Article Text

Abstract
Background: To test the hypothesis that a high C reactive protein (CRP) concentration would predict recurrence of atrial fibrillation (AF) after cardioversion in patients taking antiarrhythmic drugs.
Methods: 111 patients who underwent direct current cardioversion for symptomatic AF were enrolled. Blood was drawn for CRP determination before cardioversion on the same day. All patients were taking antiarrhythmic drugs before and after electrical cardioversion.
Results: After a mean follow up of 76 days, 75 patients had recurrence of AF. In univariate analysis, the median CRP concentration was significantly higher in patients with AF recurrence (3.95 mg/l v 1.81 mg/l, p = 0.002). Among the 55 patients with CRP in the upper 50th centile, 44 (80%) experienced recurrence of AF over a total follow up of 8.98 patient years, whereas among the 56 patients with CRP in the lower 50th centile, 31 (55%) experienced recurrence of AF over a total follow up of 14.3 patient years (p < 0.001). The adjusted hazard ratio comparing the upper 50th centile of CRP with the lower 50th centile of CRP was 2.0 (95% confidence interval 1.2 to 3.2, p = 0.007).
Conclusions: CRP is independently associated with recurrence of AF after electrical cardioversion among patients taking antiarrhythmic drugs. These results suggest that inflammation may have a role in the pathogenesis of AF resistant to antiarrhythmic drugs.
- AF, atrial fibrillation
- CI, confidence interval
- CRP, C reactive protein
- atrial fibrillation
- C reactive protein
- cardioversion
- recurrence
Statistics from Altmetric.com
Although ventricular rate control may be a viable treatment strategy for some patients with atrial fibrillation (AF),1 a strategy that achieves sinus rhythm may be preferable for patients with ventricular rates that are difficult to control or who remain symptomatic despite adequate ventricular rate control.2 Electrical cardioversion is an effective means to restore sinus rhythm, and the success of this procedure can be enhanced by the use of antiarrhythmic drugs.3 However, among patients taking antiarrhythmic drugs AF commonly recurs after cardioversion, usually within three months of cardioversion.4,5
Electrical or structural remodelling of the atria during AF may contribute to the high recurrence rates observed after cardioversion. Inflammation, necrosis, and fibrosis have been observed in atrial biopsies from patients with lone AF resistant to medical treatment.6 C reactive protein (CRP) has been found to be increased in patients with AF and may reflect an inflammatory state that promotes AF.7 A low level inflammatory response may be a part of the structural remodelling process that is associated with increased persistence of AF.
We hypothesised that increased CRP concentrations would predict recurrence of AF among patients with persistent AF taking antiarrhythmic drugs who undergo electrical cardioversion.
METHODS
Patients with persistent, symptomatic AF taking Vaughan-Williams class I or III antiarrhythmic drugs who were followed up as outpatients at our institution and underwent successful electrical cardioversion between November 2001 and August 2002 were enrolled in the study. Blood samples for CRP, routine chemical analysis, and international normalised ratio were drawn from all patients just before the cardioversion. All patients had precardioversion ECG and transthoracic echocardiography. Exclusion criteria were surgery within 60 days, an acute coronary syndrome within 60 days, history of recent infection, and history of collagen vascular disease. Our institutional review board approved the investigation.
Patients were followed up according to the usual standard of care. In addition, after cardioversion patients were instructed to call our arrhythmia clinic if they had any palpitations. These patients were then seen in the outpatient clinic as soon as possible. Recurrence of AF was defined as AF documented by ECG at any time after the cardioversion during the study time frame. CRP concentrations were assayed by immunonephelometry by the BNII analyser protocol (Dade Behring, Deerfield, Illinois, USA). CRP concentrations were determined with a typical detection limit of 0.175 mg/l (ultrasensitive CRP).
For statistical analysis, the independent samples t test was used when comparing approximately normally distributed variables between two groups. For non-normally distributed variables, the non-parametric Mann-Whitney U test was used when comparing variables between two groups. Categorical variables were compared by the χ2 test. The relation between recurrence of AF and baseline predictors was assessed by Cox proportional hazards regression modelling. For regression modelling, CRP was dichotomised at the median value and hazard ratios were computed for the upper versus lower 50th centiles of CRP. Regression modelling was done by a forward selection strategy in which variables were entered into the model if p < 0.20 and retained in the model if p < 0.30.8 All data were analysed with SPSS version 9.0 (SPSS Inc, Chicago, Illinois, USA). Results with p < 0.05 were considered significant. Because the distribution of CRP was skewed to the right, CRP concentration is presented as median with interquartile range, whereas other variables are presented as mean (SD).
RESULTS
One hundred and eleven patients (30 women and 81 men) with persistent AF who were taking antiarrhythmic drugs were enrolled in the study. After a mean follow up of 76 days (range 0.003–298 days), 75 (68%) patients had recurrence of AF. Table 1 presents the demographic and clinical characteristics of study participants according to AF recurrence. Both groups were comparable with respect to history of coronary artery disease and antiarrhythmic drugs used. Patients who experienced a recurrence of AF had a longer mean duration of AF but this was not significant (222 (479) days v 203 (345) days, p = 0.9) A higher proportion of patients with recurrence than with non-recurrence were women. Patients with AF recurrence tended to have larger left atria. The median CRP was significantly higher among patients with than among patients without AF recurrence (3.95 (2.19–6.13) mg/l v 1.81 (0.78–4.17) mg/l, p = 0.002).
Baseline characteristics of study patients according to recurrence of atrial fibrillation (AF) after cardioversion
Table 2 presents characteristics of study patients and AF recurrence rates according to CRP concentration dichotomised into upper and lower 50th centiles. Patients with coronary artery disease were more likely to have increased CRP. The median CRP among those with coronary artery disease was 4.24 mg/l, significantly higher than the median CRP of 2.53 mg/l among those without coronary artery disease (p = 0.007). Patients with CRP in the upper 50th centile had longer duration of AF (276 (546) v 157 (294) days, p = 0.3). Among the 55 patients with CRP in the upper 50th centile, 44 (80%) experienced recurrence of AF over a total follow up of 8.98 patient years (AF recurrence rate of 4.9/patient year), whereas among the 56 patients with CRP in the lower 50th centile, 31 (55%) experienced recurrence of AF over a total follow up of 14.3 patient years (AF recurrence rate of 2.2/patient year). The difference between these AF recurrence rates was significant (p < 0.001).
Characteristics of study patients according to lower and upper 50th centiles of CRP
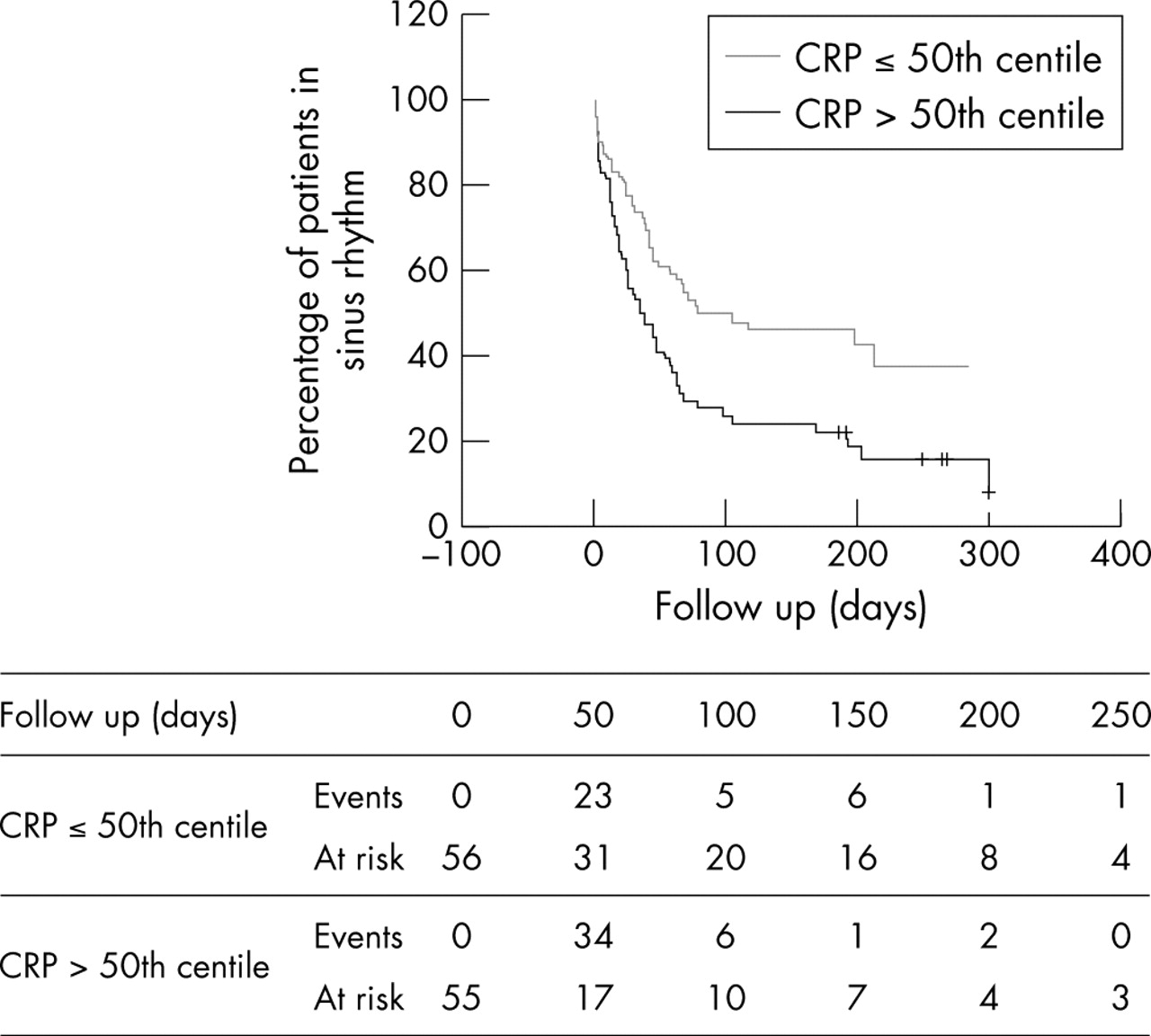
In a multivariable Cox regression model that considered age, sex, duration of AF, coronary artery disease, hypertension, left ventricular hypertrophy, left atrial dimension, and CRP, the independent predictors of AF recurrence were CRP, female sex, and left atrial diameter. The adjusted hazard ratio comparing the upper 50th centile of CRP with the lower 50th centile of CRP was 2.0 (95% confidence interval (CI) 1.2 to 3.2, p = 0.007), whereas the corresponding estimates for female sex and left atrial diameter (per centimetre increase) were 2.1 (95% CI 1.2 to 3.5, p = 0.006) and 1.4 (95% CI 1.1 to 1.8, p = 0.02), respectively. No other variables were retained in the final model. Figure 1 presents adjusted survival curves according to CRP concentration.
{kind=link}
Adjusted survival curves (percentage of patients in sinus rhythm over time) according to C reactive protein (CRP) concentration.
DISCUSSION
Previous studies have shown that younger age, smaller left atrial size, and shorter duration of AF are predictors of sinus rhythm maintenance.4 However, no biochemical marker has been shown to correlate with AF recurrence and many of the recurrences are thought to be secondary to electrical remodelling.9,10 The results of this study indicate that increased CRP concentrations are associated with higher rates of AF recurrence after cardioversion in patients with persistent AF taking antiarrhythmic drugs.
Atrial remodelling may result from several factors. These include chronic haemodynamic factors, such as hypertension and valvar heart disease, electrophysiological factors, and inflammation. Inflammation has been shown to play a part in postoperative AF. Bruins et al11 reported that the time of peak incidence of postoperative atrial arrhythmias correlates with a peak in CRP and CRP–complement complexes. In non-postoperative AF, histological studies have shown inflammatory changes and increased fibrosis in the atrial biopsies of patients with lone AF.6 In addition, Chung et al7 found that CRP concentrations are higher in patients with AF than in healthy controls. These authors also found that CRP concentrations were higher in patients with persistent AF than in those who have paroxysmal AF, suggesting that inflammation may promote the persistence of AF.7
Recently studies have shown that the use of anti-inflammatory agents is associated with a decreased incidence of AF. In a recent study by Cheruku et al,12 the use of the non-steroidal anti-inflammatory drug ketolorac significantly reduced AF after coronary artery bypass grafting. This was attributed to a decrease in inflammation caused by the non-steroidal anti-inflammatory drug.12 Statins, which have been shown to decrease inflammation,13 also decreased the incidence of AF in recent studies in both animal models and humans.14–17 In addition, recent studies have shown that angiotensin converting enzyme inhibitors may decrease the incidence of AF in patients with reduced left ventricular ejection fraction.18 Furthermore, angiotensin converting enzyme inhibitors have recently been shown in to decrease inflammation.19–22 Madrid et al23 reported that adding the angiotensin receptor blocker irbesartan to amiodarone enhanced the probability of remaining in non-sinus rhythm after cardioversion of patients with persistent AF. This effect was attributed to the possible beneficial effects of blockade of the angiotensin receptor on apoptosis, fibrosis, and electrical remodelling.24–26 These results suggest that inflammation may have a causal role in the pathogenesis of AF.
Limitations
This was an observational study of consecutive patients taking antiarrhythmic drugs who underwent successful cardioversion. The period over which data were collected was arbitrarily selected. As there were no good prior data, sample size could not be estimated. However, CRP is a marker of inflammation and there is evidence to suggest that inflammation may have a causal role in some forms of AF. However, because this was an observational study, determining causation was problematic.
In our dataset, duration of AF was not strongly related to AF recurrence or to CRP concentration. However, it is important to note that duration of AF in this study refers to how long the patient had been in AF at the time of the cardioversion and not to the duration since AF was first detected. We did not have reliable data on when AF was first diagnosed and so could not take this into account with our analysis.
Lastly, as with all observational studies, confounding caused by factors that were not accounted for is possible. We did restrict our study sample to patients taking antiarrhythmic drugs; although this was not a bias, it may affect the generalisability of the study results.
Conclusion
This study shows that CRP concentrations independently predict recurrence of persistent AF after cardioversion. As was the case in previous studies, from our results we cannot conclude that CRP has a causal role or that AF has an inflammatory basis.7 Nevertheless, among this patient population we saw significantly higher CRP concentrations in the recurrence group than in the non-recurrence group. Inflammation may be more pathogenetic in promoting persistence of AF as Chung et al7 pointed out.
Increased CRP concentration may be a marker of more extensive atrial remodelling that may lead to lower effectiveness of antiarrhythmic drugs. Whether treatments that reduce inflammation and CRP are useful in treating patients with AF warrants further study.
REFERENCES
Footnotes
-
Published Online First 12 May 2005