Article Text

Abstract
Objective To evaluate whether interventions aimed at increasing adherence to therapeutic exercise increase adherence greater than a contextually equivalent control among older adults with chronic low back pain and/or hip/knee osteoarthritis.
Design A systematic review and meta-analysis.
Data sources Five databases (MEDLINE (PubMed), CINAHL, SportDISCUS (EBSCO), Embase (Ovid) and Cochrane Library) were searched until 1 August 2016.
Eligibility criteria for selecting studies Randomised controlled trials that isolated the effects of interventions aiming to improve adherence to therapeutic exercise among adults ≥45 years of age with chronic low back pain and/or hip/knee osteoarthritis were included.
Results Of 3899 studies identified, nine studies (1045 participants) were eligible. Four studies, evaluating strategies that aimed to increase motivation or using behavioural graded exercise, reported significantly better exercise adherence (d=0.26–1.23). In contrast, behavioural counselling, action coping plans and/or audio/video exercise cues did not improve adherence significantly. Meta-analysis using a random effects model with the two studies evaluating booster sessions with a physiotherapist for people with osteoarthritis revealed a small to medium significant pooled effect in favour of booster sessions (standardised mean difference (SMD) 0.39, 95% CI 0.05 to 0.72, z=2.26, p=0.02, I2=35%).
Conclusions Meta-analysis provides moderate-quality evidence that booster sessions with a physiotherapist assisted people with hip/knee osteoarthritis to better adhere to therapeutic exercise. Individual high-quality trials supported the use of motivational strategies in people with chronic low back pain and behavioural graded exercise in people with osteoarthritis to improve adherence to exercise.
- Osteoarthritis
- Exercise
- Lower back
- Intervention
- Meta-analysis
Statistics from Altmetric.com
Introduction
Chronic low back pain and osteoarthritis, typically affecting the hip and/or knee, are the most common causes of musculoskeletal pain in older adults worldwide.1 Both conditions are debilitating due to chronic pain and physical dysfunction, leading to significant loss of quality-of-life and substantial societal impact.2 ,3 The incidence of chronic low back pain and osteoarthritis is expected to rise.4 ,5 Management of both conditions focuses on preventing unnecessary disability, minimising pain and maintaining optimal function, with a combination of pharmacological and non-pharmacological therapies.6 ,7 Therapeutic exercise is a core component of self-management of chronic low back pain and osteoarthritis in older adults.7–9
Therapeutic exercise is participation in physical activity that is planned, structured, repetitive and purposeful for the improvement or maintenance of a specific health condition (or disease).10 This definition encompasses general aerobic exercise, strengthening, flexibility, balance or body-region-specific exercises. There is high-quality evidence that exercise improves pain and function in older adults with chronic low back pain and lower limb osteoarthritis.2 ,11 ,12 Although exercise provides immediate and short-term clinically worthwhile effects,11 ,13–15 adherence to exercise declines significantly over time among older adults with chronic low back pain and those with hip/knee osteoarthritis.11 ,14 ,15 Similar barriers to exercise adherence, such as fear of movement and pain aggravation, time management and uncertainty about the benefits of exercise have been reported across these populations.16–19 As such, increasing adherence to exercise programmes is recognised as an important factor for longer term effectiveness.20
Adherence is defined as the extent to which a person's behaviour corresponds with the agreed recommendations from healthcare providers.21 Various strategies to improve adherence to exercise have been explored among people with chronic musculoskeletal problems, including education, goal setting, supervision of exercises and the use of self-monitoring techniques such as an exercise diary. A 2010 Cochrane review22 evaluated the efficacy of interventions to improve adherence to exercise for people with chronic musculoskeletal pain. While the authors concluded that supervised or individualised exercise therapy and self-management techniques may enhance adherence, they noted uncertainty in the findings as effects were inconsistent across included studies. Similarly, a recent systematic review found limited evidence for interventions to increase exercise adherence among people with osteoarthritis and rheumatoid arthritis.23 However, both of these systematic reviews are limited by the use of very broad inclusion criteria that included studies that could not isolate the specific effects of adherence strategies included within interventions. To draw accurate conclusions from experimental studies, the only difference between a control and target intervention should be the active ingredients hypothesised to produce benefit.24 An analysis of the 2010 Cochrane review found that the contextual equivalence of the control and target interventions of the included studies was low, significantly limiting the conclusions that could be drawn about the effects of adherence interventions.25 A similar limitation also applies to the systematic review by Ezzat et al.23
The primary objective of this study was to systematically review and describe randomised controlled trials (RCTs) evaluating interventions to increase adherence to therapeutic exercise, compared with contextually equivalent control interventions, among older adults with chronic low back pain and/or hip/knee osteoarthritis. A secondary aim was to perform meta-analysis on homogeneous RCTs to determine if interventions are effective at increasing exercise adherence.
Methods
The review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.26 The protocol for this systematic review was not registered.
Search strategy
The search strategy was developed in consultation with a research librarian from the University of Melbourne. Three components of the search strategy were developed separately (population, exercise, adherence) then combined using database-specific truncation terms. MESH headings and keywords were used for each term. The full MEDLINE (PubMed) search strategy is detailed in online supplementary appendix 1. The following electronic databases were searched by one reviewer (PN) from their inception until 1 August 2016: MEDLINE (PubMed), CINAHL, SportDISCUS (EBSCO), Embase (Ovid) and Cochrane Library. The reference lists of any relevant systematic reviews found by the search were screened to identify potentially eligible additional primary studies. Supplementary searches of the reference lists of included studies were also undertaken.
supplementary appendix
Study selection
RCTs involving therapeutic exercise for people 45 years or older with chronic (>3 months) low back pain and/or hip/knee osteoarthritis were considered eligible. Where mixed populations of participants were reported, only those with 50% or more meeting the above population criteria were included. Any form of therapeutic exercise was eligible, including aerobic exercise, strengthening exercise, balance exercise and so on. Studies were required to test an intervention that aimed to improve adherence to therapeutic exercise. To be eligible, the control arm of included studies was required to receive therapeutic exercise comparable to the intervention arm, such that the only point of difference between control and intervention groups was the specific adherence strategy under investigation. RCTs that compared the effectiveness of two or more different adherence strategies were eligible, as long as all other treatment elements (including the exercise programmes) remained similar across trial arms. Studies were required to measure exercise adherence. Any quantitative measure of exercise adherence was deemed eligible, including numerical rating scales and logbook/diary measures. Studies not available in English, conducted on animals or published in abstract form only were excluded.
A two-step process was used for study screening and selection, using the eligibility criteria outlined above. In the first step, titles and abstracts of all identified studies were independently screened by two reviewers in a standardised manner (AVG and PJAN). Disagreement regarding potentially eligible studies was resolved independently by a third reviewer (MAH). Following title and abstract screening, the full text of all potentially eligible articles was retrieved and each screened independently for final inclusion by the same two reviewers (AVG and PJAN). Inter-rater agreement was measured by calculating percentage agreement and the κ coefficient. Any differences regarding final eligibility were independently resolved by a third reviewer (MAH) as required.
Data extraction
A data extraction form was developed by multiple authors, independently piloted by two authors (PJAN and RSH) and subsequently adjusted to ensure all relevant data were captured. Two authors (AVG and PJAN) independently extracted data from the included study reports using the standardised form. Disagreements were resolved by discussion between the two review authors. If no agreement could be reached it was planned that a third author (RSH) would independently adjudicate. Descriptive data extracted from each study included: study location, inclusion criteria, characteristics of study participants (sample size, age, gender), content of adherence and control group interventions (number and length of sessions, exercise type, mode of delivery, any additional intervention components), whether behaviour change theory was used in developing the adherence intervention, outcomes used to measure exercise adherence and time points of outcome measurement. For each study, data regarding the effects of the adherence intervention on exercise adherence were extracted for each adherence outcome measure at each measured time point. We extracted means (SDs) or medians (IQR) or OR (95% CI) for adherence outcome measures as appropriate, along with results of relevant between-group statistical comparisons. We contacted authors for data when insufficient information was reported in the study publication.
Quality of intervention reporting
For each study, the Template for Intervention Description and Replication (TIDieR) checklist was applied to assess the quality of description of the interventions evaluated.27 This checklist consists of 12 items that constitute complete and replicable reporting of interventions (brief name, why, what (materials), what (procedure), who provided, how, where, when and how much, tailoring, modifications, how well (planned) and how well (actual)).27
Risk of bias assessment
The degree of bias in included studies was assessed independently by two authors (PJAN and AVG) using the Cochrane Risk of Bias Tool.28 This tool rates seven potential sources of bias across six domains (sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and ‘other sources of bias’). Each potential source of bias was rated as low, unclear or high risk. Where there was disagreement between raters, discrepancies were resolved by discussion and consensus with a third author (FLD), if necessary. Absolute agreement and an estimate of level of agreement between reviewers who rated the risk of bias in included studies were assessed by calculating percentage agreement and the κ coefficient for the total number of items of the Cochrane Risk of Bias Tool.11
Data synthesis
Descriptive characteristics and outcomes of included studies were summarised in tables and synthesised primarily in narrative format. Effect sizes (Cohens d) for the difference between adherence and control interventions for adherence outcomes at each time point were calculated using d = (mean 1 - mean 2)/SD pooled (where SD pooled=√[(SD12+SD22)/2]. Effect sizes (d) were interpreted as being small ≤0.20, medium=0.50, large ≥0.80.29 We anticipated there would be limited scope for meta-analyses due to heterogeneity across studies. We did not anticipate included studies would provide sufficient data for subgroup analyses, thus we had no preplanned subgroup analyses. Studies that were sufficiently homogeneous to allow data pooling were analysed using Review Manager (RevMan, V.5.2) statistical software. We considered studies to be clinically homogenous enough to allow pooling when inclusion criteria, interventions, patients and comparators were deemed similar, and comparable outcome measures were used to assess adherence. Pooled continuous data were expressed as standardised mean difference (SMD) with 95% CIs. Significance was set at p<0.05. The random effects model was used for analyses and statistical heterogeneity across pooled studies was quantified using the I2 statistic. Values >50% were considered to represent substantial heterogeneity, and were deemed unsuitable for pooling.30
Following meta-analysis, the strength of the body of evidence was synthesised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.31 The quality of evidence was downgraded from high quality by one level for each of the following criteria: presence of one or more high-risk domains in the Cochrane Risk of Bias assessment, inconsistent (wide CIs) or unexplained heterogeneity of results.31 Indirectness was not relevant to this review as search terms encompassed a specific population, outcomes measures of interest and direct comparisons.
Results
Study selection
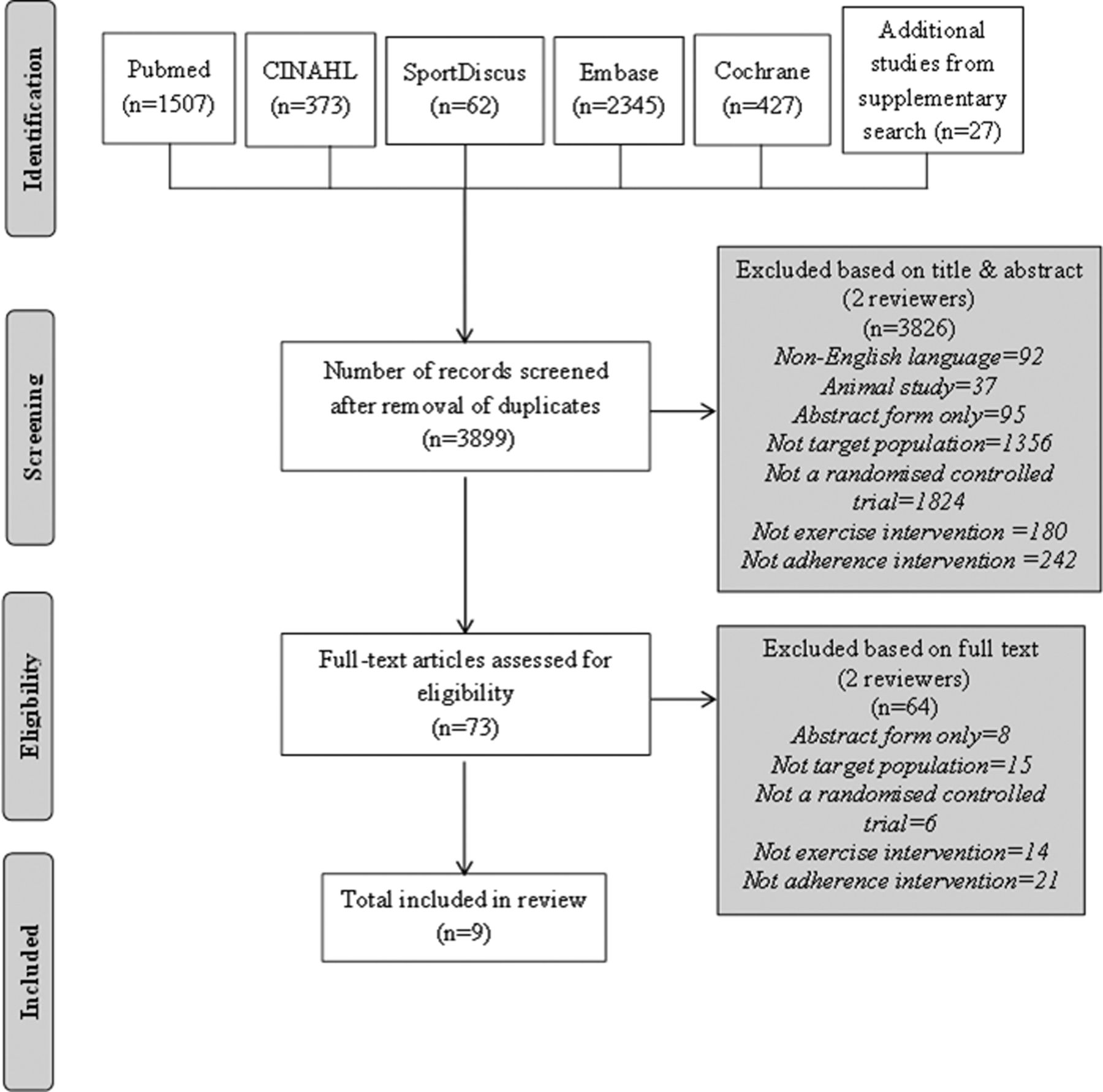
The process of study selection is shown in figure 1. The initial search yielded 4741 references. After removal of duplicates, screening of 3899 titles and abstracts yielded 73 references for full-text review. Of these, the reviewers agreed on inclusion of seven, exclusion of 63 and disagreed about whether three studies should be included (96% absolute agreement, κ=0.80), indicating good agreement between the reviewers.32 Following arbitration by the third reviewer, two articles were included and one excluded. This resulted in a total of nine unique studies, involving 1045 participants, for inclusion in the review.

Flow chart showing selection of studies.
Study characteristics
Descriptive characteristics of the nine included studies are shown in table 1.
Description of included studies
Studies were published between 1998 and 2014, four were conducted in Europe,33–36 three in Australia/New Zealand,37–39 one in Canada40 and one in Hong Kong.41 Three studies recruited older adults with chronic low back pain (total n=339),33 ,34 ,41 three recruited participants with knee osteoarthritis (total n=364)36 ,37 ,40 and three recruited participants with either hip or knee osteoarthritis (total n=342).35 ,38 ,39 Intervention duration ranged from 3 sessions over 8 weeks to 23 sessions over 55 weeks, with follow-up periods ranging from 8 to 65 weeks. A number (n=4, 44%) of studies assessed adherence at short-term (≤3 months) time points only.36 ,38 ,39 ,41 Two studies reported mid-term (3–6 months) follow-up,33 ,37 and three studies reported long-term (≥12 months) outcome measurement.34 ,35 ,40
Significant variation existed in the content of the specific adherence interventions evaluated. Five studies involved complex behavioural interventions with multiple components including education, counselling, positive reinforcement techniques and use of an exercise diary.33–35 ,40 ,41 Two studies included behavioural graded exercise, alone36 or in combination with booster sessions supervised by a clinician.35 One study examined booster sessions supervised by a clinician in isolation,37 one evaluated action coping plans39 and one used an audio or video tape of exercises in addition to verbal instructions of the exercise programme.38
Four studies explicitly referred to the use of behaviour change theory or other conceptual frameworks in developing their intervention.33 ,36 ,40 ,41 Three based their intervention development on the Transtheoretical Model of Behaviour Change,33 ,36 ,41 and one on the Knowledge to Action Cycle conceptual framework for knowledge translation.40
Table 2 describes the outcomes used to measure exercise adherence, including the time points for follow-up and missing data at each time point. A range of data was captured including ratings of overall adherence, time spent exercising, exercise session attendance and number of home sessions completed. The most common was self-reported performance of exercise in logbooks.33 ,34 ,36–38 ,41 Some studies included therapist-reported attendance at exercise sessions.34 ,39 ,40 The number of adherence outcome measures used in each study ranged from one33 ,35 ,36 ,40 ,41 to four.34 Most studies used custom-developed numerical rating scales for self-rating adherence and only one used a specific questionnaire (the Sport Injury Rehabilitation Adherence Scale).42 A number of studies reported considerable amounts of missing data. One study using self-reported logbooks had complete data for only 55% of the original cohort at the 12-month follow-up.34 Another study measuring exercise session attendance reported complete data for only 56% of the original cohort at 12 weeks.39
Effects of adherence intervention on adherence outcomes reported across included studies
Table 3 shows the TIDieR checklist for included studies. Three studies fulfilled all 12 requirements for complete intervention reporting.35 ,37 ,38 Less than half of included studies (n=4, 44%) adequately reported all activities and processes used in the intervention (Item 4). Details of physical and informational materials used in the intervention (Item 3) and details of the intervention provider, including expertise and any specific training given (Item 5) were also poorly described in a number of included studies (n=4, 44% did not fulfil checklist requirements for these items).
TIDieR checklist for reporting of interventions in included studies
Risk of bias assessment
Risk of bias across included studies was scored on 63 items (seven items per study). The two reviewers agreed on the scoring of 58 items (92% absolute agreement, κ=0.85) indicating very good agreement.32 Consensus was reached on disagreements after discussion. Results of the risk of bias assessment are shown in figure 2. All studies had at least one domain judged as unclear risk of bias. The main weaknesses of included studies related to reporting bias, where only one study was rated as being at low risk.37 A number of studies reported prespecified outcomes incompletely, or in a way that excluded inclusion in a meta-analysis. A high risk of performance bias (lack of blinding of participants and personnel) was evident in two studies,33 ,37 and was unclear in three studies.34 ,36 ,38 Four (44%) of the studies were judged to be at low risk of selection bias,33 ,35 ,37 ,40 and four (44%) at low risk of detection bias.35 ,39–41

Risk of bias summary showing review authors' judgments about each risk of bias domain of the Cochrane Risk of Bias Tool.
Effects of interventions
Outcomes regarding the effects of adherence interventions on exercise adherence are presented in table 2. Only two studies (evaluating booster sessions in people with osteoarthritis) were suitable for meta-analysis, as clinical heterogeneity in the other included studies meant no other meta-analyses were considered appropriate.
Chronic low back pain
Two studies involving motivation programmes targeting increasing self-efficacy through positive reinforcement and education reported statistically significant differences between intervention and control group adherence at one or more time point measured.34 ,41 Effect sizes ranged from large (d=1.23) at short-term follow-up41 to small to medium (d=0.44) at long-term follow-up.34 Behavioural counselling, focusing on readiness to change did not improve adherence.33
Hip and/or knee osteoarthritis
One study examining the use of behavioural graded activity in people with knee osteoarthritis36 and one study including a combination of behavioural graded exercise and ‘booster’ sessions in people with hip or knee osteoarthritis35 reported statistically better adherence at one or more time points compared with control. Effect sizes ranged from large (d=0.80) at mid-term follow-up to medium (d=0.53) at long-term follow-up.35 Only one study, examining behavioural graded activity and booster sessions, reported significant differences in exercise adherence with the intervention at all measured time points.35 Among studies that measured adherence at multiple time points in more than one category of short-term, mid-term and long-term, mean raw adherence scores for intervention and control groups decreased from short-term/mid-term to long-term.35 ,40
The four studies that did not find statistically significant benefits of the intervention on adherence compared with control groups included one study evaluating goal setting and strategies to overcome barriers to adherence,40 booster sessions with a physiotherapist,37 action coping plans39 or audio/video exercise performance cues.38
The two studies35 ,37 (229 participants) that evaluated booster sessions were pooled for meta-analysis (figure 3). The pooled effect of these interventions on improving adherence as measured by a self-reported Numeric Rating Scale was small to medium but significant, compared with control groups (SMD 0.39, 95% CI 0.05 to 0.72, z=2.26, p=0.02, I2= 35%). As further research could have an impact on the magnitude and confidence in the estimate of this effect and there is a risk of performance bias in one of the two included studies, the current evidence for this type of intervention was graded as ‘moderate’.31

{kind=link}
{kind=link}
{kind=link}
Forest plot of the mid-term to long-term effect of booster sessions on self-rated adherence assessed using Numeric Rating Scales.
Discussion
This systematic review identified nine unique studies evaluating interventions to increase adherence to therapeutic exercise among older adults with chronic low back pain and/or hip/knee osteoarthritis. Owing to significant heterogeneity across studies, we were only able to conduct a limited meta-analysis. We found moderate-quality evidence that incorporating booster sessions with a physiotherapist may improve therapeutic exercise adherence in people with osteoarthritis. We also found emerging evidence from individual high-quality studies that interventions specifically targeting patient motivation to exercise, or adopting a behavioural graded exercise approach may improve therapeutic exercise adherence in people with chronic low back pain and osteoarthritis, respectively. However, effect sizes declined to medium (at best) over the long term. Results of this systematic review and limited meta-analysis suggest that behavioural counselling, use of action coping plans or audio/video exercise performance cues are ineffective at improving exercise adherence in these patient groups.
In contrast to previous systematic reviews,22 ,23 which included studies that could not isolate the specific effects of the adherence strategy under investigation, our review included only studies with contextual equivalence between control and target interventions. Despite this, our findings are largely consistent with those of previous reviews. In people with osteoarthritis and rheumatoid arthritis, Ezzat et al23 included 19 studies, of which 13 involved participants with osteoarthritis. They did not perform a meta-analysis and concluded there was limited evidence that interventions can improve exercise adherence. Of the 42 studies included in the 2010 Cochrane review22 of interventions to improve adherence to exercise for chronic musculoskeletal pain in adults, all but two included people with osteoarthritis and spinal pain. Although the authors concluded that supervised or individualised exercise therapy may enhance exercise adherence, this conclusion is questionable given the lack of contextual equivalence between control and intervention arms of the included RCTs.
Our review highlighted some potential strategies that may be effective for increasing exercise adherence and warrant further research. Techniques specifically aimed at increasing patient motivation to exercise appear promising for people with chronic low back pain, based on the positive findings of two individual moderate-high-quality studies.34 ,41 These techniques include positive feedback and reinforcement of patient efforts, advice about posting self-reminders at home to complete exercises, the use of an exercise diary and the use of a ‘treatment contract’. Patient motivation to exercise is critical for sustained exercise adherence,43 and a systematic review of individual and intervention-related factors associated with adherence to home exercise among people with chronic low back pain found incorporating motivational strategies in interventions was associated with increased adherence.44
Another intervention with promise is behavioural graded exercise for people with hip or knee osteoarthritis. Behavioural graded exercise uses principles of operant conditioning and self-regulation, and is directed at gradually increasing intensity of exercise and integration of exercises into daily living.35 ,36 ,45 Lack of confidence in capability to exercise, lack of time and inability to accommodate exercises in daily life have been recognised as significant barriers to exercise participation among people with knee osteoarthritis.16 ,46 ,47 The use of behavioural graded exercise addresses these barriers directly.
Pooled analysis found moderate-quality evidence for booster sessions improving mid-long-term exercise adherence in people with osteoarthritis. Booster sessions involve returning to a therapist after an initial period of exercise treatment. Content of these sessions may vary. In the two included studies, these sessions focused on review and progression of the home exercise programme and discussion of progress and barriers to exercise adherence.35 ,37 The use of such sessions provides ongoing contact and reinforcement, both of which are recognised as facilitators to exercise adherence in this population.16
Given the vast array of factors known to influence exercise adherence in people with chronic low back pain and/or osteoarthritis, no single strategy will be effective in overcoming all barriers to exercise participation in all people, all of the time.16 ,18 ,20 ,44 ,48 For interventions to effectively facilitate behaviour change, the use of theoretical rationale is imperative when designing interventions.49 Medical Research Council guidelines recommend including theory within complex intervention study designs;50 however, only four studies in this systematic review explicitly referred to the use of behaviour change theory or other conceptual frameworks in developing their intervention.33 ,36 ,40 ,41
Furthermore, it is likely that multifaceted adherence interventions, that contain multiple behaviour change techniques and address multiple barriers to exercise participation, are required. Previous literature has suggested that complex interventions containing multiple concurrently delivered strategies can improve adherence to exercise more than a single-strategy intervention among wider chronic disease populations.51 Alternate to multifaceted adherence interventions is an individualised targeted approach to promoting exercise adherence, whereby the unique barriers to exercise participation are established for each patient and a targeted interventional strategy is developed collaboratively between the clinician and patient in order to increase exercise adherence.52 Although an intervention of targeted exercise adherence is promising for improving adherence for longer periods in older adults with knee pain, results to date have been published as conference abstracts only, preventing inclusion in this review.53 ,54
Strengths and limitations
This review advances previous systematic reviews in comparable populations.22 ,23 Although our review included fewer eligible studies, those that were reviewed demonstrated acceptable contextual equivalence between intervention and control groups, allowing us to determine whether interventions increase adherence more accurately than previous systematic reviews. We conducted an extensive database review; however, it is possible that articles were missed during the search due to publication and selective reporting biases, presenting a potential limitation. In addition, our ability to pool data was limited due to the heterogeneity in interventions and outcomes identified.
It is possible that effectiveness of booster sessions, and indeed other interventions designed to increase adherence, may be influenced by factors such as comorbidities, age of the patient, cognitive capability and location of intervention delivery; however, this has not yet been explored to date.
Improved reporting of interventions is required. Interventions in many of the included studies in this review were poorly described, particularly with respect to physical or informational materials used in the intervention. These deficiencies in reporting preclude clinicians and researchers from reliably replicating or implementing interventions. Previous literature has found this to be common among interventions designed to change behaviour55 ,56 and, as a result, the Behaviour Change Technique Taxonomy was developed to provide a clear and replicable method of coding the components of any behaviour change intervention.57 In addition, the recently published Consensus on Exercise Reporting Template (CERT) was developed to provide guidance specifically in reporting exercise programmes.58 Future RCTs should consider using these in addition to the TIDieR checklist,27 in developing and reporting intervention content.
Finally, the heterogeneity in outcomes used to measure exercise adherence remains an issue, and limited our ability to pool data in this review. This has been previously acknowledged as a limitation to advancing research in this field.59 A recent systematic review of measures of self-reported adherence to home exercise programmes concluded there is no gold standard measure.60 Psychometric evaluation of commonly used self-reported measures of exercise adherence, and development of a validated standard outcome measure for adherence, should be a research priority.
Conclusion
In conclusion, this systematic review identified a small number of RCTs that evaluated whether interventions aimed at increasing adherence to therapeutic exercise increased adherence among older adults with chronic low back pain and/or hip/knee osteoarthritis. Meta-analysis provides moderate-quality evidence for booster sessions with a physiotherapist improving patient adherence to therapeutic exercise in people with osteoarthritis. Individual high-quality trials provide emerging evidence to support the use of patient motivational strategies and behavioural graded exercise to improve adherence to exercise in people with chronic low back pain and osteoarthritis. However, effect sizes for these interventions declined over time, to medium at best long term.
What are the findings?
The benefits of exercise for older adults with chronic low back pain and hip/knee osteoarthritis are well established.
Adherence to exercise programmes is important to optimise clinical benefits, and strategies to enhance exercise adherence have been evaluated in clinical trials.
Previous systematic reviews of the effectiveness of interventions for improving exercise adherence were hampered by a lack of contextual equivalence between control and intervention groups.
How might it impact on clinical practice in the future?
Meta-analysis of two studies provides moderate-quality evidence that booster sessions with a physiotherapist may improve adherence to exercise in people with hip/knee osteoarthritis.
Individual clinical trials provide emerging evidence to support the use of patient motivational strategies in people with chronic low back pain and behavioural graded exercise in people with osteoarthritis to improve adherence to exercise.
Accurate reporting of intervention components and development of a standard, validated measure of exercise adherence are urgent research priorities in order to progress this field of research.
References
Footnotes
Contributors All authors were involved in study concept and design. PJAN and FLD performed the literature search. PJAN, AVG and MHA screened articles for eligibility. PJAN, AVG and FLD evaluated the quality of included articles. PJAN wrote the first draft of this article. All authors revised the paper and provided scientific input. All authors approved the final manuscript. RSH is the guarantor (the contributor who accepts full responsibility for the finished article, had access to all data and controlled the decision to publish).
Funding PJAN is supported by a PhD stipend from the Medibank Health Research Fund. KLB is supported by an NHMRC Principal Research Fellowship (#1058440). RSH is supported by an Australian Research Council Future Fellowship (FT130100175). AVG is supported by an NHMRC programme grant (#061887). MAH is supported by the National Institute for Health Research (NIHR) School for Primary Care Research.
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the National Health Service, the NIHR or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.