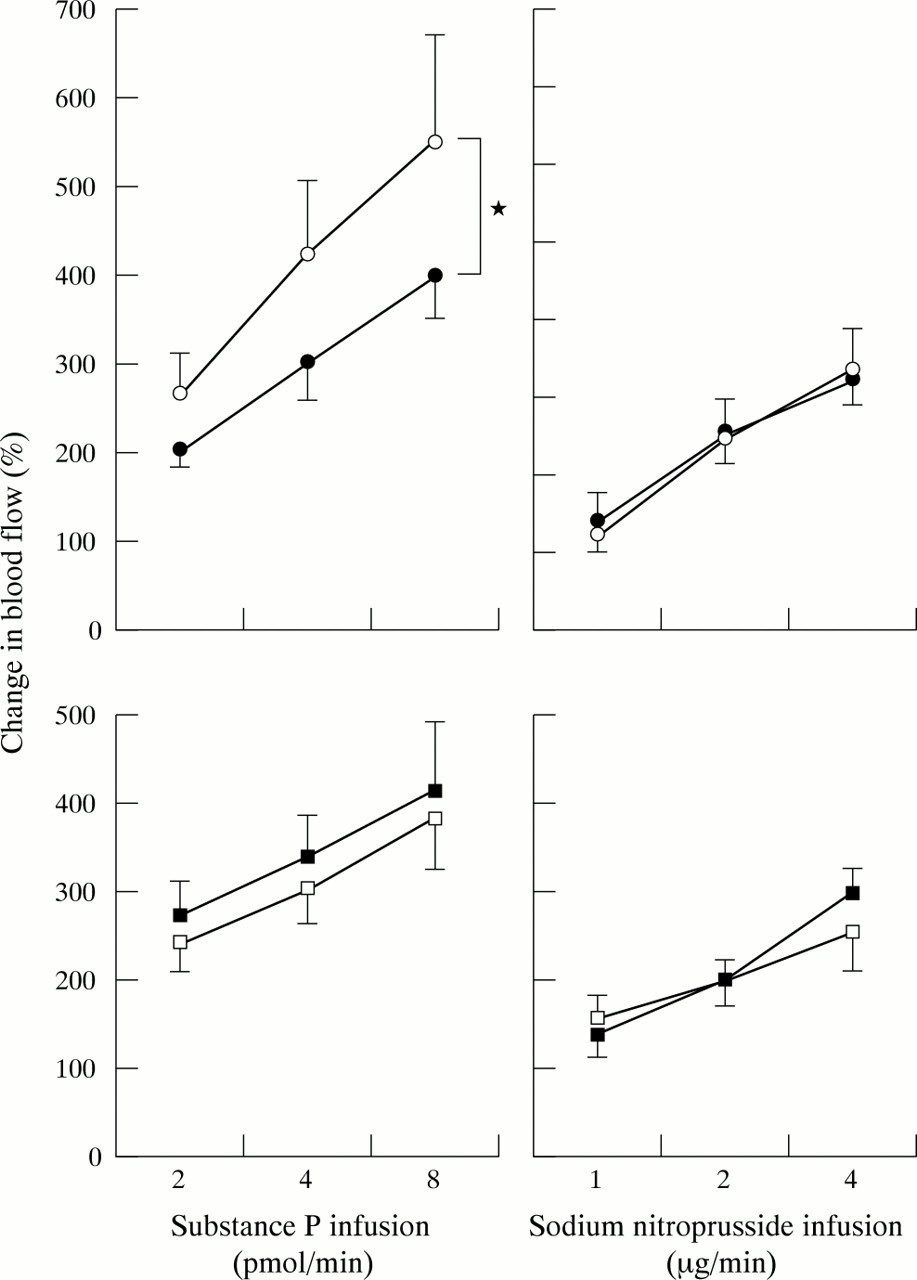
Substance P caused dose dependent increases in blood flow of the infused forearm in both patients and controls (p < 0.001 for both, analysis of variance; fig 1). In comparison to the control group, the substance P induced increases in blood flow were significantly less in the patient group (p < 0.05, two way analysis of variance; fig 1). During pravastatin treatment, substance P appeared to cause a slightly greater increase in blood flow but this was not significantly different from baseline responses (p = 0.30, two way analysis of variance, baseline versus pravastatin) although it was no longer significantly different from control group responses (p = 0.24, two way analysis of variance).

Forearm blood flow responses to substance P and sodium nitroprusside administration in control subjects (open circles, upper panels) and patients at baseline (closed circles, upper panels), and in patients during placebo (open squares, lower panels) and during pravastatin treatment (closed squares, lower panels). p < 0.001 for each forearm blood flow response (one way analysis of variance). *p < 0.05 (two way analysis of variance, controls versus patients).
Sodium nitroprusside also caused dose dependent increases in blood flow of the infused forearm (p < 0.001, analysis of variance; fig 1), which were similar in patient and control groups. Neither pravastatin nor placebo treatment influenced the response to sodium nitroprusside infusion.
Fibrinolytic factor responses
Substance P caused dose dependent increases in plasma t-PA antigen and activity concentrations in the infused forearm of both patients and controls (p < 0.001 for both, analysis of variance; table 2). Substance P induced increases in plasma t-PA concentrations were similar in both groups and, in the patient group, were unaffected by pravastatin or placebo treatment. The concentration differences between the forearms and the estimated net release of t-PA antigen and activity also increased dose dependently (p < 0.001, analysis of variance; fig 2), which did not differ between the patient and control groups or during pravastatin and placebo treatment. There were no significant differences in plasma PAI-1 antigen and activity concentrations at baseline, although there appeared to be a trend for plasma PAI-1 antigen concentrations to be lower in the control group (p > 0.12, unpaired t test; table 3). Plasma PAI-1 concentrations were unaffected by substance P infusion or pravastatin treatment (table 3).
Plasma tissue plasminogen activator (t-PA) antigen and activity in patients at baseline and during placebo and pravastatin treatment and in a matched control group
Plasma plasminogen activator inhibitor type 1 (PAI-1) antigen and activity in patients at baseline and during placebo and pravastatin treatment and in matched controls

{kind=link}
{kind=link}
Concentration difference between infused and non-infused forearms (upper panels) and estimated net release (lower panels) of plasma tissue plasminogen activator antigen (solid lines, left panels) and activity (dashed lines, right panels) during substance P administration in controls (open circles) and patients at baseline (closed circles), and during placebo (open squares) and pravastatin (closed squares) treatment. p < 0.001 for each response (one way analysis of variance).
Reproducibility of substance P responses
Comparison of responses at baseline and during placebo treatment shows good reproducibility for substance P induced increases in plasma t-PA concentrations and FBF (table 4).
Repeatability of t-PA and blood flow responses to substance P administration in the infused forearm: baseline versus placebo
DISCUSSION
Despite impaired endothelium dependent forearm vasodilatation, we have shown that in patients with hypercholesterolaemia intrabrachial substance P infusions are associated with a normal capacity to release t-PA acutely. Moreover, pravastatin treatment, sufficient to reduce cholesterol concentrations by 22%, had no significant effects on acute t-PA release. This suggests that, despite the presence of endothelial dysfunction, hypercholesterolaemia does not influence the acute fibrinolytic capacity of the endothelium and that the preventative benefits of lipid lowering treatment are unlikely to be mediated by improvements in endogenous fibrinolysis.
Consistent with previous findings,3 we have shown that in patients with hypercholesterolaemia, endothelium dependent vasodilatation in response to substance P infusion is impaired. However, in contrast to the pronounced impairment of t-PA release that we have recently described in cigarette smokers,19 hypercholesterolaemia and lipid lowering treatment do not appear to influence substance P induced t-PA release. These findings suggest that although smoking is associated with impaired endogenous fibrinolysis, hypercholesterolaemia is not. This is consistent with the observations that the patency rate of the infarct related artery following thrombolytic treatment during myocardial infarction is enhanced in cigarette smokers,30–32 but not in patients with hypercholesterolaemia,33 and that cigarette smoking is associated with thrombotic occlusion whereas hypercholesterolaemia is linked to atherogenesis and plaque rupture.4 This would also indicate that endothelial dysfunction can be manifest in separate distinct pathways depending on the nature of the insult.
The WOSCOPS (west of Scotland coronary prevention study)34 was the first major randomised controlled trial to show the primary preventative benefits of lipid lowering therapy. We therefore chose to examine the effects of pravastatin 40 mg daily on endothelial and fibrinolytic function in a well defined and otherwise healthy hypercholesterolaemic population. Although the total cholesterol was reduced by 22% and pravastatin was used at doses that have been shown to confer major preventative benefits in several large scale clinical trials,34–36 the total serum cholesterol concentration remained significantly higher than that in the normocholesterolaemic population. It may be that a greater reduction in cholesterol concentrations would have facilitated a significant improvement in endothelium dependent vasodilatation. However, the mean cholesterol concentrations of the patients in WOSCOPS were similar to those in the present study and the relative risk reduction in ischaemic events is the same across a broad range of cholesterol concentrations.35 Moreover, it appears that statins do not just lower cholesterol and may have many ancillary vascular actions.37 Finally, since we did not observe a significant difference in t-PA release between hypercholesterolaemic and normocholesterolaemic subjects, it is unlikely that additional reductions in lipid concentrations, brought about by higher doses of pravastatin or more potent statins, would influence the acute release of t-PA.
The influence of lipid lowering therapy on endothelial dysfunction was initially studied in patients with hypercholesterolaemia following treatment for 3–6 months.5,6 However, more recent studies have shown that endothelial dysfunction can be reversed by statin treatment for six38 or even four weeks.7 Indeed, two hour treatment with plasma LDL aphaeresis is associated with rapid and immediate reversal of endothelial dysfunction.39 It is therefore unlikely that the absence of an effect of pravastatin treatment is caused by the length of treatment and is consistent with a recent preliminary report from the WOSCOPS that showed no changes in basal plasma t-PA concentrations despite 12 months' treatment with pravastatin.40 Moreover, in contrast to previous studies, we have used a randomised double blind crossover study design that provides a greater sensitivity to detect potential differences in responses. The coefficients of reproducibility are consistent with our previous studies20,41 and indicate a power sufficient to detect an approximately 20% change in blood flow and fibrinolytic responses.
In summary, whereas endothelium dependent vasodilatation is abnormal in both cigarette smoking and hypercholesterolaemia, acute t-PA release appears to be impaired only by cigarette smoking.19 These observations support the concept that endothelial dysfunction is not a homogeneous condition and may be manifested in differing ways depending on the nature of the injury. Moreover, the benefits of lipid lowering treatment in the primary34 and secondary35,36 prevention of coronary events are unlikely to be mediated by improvements in endogenous fibrinolysis.
Acknowledgments
This work was supported by a grant from the British Heart Foundation (PG/96149). Dr Fraser Witherow was the recipient of a British Heart Foundation Junior Research Fellowship (FS/2000005). Professor David Webb was supported by a Research Leave Fellowship from the Wellcome Trust (WT 0526330). We would like to thank Laura Flint, Pamela Dawson and Margaret Millar for their assistance with this study.