Article Text

Abstract
Background Voluntary lumbopelvic control is compromised in patients with back pain. Loss of proprioceptive acuity is one contributor to decreased control. Several reasons for decreased proprioceptive acuity have been proposed, but the integrity of cortical body maps has been overlooked. We investigated whether tactile acuity, a clear clinical signature of primary sensory cortex organisation, relates to lumbopelvic control in people with back pain.
Methods Forty-five patients with back pain and 45 age- and sex-matched healthy controls participated in this cross-sectional study. Tactile acuity at the back was assessed using two-point discrimination (TPD) threshold in vertical and horizontal directions. Voluntary motor control was assessed using an established battery of clinical tests.
Results Patients performed worse on the voluntary lumbopelvic tasks than healthy controls did (p<0.001). TPD threshold was larger in patients (mean (SD)=61 (13) mm) than in healthy controls (44 (10) mm). Moreover, larger TPD threshold was positively related to worse performance on the voluntary lumbopelvic tasks (Pearson's r=0.49; p<0.001).
Discussion Tactile acuity, a clear clinical signature of primary sensory cortex organisation, relates to voluntary lumbopelvic control. This relationship raises the possibility that the former contributes to the latter, in which case training tactile acuity may aid recovery and assist in achieving normal motor performance after back injury.
Statistics from Altmetric.com
Two goals of rehabilitation after injury are resolution of symptoms and return to normal motor/behavioural function. Resolution of pain is a relatively clear endpoint, but resolution of motor/behavioural function is not—myriad factors can contribute to motor dysfunction after an initial episode of pain and most people are not aware that they are moving differently (see the work of Hodges and Moseley1 for a review). One contributor to motor dysfunction is a loss of proprioceptive acuity.2,–,4 Although attention has been focussed on disruption of proprioceptive input peripherally or within the spinal cord,5 proprioceptive acuity also depends on intact cortical proprioceptive maps. One such map is the representation of the surfaces of the body, held in the primary sensory cortex (S1). In patients with back pain, the representation of the back in S1 is shifted by about 2 cm,6 or several hundred thousand neurons (several trillion synapses). In patients with phantom limb pain or complex regional pain syndrome, a clear clinical signature of altered S1 representation is increased two-point discrimination (TPD) threshold.7 8 This is not surprising because both S1 representation and TPD depend on inhibitory mechanisms within S1.9
We recently observed, in a convenience sample of back-pain patients, that increased TPD threshold coincided with the area of their pain and disruption of their body image.10 TPD elsewere on the back was normal. However, whether increased TPD threshold is characteristic of back-pain patients in general remains to be determined. Further, although there is good evidence that back-pain patients find simple movements of the back and pelvis difficult,4 11 whether this relates to TPD threshold at the back has not been investigated. This study aimed to determine the relationship between back pain, TPD threshold at the back and lumbopelvic control. We hypothetised (1) that TPD threshold at the back is larger in patients than in healthy controls and (2) that larger TPD threshold relates to worse voluntary lumbopelvic control.
Methods
Setting
A cross-sectional study of back-pain patients and healthy controls was undertaken in a private physiotherapy practice in Reinach, Switzerland. All participants gave written informed consent. The study was conducted according to the Helsinki Declaration and was approved by the ethical committee of canton Aargau, Switzerland.
Subjects
A convenience sample of 45 patients (20 males) with non-specific low back pain for at least 3 months (mean (SD): height, 170 (8) cm; weight, 74 (16) kg; age, 43 (15) years) and 45 age- and sex-matched healthy controls (20 males; mean (SD): height, 171 (7) cm; weight, 69 (12) kg; age, 41 (10) years) participated. Patients who presented for treatment of their back pain, and who described an area of pain that fell between the spinous processes of T10 and L5, were eligible. Patients who also described leg pain were still eligible. Thirty (66%) patients reported pain beyond their gluteal folds. Patients were excluded if the interview revealed red flags or the physical examination revealed non-stable neurological signs. The presence of non-red flag structural abnormalities that were identified via radiology was not an exclusion criterion. Healthy controls were excluded if they had back pain that impaired activities of daily life in the past 2 years or had a neurological, orthopaedic or psychiatric condition that would affect lumbopelvic control or tactile acuity.
Measures
Demographic data, including self-reported habitual activity, were obtained from all participants. Patients underwent a normal interview and physical assessment with a physiotherapist and completed the Roland–Morris Disability questionnaire12 and the Coping Strategies Questionnaire.13
TPD threshold was measured according to established protocol,14 by a plastic calliper ruler in the area between the first lumbar vertebra and iliac crest left and right, both horizontally and vertically. TPD threshold was defined as the shortest distance between the calliper points at which the participant could clearly detect two points instead of one and was calculated as the average of a descending run (5 mm increments from 10 cm) and an ascending run (5 mm increments from 1 cm). To make sure the participant was not guessing according to the pattern of stimuli that were presented, we included stimuli that were out of sequence (expanding the callipers instead of contracting them or vice versa).
Lumbopelvic movement control was evaluated by a battery of six individual tests, which yield a total score out of six. For each individual test, participants are given, as a reference, a picture in which a model demonstrates the target alignment of the pelvis and lumbar spine. A trained physiotherapist judges whether the correct alignment has been obtained, in which case the test is considered negative, or unsuccessful, in which case the test is considered positive. A score of 6 denotes a poor ability to voluntarily adopt certain alignments of the pelvis and lumbar spine, on the basis of a picture. This battery of tests has been investigated in healthy controls and patient groups and has established internal consistency and high between-therapist reliability once therapists have received appropriate training.15 16 Patients with back pain perform worse than healthy controls on this battery of tests.16
Statistics
Statistical analysis was undertaken in SPSS V.16.0. Point values, means and SD were calculated. To test the hypothesis that TPD threshold is greater in patients than it is in healthy controls, we used a multivariate analysis of variance with within subjects repeated measures factor test (vertical TPD, horizontal TPD) and between-subjects factor group (patients, controls). We compared performance on the lumbopelvic movement control tests between patients and controls via a t test for independent samples. To test the hypothesis that a larger TPD threshold related to worse voluntary lumbopelvic control, we used a Pearson correlation coefficient. Significance was set at p<0.05.
Results
There were no differences between patients and controls on habitual activity, age, height and weight (p>0.2 for all). Twenty-eight (65%) patients and 32 (70%) controls were in paid employment. Three patients (8%) were in receipt of disability allowances. For patients, mean (SD) Roland–Morris disability questionnaire12 score (maximum score, reflecting maximum disability due to back pain=24) was 9 (5) and mean (SD) catastrophising subscale of the coping strategies questionnaire13 score (where maximum score, reflecting maximum catastrophising=36) was 13 (8).
TPD threshold
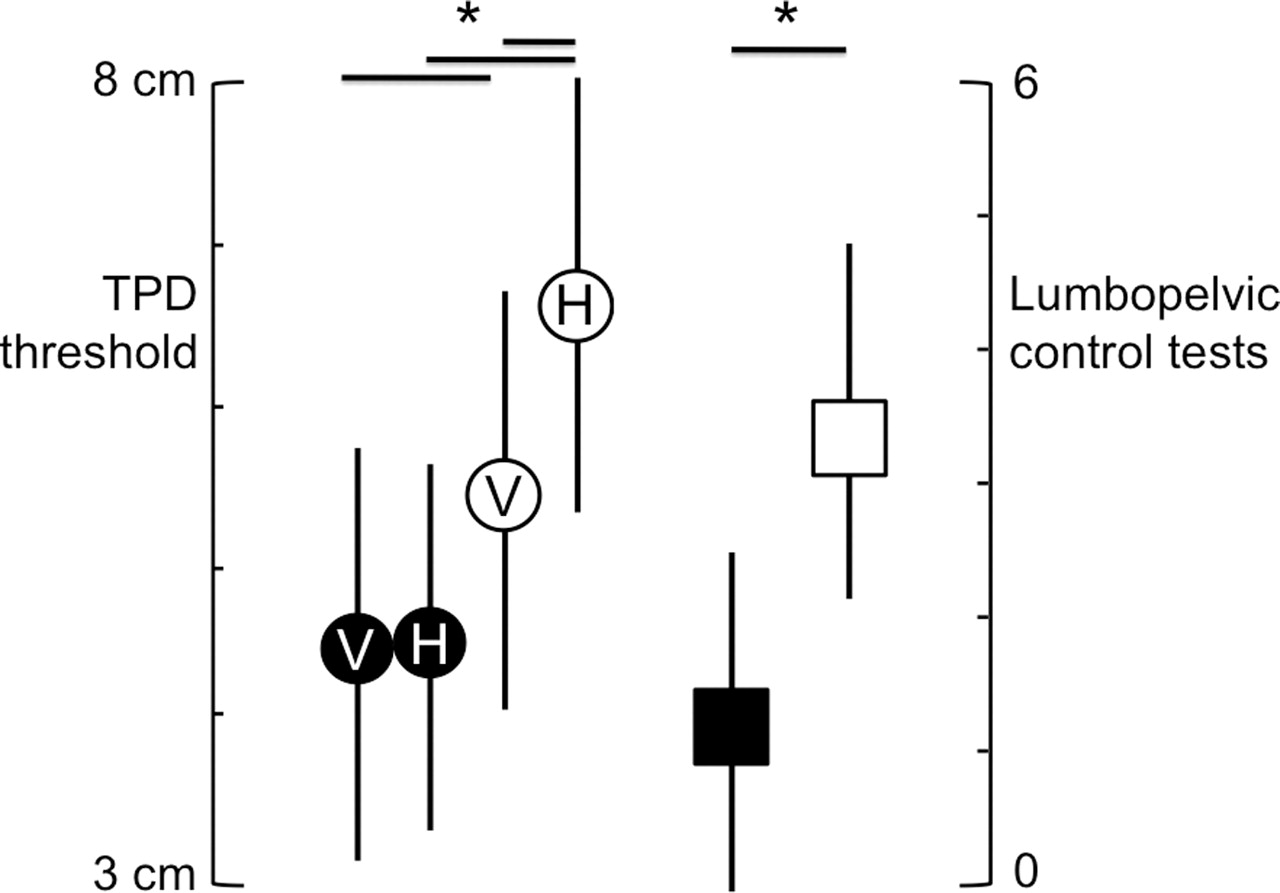
Vertical TPD threshold was less than horizontal TPD threshold (main effect of test F(1,88)=26.0, p<0.001), but this was driven by a large difference between vertical and horizontal TPD in patients (Group×Test interaction (F(1,88)=15.9, p<0.001; fig 1). TPD threshold was greater in patients (mean 60, 95% confidence interval (CI) 57 to 64 mm) than in controls (44, 95% CI 40 to 48 mm); main effect of group, F(1,88)=40.5, p<0.001). The difference in TPD threshold between patients and controls was greater in the horizontal direction than it was in the vertical direction (p=0.03). That is, although TPD was worse in patients than in controls in both the horizontal and vertical directions, the extent to which it was worse was greater in the horizontal direction than in the vertical direction.
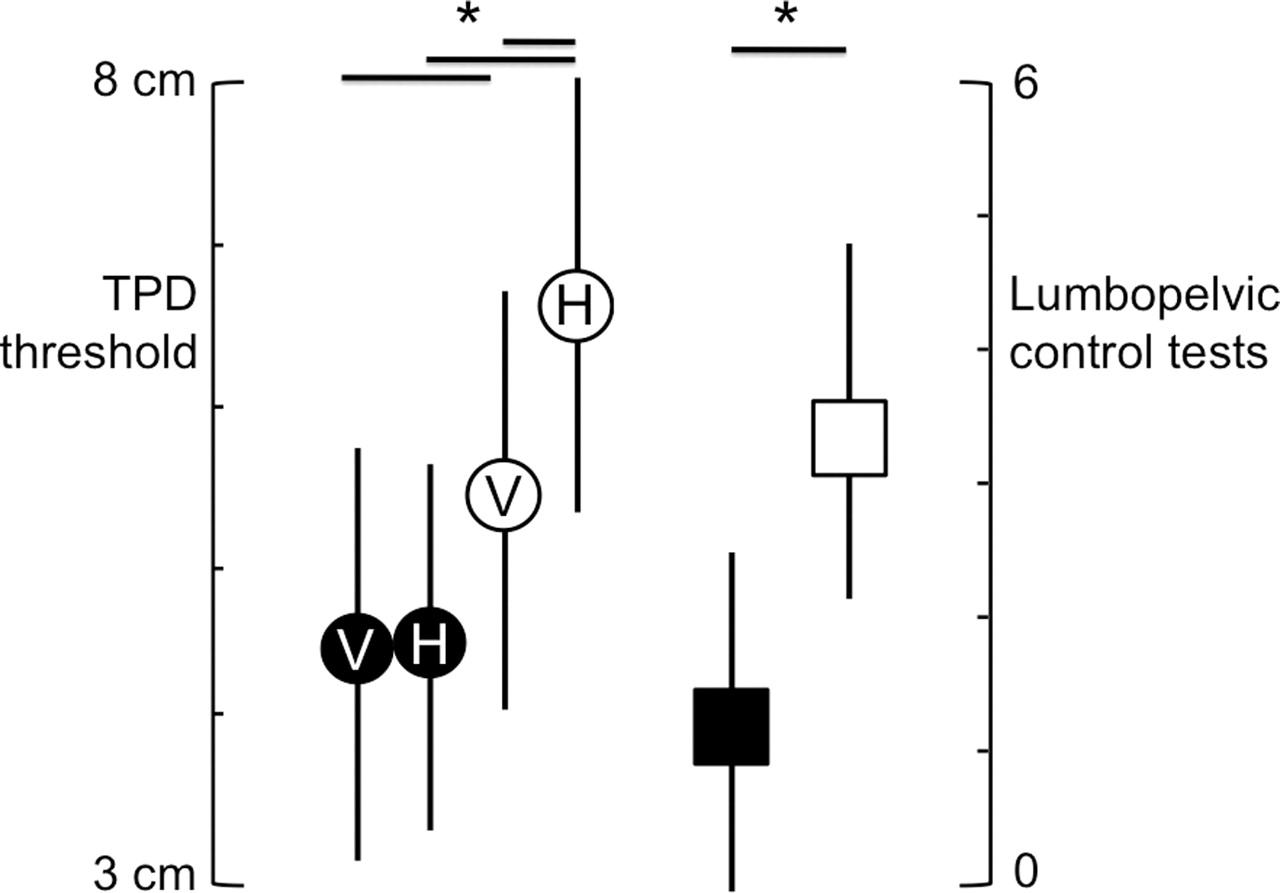
Two-point discrimination (TPD) threshold (left vertical axis, circles; V, vertical TPD; H, horizontal TPD) and number of positive tests on the voluntary lumbopelvic control test battery (right vertical axis, squares) for back-pain patients (open shapes) and healthy controls (filled shapes). *p<0.05.
Lumbopelvic control
Healthy controls had better lumbopelvic movement control than back-pain patients did: mean (SD) score on the lumbopelvic movement control test for patients was 3 (1.1) and for healthy controls was 1 (1.3) (t(88)=7.9, p<0.001; fig 1).
The relationship between TPD threshold and lumbopelvic movement control
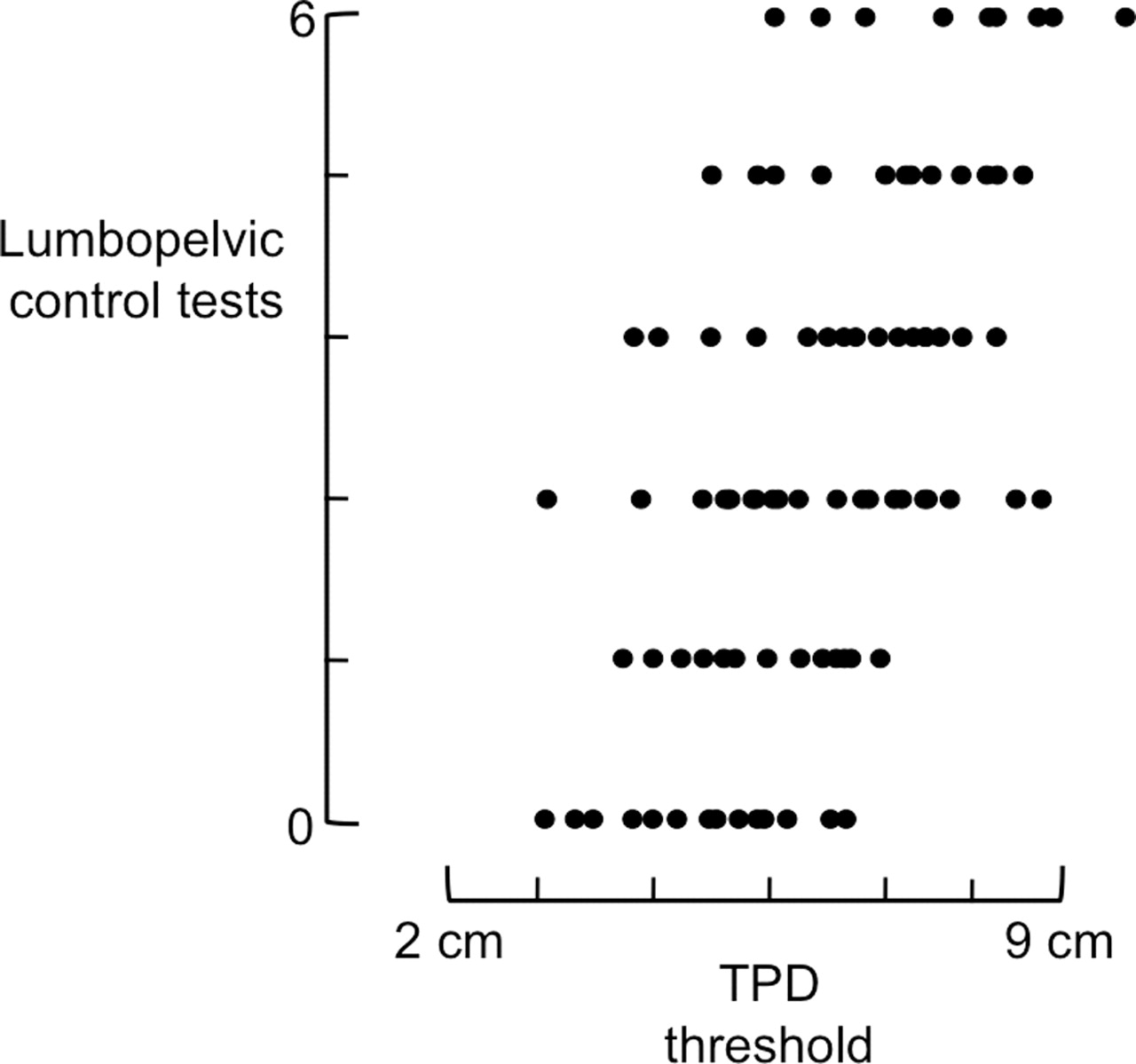
TPD threshold was negatively related to lumbopelvic control. That is, the higher TPD threshold at the back, the more positive tests there were on the lumbopelvic movement control test battery (Pearson's r=0.49, p<0.001; fig 2).

{kind=link}
{kind=link}
Scatterplot of all subjects (45 back-pain patients and 45 controls) between two-point discrimination (TPD) threshold (x-axis) and number of positive tests on the lumbopelvic control battery (y-axis, maximum=6). Regression yielded significant correlation Pearson's r=0.49.
Discussion
We hypothesised (1) that TPD threshold at the back is greater in patients with back pain than in healthy controls and (2) that larger TPD threshold at the back relates to worse voluntary lumbopelvic control. Our results support both hypotheses. Increased TPD threshold at the back corroborates our previous report in a convenience sample of eight patients with back pain10 but provides the first comparison between patients and controls. A relationship between TPD threshold and lumbopelvic movement control is a new finding that has clear implications for back pain rehabilitation, particularly where motor training is involved.
Increased TPD threshold at the back is probably confined to the area of usual pain—we found normal TPD thresholds at the thoracic level in patients with lumbar pain,10 and others have shown normal TPD threshold elsewhere in the body in those with back pain.17 Where, then, might the effect occur? TPD depends on intact mechanisms throughout the sensory neuraxis—from peripheral sensory neurons to S1. It seems unlikely that transmission of the stimuli to the brain is reduced in people with back pain, because the S1 response evoked by electrical cutaneous stimulation at the back is not delayed, nor diminished, in patients with back pain.6 Perceptual threshold is also unaffected.10 However, spinal mechanisms mediate central sensitisation, via which peripheral Aβ cutaneous input activates spinal nociceptors.18 Therefore, although the speed and magnitude of the cortical response to cutaneous stimulation is unaffected, the spinally evoked noxious input may lead to supraspinal noise and a loss of normal inhibition. Whether spinal sensitisation contributes or not, supraspinal mechanisms seem most likely to explain the loss of tactile acuity in back pain. EEG data, showing a shift and expansion of the representation of the back in S1 in patients with back pain,6 implicate S1. Notably, however, larger S1 representation usually corresponds with greater tactile acuity. It seems likely, then, that expansion of S1 representation associated with back pain reflects “smudging”, or overlapping representations, rather than expansion of discrete S1 receptive fields.6 That TPD threshold is considered a clinical signature of S1 organisation in other pathological pain states, for example phantom limb pain and complex regional pain syndrome,19 lends support to the notion that increased TPD reflects shifts in S1 response profiles, although without corroborative functional imaging, we cannot be sure.
Regardless of where the deficit in TPD is mediated, that it is related to lumbopelvic control is an important finding, for two reasons: first, it raises the possibility that cutaneous input plays a larger role in proprioceptive input than was previously thought. Although cutaneous input is known to contribute to proprioception,20 precise experiments interrogating motor control of a single finger show that elimination of cutaneous input via topical anaesthesia in healthy human volunteers has only a small impact on movement control.20 Extrapolation of those data to back-pain patients would imply that the effect of decreased tactile acuity on back movement control would also be small. Perhaps, then, cutaneous input plays a bigger proprioceptive role in people with back pain than it does in people without back pain, such that decreased tactile acuity has a larger impact on back movement control than it would in a healthy normal population. There is some corroborative evidence for this line of thinking—vibration of multifidus induces illusory movement and disrupts proprioception in healthy participants, but it does not have these effects in back-pain patients. That is, muscle spindles appear to not contribute to lumbopelvic proprioception in patients with back pain but they do in those without back pain.21 Another possibility, however, is that increased TPD threshold and lumbopelvic motor control dysfunction are epiphenomena of some other process (although pain is unlikely to be a cause).22 This is an important consideration because the cross-sectional nature of the current work cannot demonstrate a causative relationship. The possibility that poor tactile acuity disrupts lumbopelvic control could be easily clarified by training tactile acuity and reassessing control.
Tactile acuity seems very responsive to training. In patients with complex regional pain syndrome, which is also characterised by decreased tactile acuity, a single 30-min session of tactile discrimination training can decrease TPD threshold by up to 10 mm, and an effect lasts for at least 48 h.23 Two weeks of daily tactile discrimination training normalises tactile acuity in that patient group.24 Moreover, and importantly in light of S1 reorganisation observed in patients with back pain, normalisation of TPD threshold coincides with normalisation of S1 representation in people with complex regional pain syndrome and phantom limb pain (see Flor et al, Lotze and Moseley25,–,27 for reviews). These findings, taken together with the current results, suggest that tactile discrimination training might help normalise lumbopelvic proprioception and motor control in patients with back pain. Although preliminary data using an electrocutaneous sensory discrimination training device for chronic back pain showed no effect on pain,28 that study did not investigate lumbopelvic control, nor TPD treshold data, which leaves the question open for investigation. Importantly, this notion is speculative—the current data do not constitute evidence for this treatment approach.
The current findings may generalise to other chronic pain populations, but we cannot be sure. That is, it is possible that concommitant tactile acuity and motor control deficits are confined to complex regional pain syndrome and back pain. We know that deficits of postural and motor control go hand in hand with chronic pain (see Moseley and Hodges29 for a review), and tactile acuity deficits have been reported for a range of chronic pain disorders (eg, facial pain),22 but we cannot conclude, on the basis of the current data, that loss of tactile acuity causes motor control dysfunction, nor that the relationship between these factors is ubiquitous.
Interpretation of the current findings should consider several issues. First, this was a pragmatic cross-sectional study undertaken within a clinical setting. We did not have access to electromyography, which would have permitted detailed investigation of motor output and provided an empirical corroboration of the clinical lumbopelvic control tests used here, nor to EEG, which would have permitted detailed investigation of tactile processing. Second, we may have detected larger or more specific effects if we had confined the study sample to those with particular diagnoses or level of habitual activity, although that would have also limited the generalisability of our results. Third, although the assessment of TPD was blinded to group, and the assessment of lumbopelvic control was blinded to TPD, we did not blind the therapist assessing lumbopelvic control to group because preliminary testing suggested that this would be impossible to do. That is, the fact that a patient has back pain is quickly apparent to many experienced clinicians.
Conclusions
TPD threshold at the back is greater in patients with back pain than in healthy controls, and greater TPD threshold at the back relates to decreased voluntary lumbopelvic control. These findings raise the possibility that decreased tactile acuity may contribute to poor motor control, which has implications for back pain rehabilitation in particular and for movement retraining in general.
What is already known on this topic
▶ That chronic pain is often associated with functional reorganisation of the primary sensory cortex, that tactile acuity provides a clinical signature of the receptive fields represented in the primary sensory cortex and that cutaneous input contributes to proprioceptive acuity and therefore motor control.
What this study adds
▶ This study clearly demonstrates that tactile acuity at the back is decreased in people with chronic back pain and that the reduction in tactile acuity relates to decreased lumbopelvic control as determined by clinical assessment involving lumbopelvic positioning using a photograph as a frame of reference.
Acknowledgments
GLM supported by Nuffield Dominions Trust, UK, and the National Health and Medical Research Council of Australia.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the ethical committee of canton Aargau, Switzerland.
-
Provenance and peer review Not commissioned; externally peer reviewed.