Article Text

Abstract
Objective To evaluate the efficacy of a home-based exercise programme added to usual medical care for the treatment of depression.
Design Prospective, two group parallel, randomised controlled study.
Setting Community-based.
Patients 200 adults aged 50 years or older deemed to be currently suffering from a clinical depressive illness and under the care of a general practitioner.
Interventions Participants were randomly allocated to either usual medical care alone (control) or usual medical care plus physical activity (intervention). The intervention consisted of a 12-week home-based programme to promote physical activity at a level that meets recently published guidelines for exercise in people aged 65 years or over.
Main outcome measurements Severity of depression was measured with the structured interview guide for the Montgomery-Asberg Depression Rating Scale (SIGMA), and depression status was assessed with the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I).
Results Remission of depressive illness was similar in both the usual care (59%) and exercise groups (63%; OR = 1.18, 95% CI 0.61 to 2.30) at the end of the 12-week intervention, and again at the 52-week follow-up (67% vs 68%) (OR=1.07, 95% CI 0.56 to 2.02). There was no change in objective measures of fitness over the 12-week intervention among the exercise group.
Conclusions This home-based physical activity intervention failed to enhance fitness and did not ameliorate depressive symptoms in older adults, possibly due to a lack of ongoing supervision to ensure compliance and optimal engagement.
- Exercise
- Exercise rehabilitation
- Intervention efficacy
- Physical activity promotion in primary care
- Aging
Statistics from Altmetric.com
- Exercise
- Exercise rehabilitation
- Intervention efficacy
- Physical activity promotion in primary care
- Aging
Introduction
Depression is common among people aged 60 years and older, and is associated with a reduction in quality of life, as well as increased physical disability, service utilisation (particularly readmission to hospital) and mortality.1 ,2 Although antidepressant medication is often the primary treatment for depression in older adults,3 ,4 there are risks associated with its use among this age group,5–9 and half fail to achieve symptom remission.10 ,11 Those failing to respond to treatment can be left with ongoing depressive illness, placing their general health and well-being in jeopardy.12 ,13 With most adults aged 65 years and older suffering from at least one chronic medical condition,14 treatments that reduce the burden on healthcare systems and remove the deleterious effects of polypharmacy are needed to ameliorate depression in older adults.
Evidence derived from observational studies of community-representative samples of older adults shows that depression is less prevalent among people who exercise regularly,15–17 while the antidepressant effect of physical activity is comparable to that found for medication or psychotherapy,18 with efficacy found for both aerobic19 ,20 and resistance modes of exercise21–23 in a series of randomised trials. Importantly, the mental health benefits of these exercise interventions appeared to last beyond the acute treatment phase,22 ,24 with relapse of depression less frequent compared with participants receiving antidepressant medication alone.25 While the results of such studies are encouraging, these interventions tend to be clinic-based or laboratory-based, leaving questions about their transferability and sustainability in home environments.
We report data from a community-based randomised clinical trial of an intervention designed to increase the level of physical activity among adults aged 50 years and older who were depressed and under the medical care of a general practitioner (GP). Our primary outcomes of interest were the proportion of individuals who achieved a 50% or greater reduction in depressive symptoms, and/or a remission of their illness, among those who received standard primary healthcare compared with those who received a home-based exercise programme in addition to their usual medical treatment. To further assess the impact of the exercise intervention, we examined the relationship between changes in markers of physical fitness (ie, cardiorespiratory capacity, calories spent per week in moderate–high intensity activities, body mass, lower limb strength) from baseline to postintervention and the reduction of depressive symptomatology.
Methods
Study population
The study population consisted of 200 adults aged 50 years or older deemed to be currently suffering from a clinical depressive illness during a standardised mental health telephone assessment with project staff. A project information sheet, consent form and screening questionnaire was posted to a random Australian Electoral Commission sample of 59 260 individuals aged 50 years and older and residing in the Perth-metropolitan region of Western Australia between September and December 2010. Of the 7346 returned questionnaires (12.4% response rate), those with a score of 10 or more on the Patient Health Questionnaire (PHQ-9),26 which was embedded within the postal screening questionnaire, were contacted by project staff (Doctoral and Master's Degree-level psychologists) to conduct a formal assessment of their depressive symptomatology—with the Structured Clinical Interview for DSM-IV Axis I Disorders—Research Version (SCID-I-RV).27 All research psychologists were trained and supervised in the use of SCID and SIGMA by an experienced registered clinical psychologist, with each baseline assessment reviewed to ensure consistency of the evaluation protocol. Participants meeting the criteria for a Major Depressive Episode or Minor Depressive Illness were invited to participate in the study and a medical consultation was arranged with their GP to initiate treatment. Minor depression was defined as follows: at least two, but less than five, of the symptoms of a Major Depressive Episode during the same 2-week period that represents a change from previous functioning; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure—SCID-I-RV Module J. Each participant's GP was informed of their patient's involvement in the study, as well as their current depressive status based on the SCID-I assessment, and requested that—If this is a previously untreated illness, we would be grateful if you could initiate a treatment plan for this patient—managing the patient's depressive symptoms with your usual clinical practice. Individuals meeting the depression criteria were excluded from the study if they reported suicide intent, delusions or hallucinations, concurrent alcohol or substance abuse or dependency, a medical condition or locomotion difficulties that would preclude participation in a physical activity programme, or if they were not fluent in written or spoken English (figure 1).
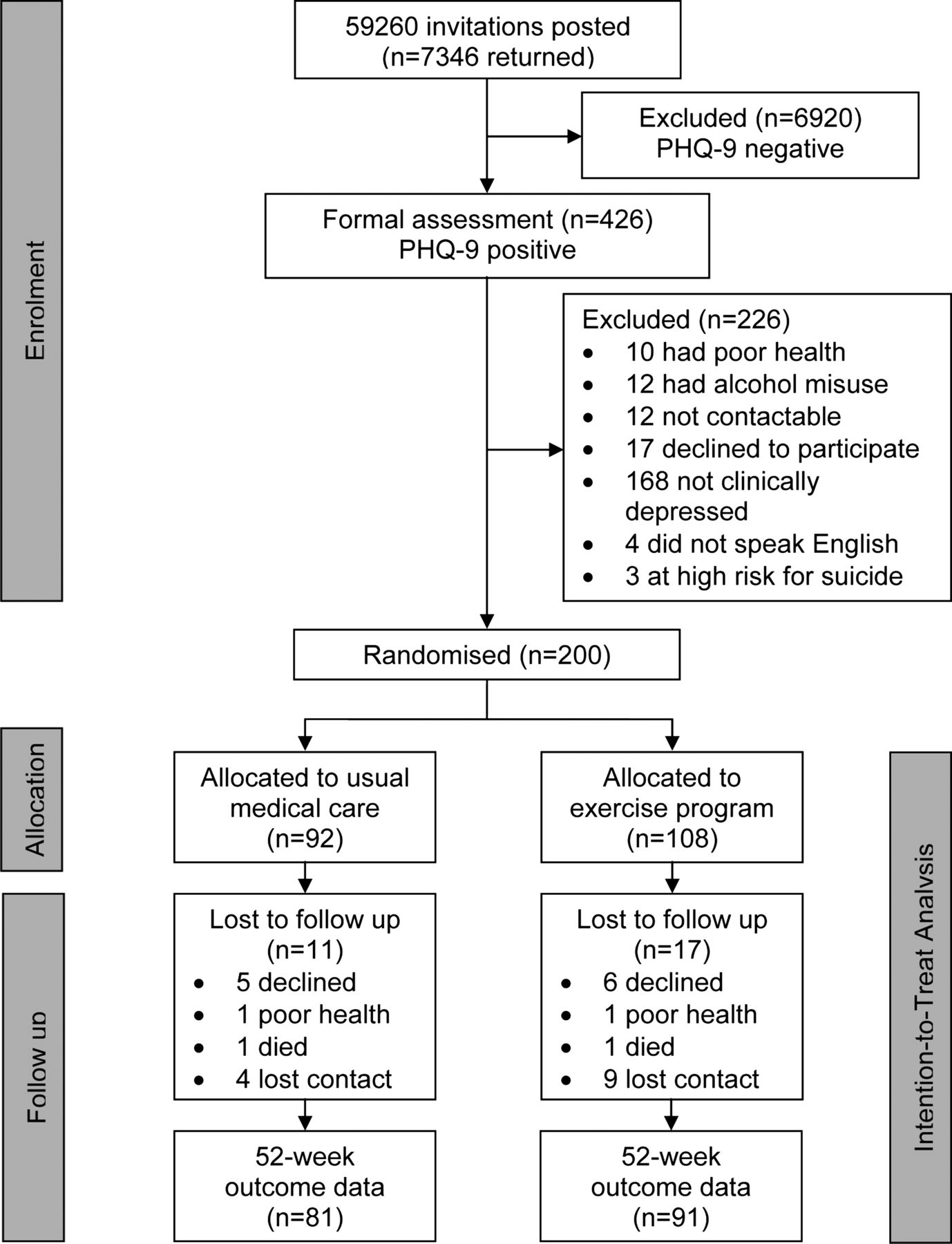
Flow of study participants from enrolment until the final collection of primary outcomes at 52 weeks.
Intervention
Participants were randomly allocated to either usual medical care (control) or medical care and physical activity (intervention), based on permuted block randomisation conducted by an independent researcher not in direct contact with participants. Blocks varied in size from 4 to 10 participants and the random list of numbers was computer generated. All participants were assessed for ongoing depression status via telephone by project psychologists at baseline (original telephone assessment for PHQ-9 positive individuals), and then at 4, 8, 12, 26 and 52 weeks following group allocation. Those conducting the telephone mental-health assessments were blind to treatment group allocation status. Contact details of participants randomised to the intervention group were provided to the study's exercise physiologist on a weekly basis. Telephone contact was made to arrange a home visit to conduct a preintervention physiological assessment and assign the 12-week individualised exercise programme for the participant. Booster telephone calls were made by the exercise physiologist at weeks 4 and 8 to review progress and facilitate compliance with the programme, followed by another home visit at week 12 to complete the postintervention physiological measures.
The aim of the exercise programme was to promote physical activity at a level that meets the recently published guidelines of the American College of Sports Medicine and American Heart Association for exercise in people aged over 65 years.28 Guidelines are to complete aerobic (cardiorespiratory) activity of moderate intensity at least 5 days/week or of vigorous intensity a minimum of 3 days/week. Target duration is to accumulate at least 30 min/day of moderate-intensity activity, in bouts of at least 10 min each or continuous vigorous activity for at least 20 min/day. In addition, resistance exercise should be performed at least 2 days/week of 8–10 exercises involving the major muscle groups for 10–15 repetitions. Resistance exercise was performed using available home resources and provision of relatively inexpensive and portable equipment such as Theraband, dumbbells, Swiss Balls, Gymsticks and ankle cuff weights. Resistance exercises targeted the major lower and upper body muscle groups as well as trunk flexors and extensors. Intensity was prescribed at 10 RM (resistance that limits the number of movements to 10 per set), which is the higher end of the ACSM/AHA guidelines based on the findings of Singh et al.23 In order to provide progressive resistance training, participants were instructed to increase the resistance for the next set or session once they could complete more than 10 repetitions at that load. This was monitored and reinforced at each of the booster telephone calls. At baseline, each participant was provided with a booklet of printed diagrammatic exercises and accompanying explanations for each, and a log book to describe the frequency, duration and type of exercise (resistance or aerobic), as well as a rating of perceived exertion (RPE; using a supplied Borg Scale for RPE). These were reviewed at each contact point and alterations made to the programme based on aerobic capacity and strength gains.
Participants were asked to perform resistance exercises at home three times per week, resulting in 36 exposures for those fully compliant with the programme. Participants were also encouraged to engage in a minimum of 150 min of aerobic exercise per week (usually 30 min/day over 5 days) in activities such as swimming, walking and cycling. Participants who preferred doing their aerobic exercise at home were provided with an exercise step. Warm-up, cool down and stretching were explained to the participants and encouraged for each exercise session. The intervention protocol is available online as supplementary material.
The study procedures followed the guidelines of Helsinki for Human Rights and the protocol was approved by the Human Research Ethics Committee of the University of Western Australia (RA/4/1/2233). The study was registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12609000150246).
Primary variables
Fifty per cent reduction in depressive symptomatology
We used the structured interview guide for the Montgomery-Asberg Depression Rating Scale (SIGMA)29 to measure the severity of depressive symptoms. MADRS is widely used in clinical trials of depression because its items have been shown to be sensitive to change with antidepressant treatment. Use of SIGMA can result in high reliability of MADRS scores in evaluating individuals with depression and has been shown to have good to excellent inter-rater reliability across all 10 of the MADRS items.29 SIGMA was administered at baseline and weeks 4, 8, 12, 26 and 52 of the study.
Remission of symptoms (no longer meeting the criteria for major and minor depression)
SCID-I is a semistructured interview used to make major DSM-IV Axis I diagnoses; it possesses high inter-rater reliability across diagnostic groups.27 The SCID interview is considered the gold standard in the assessment of depression and is widely used in depression intervention trials. Postgraduate-level research psychologists utilised the SCID module for current major depressive disorder to assess symptoms of depression, including mood disturbance, psychomotor disturbances, low energy level, low self-esteem, low cognitive functioning, suicidal ideation, functional impairment, grief and health-related complications. SCID was administered at baseline and weeks 12, 26 and 52.
Secondary variables
Change in level of physical activity
The Community Healthy Activities Model Program for Seniors (CHAMPS) questionnaire30 was used to assess physical activity level and has been shown to have acceptable validity, reliability and sensitivity to change in older adults.31 ,32 CHAMPS is designed to assess the weekly frequency and duration of activities typically undertaken by older adults. Activities listed in CHAMPS were assigned a metabolic equivalent value specific for older adults, as defined by Stewart et al,30 that enables coding and classification of activities by rate of energy expenditure. Outcome measures from CHAMPS utilised in this study included caloric expenditure per week and frequency per week for moderate–high intensity activities. CHAMPS was administered by the exercise physiologist during the preintervention home-based assessment, and again at the end of the 12-week activity period for intervention participants.
Change in physiological measures
The exercise physiologist assessed two aspects of physical function among intervention participants during the preintervention and 12-week home visits. Timed Chair Stand is a simple functional strength measure for lower limbs. Performance is assessed as the number of times the participant can stand up and sit down as quickly as possible within 30 s, without pushing up using the arms. Cardiorespiratory Capacity was assessed using a standard step test designed for older adults, in which heart rate is recorded electronically. Maximum aerobic power was calculated based on the linear relationship between heart rate and work rate and assuming a maximum heart rate of 220 minus age. Oxygen uptake at maximum aerobic power was estimated using standard calculations33 and expressed as an absolute measure, as well as relative to body mass.
Other study measures
In addition to PHQ-9, a number of other variables were collected from all participants on the postal screening questionnaire. Participants provided information about their gender, place of birth (Australia vs overseas), marital status, current living arrangements, highest educational achievement and age. We also asked them how often they engaged in moderate–high intensity activities during the past week, whether they smoked, and if they engaged in harmful drinking (a score of eight or more on the alcohol use disorders identification test.34 We used self-reported height and weight to calculate the body mass index (BMI), and classified as overweight or obese participants with a BMI of 25 kg/m2 or above. Participants also recorded whether a doctor had ever told them they had an anxiety disorder or depression (yes/no), age at first diagnosis of depression and the number of GP visits over the past year. Finally, we asked participants to record the names of any prescribed medications they were currently taking, and from this list we retrieved information about the use of antidepressants (any class).
Sample size calculation
We estimated that, with 100 participants in each group, the study would have 77% power (two-tailed α=5%) to declare as significant a difference of 20% or more between the groups. We had originally planned to recruit 300 participants to ensure greater power for the study, but that was not possible within the time and budgetary constraints of the study.
Statistical analysis
We used cross-tabulations and independent samples t tests to determine the distribution of potential confounders according to the allocation group (control or intervention). We applied imputation by chain equations to complete an intention-to-treat analysis. All variables available at baseline (table 1) plus SCID and SIGMA scores at baseline and weeks 12, 26 and 52 contributed information to calculate the missing values for the imputation files. We produced five imputed datasets to achieve stable estimates and 95% CIs. To examine the effect of the intervention, we conducted a split-plot analysis of variance (ANOVA) comparing the mean difference of SIGMA scores during the four assessment phases of the study (at baseline and at 12, 26 and 52 weeks). Using this technique, the effect of the intervention was determined by the interaction of group allocation over time, as well as the effect of these variables independently.
Background characteristics at study entry
We then compared the proportions of people who reduced their SIGMA score by at least 50% at the end of the intervention (12 weeks), and at the 26-week and 52-week follow-up assessments. We also analysed remission of major or minor depression, as measured by the SCID, at these same time points. We used logistic regression to estimate the association between the allocation group and each of these outcomes, and report ORs with 95% CIs.
To examine the impact of fitness improvement on depressive symptomatology, we used Pearson product-moment correlations to explore the relationship between change in SIGMA scores at week 12 and the measured difference in exercise participants’ pre–post fitness markers (ie, best timed chair rise, body mass, caloric expenditure per week for moderate–high intensity activities and maximum oxygen uptake). Finally, we looked at the effectiveness of our home-based exercise intervention, using paired samples t tests to determine the degree of change in fitness levels within the exercise group from baseline to the completion of the 12-week programme. The data were managed and analysed with SPSS, V.20 (IBM Corp). Statistical significance was set at 0.05, and all statistical tests reported are two-tailed.
Results
Two hundred participants were enrolled in the study following confirmation of their depression status during the prestudy telephone assessment. There were no statistically significant differences between the two study groups at the point of randomisation, although a non-significant higher proportion of exercise participants were using antidepressant medication (table 1). Following the randomisation phase, a greater number of participants in the exercise intervention (27.8%) compared with the usual care group (14.1%) dropped out of the study by the 12-week assessment (OR=2.34, 95% CI 1.14 to 4.81). Current antidepressant medication use was the only baseline variable that differentiated those who dropped out (39.5%) during the first 12 weeks of the study from those who continued to participate (58.6%) (OR=0.46, 95% CI 0.23 to 0.92). At the 52-week assessment point, those who earlier withdrew from the study were recontacted to collect data on our primary endpoints at the end of the study. This narrowed the proportion of missing depression status data between the usual care group (12.0%) and the exercise participants group (15.7%) at the final follow-up (OR=1.38, 95% CI 0.61 to 3.11).
A split-plot ANOVA was conducted to explore the impact of the interventions on SIGMA scores across the four assessment periods of the study. While there was a significant main effect for time, with participants manifesting a reduction in depressive symptomatology over the course of the study (Wilks’ Lambda=0.631, F(3, 196)=38.41, p<0.001, η2=0.168), this improvement was not due to treatment group allocation (F(1, 198)=0.077, p=0.846) or an interaction between the two (group×time; F(3, 196)=1.394, p=0.280; figure 2).

{kind=link}
{kind=link}
Intention-to-treat analysis of mean SIGMA scores by group across assessment points of the study.
A perprotocol examination of substantial reduction in depressive symptomatology (≥50% lower SIGMA score), or remission of depressive disorder (SCID) from baseline levels, revealed no difference between those in the exercise intervention and participants receiving usual care across the assessment periods (table 2). To explore the influence of antidepressant use on these results, a one-way between-groups analysis of covariance was conducted to compare the effectiveness of the two interventions on the change in SIGMA scores between baseline and week 52, using the number of weeks of antidepressant use during the study as a covariate in this analysis. After adjusting for antidepressant use, there continued to be no difference between the exercise intervention and usual care groups regarding the difference in depressive symptomatology at the end of the study (F(1, 156)=0.098, p=0.754, η2<0.001). There was also no relationship between the number of weeks of antidepressant use and participants’ end of study change in depression scores, independent of group allocation, as indicated by an η2 value of 0.001.
Depressive severity (SIGMA) and diagnostic status (SCID-I) between per-protocol study groups at weeks 12, 26 and 52
During the intervention, participants completed an average of 21 (SD=12) of the 36 total possible prescribed exercise sessions, at a mean intensity level of 4.8 RPE (SD=1.4). We conducted a series of correlation analyses to explore the relationship between the difference in baseline and 12-week fitness markers with the change in SIGMA scores during this same time period among exercise participants. We found no relationship between the difference in caloric expenditure during moderate–high intensity physical activities (CHAMPS) from baseline to postintervention and change in depressive symptomatology (SIGMA; r=−0.115, n=78, p=0.318). Similarly, we found no relationship between SIGMA score differences and chair rise improvement (ie, functional strength; r=0.098, n=63, p=0.446), predicted maximum oxygen uptake relative to body mass (ie, cardiorespiratory capacity; r=0.138, n=56, p=0.311), or change in body mass (r=0.088, n=59, p=0.506). Overall, the home-based exercise programme failed to result in enhanced physical performance across the intervention group, with the only significant change relating to deterioration in functional strength (ie, timed chair rise) at the end of the 12-week period (table 3).
Mean physiological scores among exercise participants at baseline and on completion of the 12-week physical activity programme
Discussion
Our goal was to test the transferability of laboratory or gym-based exercise interventions for depression in older adults to the community. In particular, we tested whether or not the addition of a personalised home-based exercise programme designed by an exercise physiologist would enhance usual primary healthcare in alleviating the symptoms and incidence of depressive disorders in adults aged 50 years and older. We found no difference between the two groups concerning remission of depressive illness or a 50% or greater reduction in depressive symptomatology at any time point in the study. Between 59% and 68% of participants in both groups were deemed free of depressive illness across the 12-week, 26-week and 52-week follow-up assessments.
Two issues are worth noting. The first is that a large proportion of participants experienced remission of their depressive status over the course of the study in both groups. Uncontrolled studies of physical activity have found that this intervention is associated with remission of depressive symptoms. This study demonstrates why the inclusion of a control group is crucial as depressive symptoms may remit with time, regardless of treatment.35 With such high rates of spontaneous remission among community-dwelling adults, it would be difficult for any intervention, let alone physical activity, to demonstrate better recovery rates. Blumenthal et al36 have noted that a large proportion of the therapeutic response is influenced by patient expectations, ongoing symptom monitoring, attention and other factors. Thus, we cannot rule out the fact that our repeated contact and monitoring of participants’ depressive status in both groups resulted in an unintended global therapeutic response, diminishing our ability to detect a difference between the interventions. Although our study is one of the largest single site exercise interventions among individuals with a structured clinical diagnosis of depression,37 the similar response rate between our groups left the study underpowered to declare as significant small differences between the intervention groups. A larger sample size, however, would not provide any further clinical significance to our findings, as such treatment outcomes argue against recommending home-based exercise as a cost-effective adjunctive therapy for depression in primary care settings.
While medication is often the primary treatment for depression in older adults, antidepressants have been shown to lessen the long-term benefits of exercise.25 It seems possible that the use of antidepressants may have limited the effectiveness of our intervention, as a borderline non-significant higher proportion of participants assigned to the physical activity group were taking antidepressants at study entry, while a greater number of those who dropped out were not using these medications. However, the lack of relationship between antidepressant use and our primary outcome measures does not support this interpretation. Instead, the more pertinent issue appears to involve the effectiveness of the exercise intervention itself and the lack of physiological change among participants across the 12 weeks of the study. In particular, the intervention group failed to show a positive change in cardiorespiratory capacity, body mass or lower limb strength from baseline levels, even though the self-reported weekly frequency of moderate–high intensity activities was higher. While there is evidence that exercise frequency38 ,39 and intensity23 ,40 have a positive impact on mood, our results indicate that there is inconsistency in participants’ self-perception of these factors with regard to the activities they are engaged in. In fact, our participants’ training logs highlighted low compliance and suboptimal energy expenditure—two factors that would contribute to the lack of improvement in physiological capacities. Kerse et al41 compared the effectiveness of a home-based physical activity programme with social visits in alleviating depression among older adults, and similarly found that those in the exercise programme reported engaging in more physical activity (ie, walking) but demonstrated no change in physical functioning over the 12-month study period, resulting in no difference between the two community-based intervention groups. Indeed, others have found that self-reported estimates of physical activity among adults were six times greater than their actual activity recorded by an accelerometer,42 reinforcing the need for objective measures of exercise adherence during community-based studies.
A limitation of our study was our inability to monitor our participants’ exercise activity over the 12 weeks of the intervention. This inhibited us from determining both the true intensity of the activities that participants were engaging in, as well as their compliance with the programme between the baseline and postintervention home visits. As a result, our home-based intervention with minimal supervision did not enable this population to exercise at the required intensity or with sufficient frequency to produce meaningful benefits. Considering that unsupervised depressed patients may fail to maintain their motivation to carry out prescribed physical activities43 compared with those engaged in more active supervision,36 ,44 this would seem to be a necessary component for future community-based interventions.
By its very definition, depression represents a lack of movement towards anything, so most patients are inactive to begin with, which can explain why approximately half the participants in exercise and depression studies drop out.45 In addition to depression, our participants possessed an average of over three chronic medical conditions at study entry. Ill health has often been cited among older adults as a barrier to physical activity.46 ,47 For older adults with a sedentary lifestyle as well as declining physical resources, the sense of being able to master a physical exercise programme could be challenging. Self-efficacy has been considered as one of the major motivational factors in both initial commitment and long-term maintenance of lifestyle modification.48 Therefore, a potential weakness of our intervention was a lack of ongoing motivational work with a participant group of adults who, by the very nature of their illness, experience lower levels of this attribute. The inclusion of problem solving, goal setting and other active coping strategies has been recommended to increase and maintain the exercise of depressed patients.49
A further limitation of our study was the lack of information we obtained about exercise and fitness levels in the usual care medical group over the course of the study. Previous physical activity interventions have reported an unexpected increase in exercise or fitness in the control group,50 and our failure to collect objective measures of fitness within the medical care only group limits our ability to rule out a Hawthorne effect among these participants,51 whereby they may have independently changed their activity levels due to being involved in a physical activity study. However, when one considers the similarity between the two intervention groups at study entry and the lack of change in fitness levels among those who received a personalised exercise programme, it would seem unlikely that those in the usual care group would have spontaneously engaged in a sustained lifestyle change (ie, regular physical activity) that would have had an impact on our primary outcomes.
We sought to enhance the treatment of depression in community-dwelling middle-aged and older adults by adding a 12-week personalised home-based exercise programme to their treatment regime. This failed to show any benefit over the usual general practice care for depression, primarily due to the high rate of remission of symptoms and the lack of change in fitness levels among those in the exercise group. Structured centre-based programmes can control and supervise the amount and quality of physical activities that participants engage in, and have been previously shown to lead to greater health gains compared with a home-based intervention for older adults.52 However, they can be prohibitively expensive and inconvenient for older adults to get to, thereby limiting their implementation possibilities. Based on the findings of our study, future community-based exercise interventions for depression should seek to incorporate personalised elements (eg, motivational interviewing, goal setting) into the treatment regime to enhance participants’ self-efficacy and ongoing participation, and ensure that objective measures of fitness are taken on a regular basis by qualified professionals so that exercise targets and physiological change are achieved.
What are the new findings?
-
Remission of symptoms is common among depressed older primary care patients, regardless of treatment.
-
Exercise may not be a cost-effective adjuvant therapy for depression in primary care settings.
How might it impact on clinical practice in the near future?
-
Ongoing supervision and objective measures of fitness are required to ensure compliance with community-based exercise interventions for depressed patients.
-
Incorporating a motivational component into exercise interventions for depression may be needed to enhance participation rates.
Acknowledgments
The investigators would like to thank all participants and research staff for their generous contribution. Special thanks to Dr Kylie Marsh and Courtney White for coordinating the respective mental health and fitness assessments.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online ActiveDep
Footnotes
-
Contributors JJP, OPA, RUN, MS and LF conceived and designed the study. JJP, OPA and RUN acquired the data. JJP had full access to all data and takes responsibility for the integrity of the data and the accuracy of the data analysis. JJP and HA performed all analyses and drafted the paper, which was critically revised by all the authors for important intellectual content.
-
Funding This study was supported by the project grant number 18037 from Healthway (the Western Australian Health Promotion Foundation). JJP is funded by a postdoctoral medical research fellowship from the Medical Research Foundation, Royal Perth Hospital.
-
Competing interests None.
-
Ethics approval Human Research Ethics Committee of the University of Western Australia (RA/4/1/2233).
-
Provenance and peer review Not commissioned; externally peer reviewed.