Article Text

Abstract
Cognitive impairment in cardiac patients may interfere with disease management. This review describes studies examining specific cognitive impairments in cardiac patients and studies that investigate the link between echocardiographic and cognitive measures. Executive function impairments were frequently reported in different patient groups. Also, lower cardiac output and worse left ventricular diastolic function are linked to executive function deficits. In cardiac patients, special attention should be paid to these executive function impairments in view of their role in disease management and independent living. Interventions that stimulate executive function should be encouraged and integrated in cardiac treatment protocols.
- Cardiac diseases
- heart failure
- echocardiography
- cardiac output
- cognition
- psychology/psychiatry
- cardiac function
- neurology
- hypertension
- ACE
- angiotensin receptor blockers
- epidemiology
- stroke
- atrial fibrillation
- contrast echocardiography
- echocardiography (three-dimensional)
- myocardial infarction
- stress echocardiography
Statistics from Altmetric.com
- Cardiac diseases
- heart failure
- echocardiography
- cardiac output
- cognition
- psychology/psychiatry
- cardiac function
- neurology
- hypertension
- ACE
- angiotensin receptor blockers
- epidemiology
- stroke
- atrial fibrillation
- contrast echocardiography
- echocardiography (three-dimensional)
- myocardial infarction
- stress echocardiography
Introduction
The increasingly expanding ageing population has resulted in a higher prevalence of cardiac disease and due to treatment possibilities patients live longer. Frequently prevalent cardiac diseases in the older population include coronary artery disease, that is, 43% of men and 41% of women aged 81 years, and atrial fibrillation, that is, 13% of persons aged 81–90 years.1 The proportion of heart failure patients increases with age and heart failure patients with preserved ejection fraction account for about half of clinical heart failure patients.2
Although these diseases can be handled better due to current medical care, embolic stroke or chronic cerebral hypoperfusion due to for instance atherosclerosis or reduced cardiac output may lead to cognitive impairment.3 In fact, cardiac disease is associated with increased risk for cognitive impairment4 ,5 and dementia.6 ,7 More specifically, large cohort studies have revealed a link between increased risk for dementia and for instance atherosclerosis6 and atrial fibrillation.8 Naturally, having dementia restricts one's possibility to effectively manage care of a concomitant medical condition. Cognitive impairment not necessarily leading to dementia may however also limit an individual in managing one's health when facing a complex chronic illness. Specific cognitive deficits, that is, memory impairment and executive function deficits such as problems with regulation of one's behaviour may negatively influence self-management of an illness, such as reduced medication adherence.3 ,9 Other executive function deficits such as planning difficulties and reduced cognitive flexibility may result in missed appointments and inability to make diet changes. In general, intact executive functions are crucial for the management of chronic conditions.10
The majority of case–control studies concerning the relationship between cardiac function and cognition have focused on cognitive performance in heart failure patients.4 ,11 There are fewer studies examining cognition in persons with a further specified cardiac disease as heart failure with either impaired or preserved ejection fraction, or another type of cardiac disease such as atrial fibrillation. The aims of the present review are twofold: the first aim is to provide an overview of studies that investigate the presence of cognitive impairments in patients with a specific type of cardiac disease. Since the origin of specific cognitive impairments in cardiac patients is likely multi-factorial,3 the second aim of the study is to include studies that investigate the relationship between cognitive impairments and cardiac function measured by echocardiography.
Methods
Search strategies and selection criteria
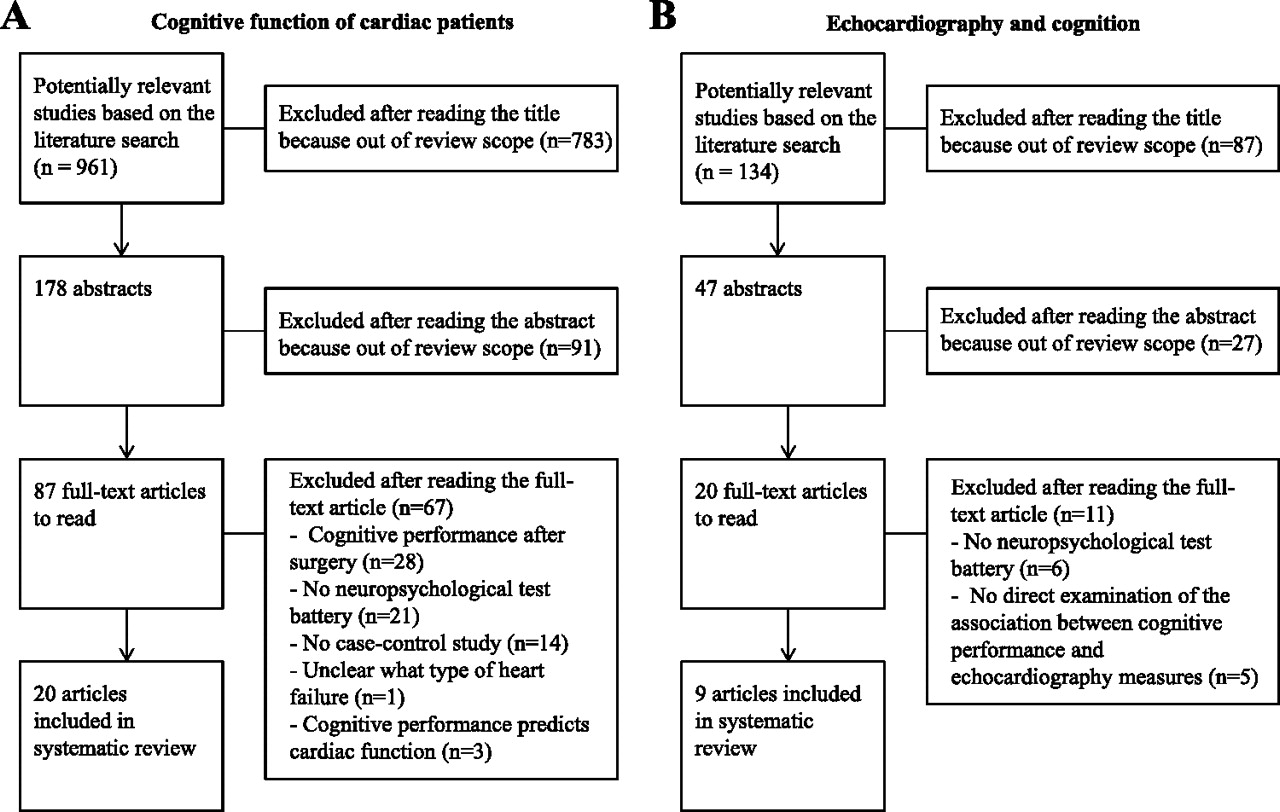
The literature search aimed for studies that included adults and were written in the English language. The first search focused on studies concerning presence of specific cognitive deficits in cardiac patients. Only studies using neuropsychological tests covering specific cognitive functions were included. With respect to the heterogeneous group of heart failure patients we included studies that mentioned ejection fraction, and focused on systolic heart failure patients and/or patients with heart failure and preserved ejection fraction, since the presence of cognitive deficits in heart failure patients in general has been reviewed already.4 ,11 Inclusion and exclusion of studies and MeSH terms used are presented in figure 1A and appendix 1, respectively. The quality of the included studies was independently assessed by two authors (LHPE and JCJ) using the Newcastle-Ottawa Scale.12 This scale rates the quality of case–control studies and cohort studies in terms of the selection of participants; four criteria, comparability of study groups; one criterion, and outcome assessment; three criteria. Rating scores range from 1 to 9 points, and higher scores indicate better study quality. Differences in rating were resolved by consensus. Details concerning the studies including ratings are presented in tables 1–4. Finally, to explore the relationship between cardiac function and cognition, a separate search was performed (see appendix 1). For inclusion and exclusion of studies in this search and details on the included studies see figure 1B and table 5, respectively.
{kind=link}
Flowcharts. (A) Literature search and study selection concerning presence of specific cognitive deficits in cardiac patients. (B) Literature search and study selection concerning the relationship between echocardiography and cognition.
Characteristics of studies examining cognitive function in patients with coronary artery disease
Characteristics of studies examining cognitive function in patients with atrial fibrillation
Characteristics of studies examining cognitive function in patients with systolic heart failure
Characteristics of studies examining cognitive function when comparing systolic heart failure patients and heart failure patients with preserved ejection fraction
Characteristics of studies examining cognitive function related to echocardiographic measures
Review outline
First, specific cognitive deficits in persons with cardiac disease will be discussed, that is, persons with coronary artery disease, persons with atrial fibrillation and persons with systolic heart failure or heart failure with preserved ejection fraction. In addition, studies investigating the relationship between echocardiographic measures and cognitive functioning are described. Finally, implications of these findings will be addressed and the potential role for interventions will be explored.
Specific cognitive deficits in patients with cardiac disease
Coronary artery disease and global cognitive impairment
One case–control study looked at the cognitive performance of persons scheduled for coronary artery bypass graft (CABG) surgery. Before surgery, performance on several cognitive tests was lower compared with controls, particularly concerning performance on a verbal memory test.14 A longitudinal study including on-pump CABG patients, off-pump CABG patients, non-surgical patients with coronary artery disease and controls showed that all patients with coronary artery disease showed worse motor speed, psychomotor speed and global cognitive function.13 After 6 years of follow-up, all coronary artery disease patients showed mild but significant decline in visual memory, visuoconstruction, executive function and global cognition compared with controls.13
Larger cohort studies investigated whether coronary artery disease was a significant predictor of cognitive decline. Although coronary artery disease was particularly associated with reduced verbal fluency and lower general cognitive function in one study,18 coronary artery disease was not associated with several cognitive measures in another.15 A population-based cohort study that looked at subtypes of mild cognitive impairment reported that coronary artery disease was significantly associated with non-amnestic mild cognitive impairment, but not with amnestic mild cognitive impairment.16 A longitudinal 6-year follow-up study examined the relationship between cognitive function and coronary artery disease.17 It was shown that history of coronary artery disease was associated with lower scores on measures of global cognition, reasoning and vocabulary in men, and also with lower verbal fluency in women.17
Taken together, there are limited studies that examined cognitive impairments in persons with coronary artery disease patients without surgical intervention. The general finding is that coronary artery disease is a risk factor for global cognitive deficits in the long run.
Atrial fibrillation and cognitive inflexibility
Some case–control studies show lower performance on cognitive tests in patients with atrial fibrillation when compared with controls,19 ,20 but not all studies show significant differences.21 Cognitive deficits that have been reported include verbal memory impairment and cognitive inflexibility.19 ,20 Unfortunately, most of these case–control studies used a small sample size.
Cohort studies report reduced global cognitive functioning and specific cognitive deficits in persons with atrial fibrillation, such as reduced abstract reasoning, visual and verbal memory deficits, and executive function deficits, that is, cognitive inflexibility.22 ,23
A smaller cohort study did not find support for atrial fibrillation as a predictor for overall cognitive decline,24 but this study did not include a domain specifically measuring executive functioning.
In sum, both case–control and cohort including studies indicate impairment associated with atrial fibrillation in several cognitive domains, including executive function deficits. Although not all cognitive functions may be impaired, special attention for lack of cognitive flexibility is warranted.
Cognitive deficits in heart failure patients seem related to ejection fraction
Several studies investigated the presence of cognitive impairments in systolic heart failure patients compared with controls. One case–control study showed impaired verbal memory and vigilance in systolic heart failure patients with idiopathic dilated cardiomyopathy.29 Of note is that the patients also revealed more symptoms of depression and anxiety, which may partly explain results.29 Compared with healthy controls, patients with systolic heart failure showed significantly lower scores on several cognitive domains.25 In two other studies including patients with cardiovascular disease, those with systolic heart failure showed verbal memory deficits and executive functions deficits, such as cognitive inflexibility.27 ,28 A small study including patients with previous myocardial infarction, no differences were found between those with systolic heart failure and those without.26
Other studies compared systolic heart failure patients and heart failure patients with preserved ejection fraction. One study showed a significant interaction between age and ejection fraction for verbal memory performance; older heart failure patients showed a significant decline in memory when ejection fraction dropped below 30%.30 In another study, persons with coronary artery disease and the lowest ejection fraction showed worse global cognitive performance, worse visuoconstruction and slower motor speed.31 A recent study examined cognitive functioning and determined presence of heart failure in the general older population.32 Presence of both systolic heart failure and heart failure with preserved ejection fraction was associated with lower performance on attention and executive function tasks.32
In sum, cognitive test performance on various domains in systolic heart failure patients seems to be worse compared with healthy controls. In case systolic heart failure patients are compared with heart failure patients with preserved ejection fraction, differences in performance are much smaller.
Echocardiography measures are related to executive function deficits
Most studies examining the relationship between cardiac function and cognition focus on ejection fraction and cardiac output. A study including a group of cardiac rehabilitation patients showed that those with reduced ejection fraction scored significantly lower on measures for global cognition, language, psychomotor speed and verbal memory than those with higher ejection fraction.39 Two small studies including older patients with cardiovascular disease showed a relationship between lower ejection fraction and worse performance on tests measuring sustained attention and vigilance.38 ,40 Other small studies revealed that in older patients with cardiovascular disease, executive function deficits, particularly cognitive inflexibility and planning difficulties, were associated with reduced cardiac output.33 ,35
Large cohort studies such as the Framingham Offspring study confirmed the relationship between lower cardiac output and reduced cognitive flexibility.36 This study also revealed that participants' left ventricular mass was inversely associated with abstract reasoning, visuospatial memory and verbal memory, but not after adjustment for cardiovascular diseases.34 This large cohort study recently discussed a non-linear, that is, U-shaped, association between ejection fraction and cognitive test performance.37 Compared with the referent (quintiles 2–4), the lowest quintile and the highest quintile ejection fraction values were associated with lower scores on the memory and visuospatial organisation/executive function tests. Finally, a longitudinal study of the general population revealed that baseline markers of left ventricular diastolic and systolic dysfunction were associated with lower scores on tasks measuring attention and executive function after several years' follow-up.32
Summarising, in heterogeneous groups of older persons with cardiovascular disease, executive function impairment, that is, cognitive inflexibility, often appears to be related to reduced cardiac output or to reduced left ventricular diastolic function. Results concerning the relationship between cardiac output and executive function have however not been entirely consistent; one explanation could be that this relationship between left ventricular systolic function and cognition may not be linear, but may rather show an inverted-U curve.
Discussion
This review shows that while persons with coronary artery disease mostly reveal general cognitive deficits, persons with atrial fibrillation tend to show deficits particularly in the executive function domain. In persons with heart failure, most studies included persons with systolic heart failure who generally show cognitive impairments when compared with healthy controls. When systolic heart failure patients are compared with heart failure patients with preserved ejection fraction, differences in cognitive function are less apparent. Unfortunately, these studies only include a limited number of heart failure patients with preserved ejection fraction and not all studies include measures of executive function. Finally, in persons with cardiovascular disease those with reduced ejection fraction or cardiac output show more executive function impairments, particularly cognitive inflexibility, compared with those with preserved ejection fraction or cardiac output. These executive function impairments put cardiac patients at risk for poor disease management and functional dependence.3 ,9 More specifically, it was recently shown that acute cardiac patients, particularly those with heart failure, have increased risk for several negative health outcomes including general cognitive impairment, frailty and depression.41
Cardiac output is one mechanism underlying cognitive deficits
The relationship between cognition and echocardiographic measurements in patients with cardiovascular disease can be explained by reduced cardiac output due to impaired pump function. Reduced cardiac output may lead to systemic hypoperfusion and vascular dysfunction, increasing the risk for cerebrovascular disease and cerebral hypoperfusion.3 Concordantly, cerebral blood flow velocity during cognitive activation was significantly lower in cardiac disease patients compared with healthy controls.42 Reduced cardiac output and cerebral hypoperfusion may subsequently lead to cerebrovascular pathology and brain atrophy3 ,43 and specific cognitive function deficits such as attention deficits and executive function impairments in older adults with cardiovascular disease.38 ,44 However, this review does not find consistent support for a linear relationship between cardiac output and cognitive deficits. In fact, evidence points to a relationship that shows an inverted-U curve.37 Other psychosocial factors may also contribute to cognitive deficits in cardiac patients. Cardiac disease is for instance related to multi-pharmacotherapy,3 higher levels of depressive symptoms, marital problems and sleep disturbances,45 all factors that might negatively affect cognitive function and treatment adherence in cardiac patients.
Neuroimaging studies may enlighten relationship cardiac function and cognition
Other underlying mechanisms causing cerebrovascular pathology and brain atrophy are atherosclerosis and atrial fibrillation.46 ,47 Cerebrovascular pathology, such as white matter lesions, may also be an explanation for the reported vulnerability of cognitive flexibility in patients with atrial fibrillation and cardiac patients with lower ejection fraction. More specifically, cognitive flexibility requires functional connectivity of fronto-striatal networks,48 networks which are particularly vulnerable to infarction.49 Neuroimaging techniques such as diffusion tensor imaging could be very useful in the characterisation of neuropathology underlying these cognitive deficits by detecting disruption of functional white matter connectivity.50 Besides use of innovative neuroimaging techniques, cardiology clinics in medical centres could add standard neuropsychological assessment as well.
Standard neuropsychological testing in cardiac settings
The present review included studies that assessed extensive neuropsychological test batteries in order to determine the relation between cardiac function and specific cognitive functions. Of note is that not all studies used neuropsychological measures of executive functions. Future studies should include an extensive battery of neuropsychological tests, including tests that assess cognitive flexibility, and should also take into account possibly mediating factors such as medication use and depressive symptoms. More insight in the relationship between impaired cardiac function and executive function deficits such as cognitive inflexibility is of particular importance in view of the crucial role for executive functions in a person's autonomy. In daily clinical practice, however, there may not be sufficient time to assess a full neuropsychological test battery. Studies included in this review measure different cognitive functions and make use of varying test instruments. One cognitive function that seems particularly vulnerable in patients with atrial fibrillation and persons with reduced cardiac output is cognitive flexibility. A widely used instrument to determine cognitive flexibility is the Trailmaking Test.51 This test is sensitive to the presence of frontal lobe pathology and increased cerebrovascular risk and is easily applied in a time-restricted clinical setting.52
Improving cognition through cardiac treatment
Cardiac function has a potentially modifiable nature, for instance, through medication; therefore, we emphasise the need to further explore the effects of cardiac treatment on cognition. After different types of surgical procedures in patients with coronary artery disease there appear to be differences in short-term cognitive outcomes. Minimal extracorporal circulation surgery seems to result in better cognitive functioning 3 months after the surgery compared with conventional extracorporal circulation surgery.53 These short-term cognitive deficits could be partly explained by reduced levels of cerebral perfusion.53 Although early postoperative cognitive impairments have commonly been reported after CABG, cognition appears to normalise after 3 months.13 Cognitive decline in patients with coronary artery disease on the long run is frequent, but appears to be unrelated to the use of cardiopulmonary bypass or even CABG surgery altogether.13 ,54 Nonetheless, to prevent early cognitive deficits after surgery, minimal extracorporal circulation procedures are recommended.54 Other intervention studies also provide evidence for beneficial effects on cognition by cardiac treatment. One small study for instance showed that by improving left ventricular ejection fraction following cardiac resynchronisation therapy, both scores on a global cognition measure and on a combined measure of executive function tests improved.55 Within this line of reasoning, since physical activity is generally beneficial for patients with cardiac disease and physical activity programmes improve cognition in older adults,56 the effects of physical activity on cognition in cardiac disease patients is of interest. Only one study actually examined the effects of exercise on cognition in patients with coronary artery disease (n=12) and heart failure (n=12) who participated in an exercise programme.57 Directly after a 3-week ergometer training intervention, participants showed improved performance on arithmetic and memory measures. Future studies offering a physical activity programme to cardiac patients that include measures of different cognitive domains, echocardiography and neuroimaging would contribute substantially to the existing knowledge concerning this topic.
Summary
General cognitive impairments in cardiac disease patients have not been reported consistently. Nonetheless, more specific cognitive impairments, for instance cognitive inflexibility, have particularly been reported in patients with atrial fibrillation and persons with reduced cardiac output. These specific impairments may have a crucial impact on the patient's self-management of the cardiac condition. More insight in specific factors involved in the relationship between cardiac function and cognition may lead to the identification of patients most likely to experience executive function deficits and to those most likely to cognitively benefit from cardiac treatment or exercise.
Appendix
Key words used for the part of the review concerning presence of specific cognitive deficits in cardiac patients included the MeSH terms: heart diseases OR cardiac arrhythmias OR cardiomyopathies OR heart valve disease OR myocardial ischemia OR heart failure OR diastolic heart failure OR systolic heart failure OR ventricular dysfunction in combination with the MeSH terms cognition OR attention OR memory OR executive function in combination with the MeSH terms adult OR patients OR persons. To explore the relationship between cardiac function and cognition, a search was performed including the MeSH terms: echocardiography OR stroke volume OR cardiac output OR atrial function OR ventricular function OR systole OR diastole AND cognition OR attention OR memory OR executive function. For inclusion and exclusion of studies see figure 1.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.