Article Text

Abstract
Objectives The authors reconfigured the emergency care system of Addenbrookes Hospital, Cambridge. The medical admissions unit and the emergency department (ED) have been combined into one emergency assessment unit. This paper aims to determine if reconfiguration has reduced non-elective hospital admissions and reduced mortality for non-elective admissions.
Design A retrospective ‘before and after’ study in a teaching hospital. Routinely collected data were used to evaluate the effectiveness of this approach.
Setting One acute trust in the UK.
Main outcome measures Inhospital mortality rates and standardised admission ratios (SAR) between 2003 and 2009.
Results There was a significant trend towards improved survival, both for non-elective admissions and deaths in the ED (z=−3.92; p>0.001), despite the age and acuity of patients increasing. There was a marked decrease in the SAR. Formal complaints, incident reports and the proportion of patients leaving before treatment declined, whereas the proportion of patients re-admitted as an emergency within 28 days did not change.
Conclusions Integrating emergency care within a hospital reduces hospital admissions, is associated with reduced inhospital mortality and a better quality of care.
- Cardiac care
- care systems
- cost effectiveness
- emergency care systems
- emergency departments
- emergency department management
- management
Statistics from Altmetric.com
- Cardiac care
- care systems
- cost effectiveness
- emergency care systems
- emergency departments
- emergency department management
- management
Emergency care processes are imperfectly designed. Current systems of emergency care are complex and have evolved over many years, rather than resulting from careful planning. Most hospitals have experienced unprecedented rising demand for non-elective work over the past decade. There have been several interventions to try and improve the efficiency and functionality of the emergency care system.1 The majority of the evidence to support differing models is of low quality. There is very little original research that evaluates the benefits of combining parts of emergency secondary care. The majority of relevant research has looked at improving flow within emergency departments (ED), or has focused on reducing attendances at ED. This evidence gap was identified: ‘Surprisingly little research has been undertaken in the areas of bed management, innovations to reduce delayed discharges, working practices and workforce numbers.’2 3
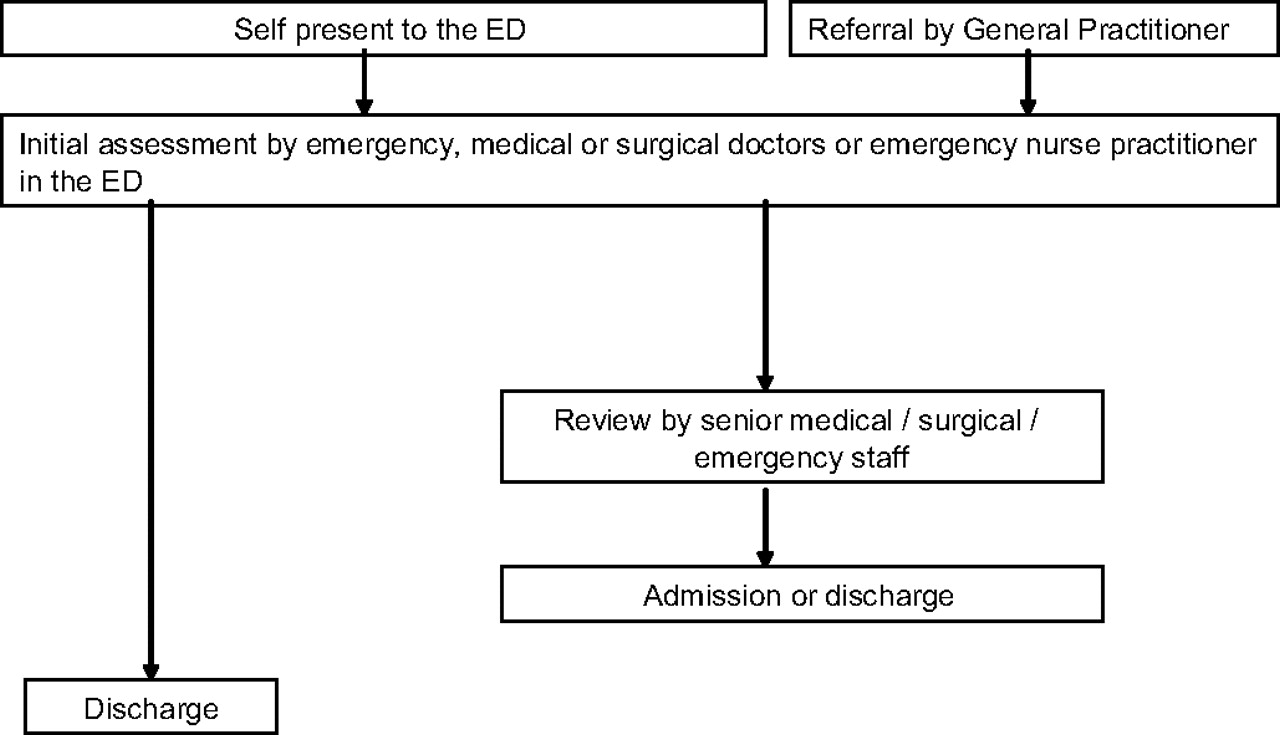
In June 2004, we embarked upon a redesign of the process of assessment for patients presenting as an emergency. The new system started in June 2006. The principal modification was the relocation of the medical admissions unit (MAU), including medical and nursing staff, into the ED in conjunction with a combined assessment process for all specialties using the ED. This new model was called the emergency assessment unit (EAU). This was accompanied by a change in environment, staffing, working practices and diagnostic service support. Our ED was expanded from 28 cubicles to 40. We increased the medical staff, in addition to combining the nursing and medical staff from the MAU with the ED; we appointed three consultants, two specialist registrars in acute medicine and two new emergency medicine consultants. We modified working practices; the process changes are summarised in figures 1 and 2. We were supported in this by increased pathology and radiology support; so that there was minimal delay in getting relevant test results. We are supported by physician assistants who provide phlebotomy before clinical assessment so that a clinician can make a prompt decision with the benefit of relevant blood test results. All of these changes were designed to reduce the duplication of clinical assessment and improve efficiency.

Traditional process for evaluating patients presenting for unscheduled care before 2006. ED, emergency department; MAU, medical admissions unit.
Streamline process for evaluating patients for unscheduled care before 2006. ED, emergency department.
Previous exploratory work has indicated that integrating emergency care services in one place with a flexible team had a possible benefit on mortality and a clear effect on reducing emergency admissions.4 A further evaluation was performed to identify if this possible mortality benefit was evident through the opportunity of greater data acquisition. This study also explored whether the benefits in terms of quality reported in 2008 had been sustained.
Methods
Multiple, routinely collected measures were used to evaluate the effectiveness and quality of our approach. Data have been routinely collected on a quarterly basis from 2003 until the switch to an integrated process in June 2006 and then afterwards to the end of the first quarter of 2009.
Dr Foster data were used to identify changes in mortality before and after integration and the change in length of stay for non-elective admissions, all-cause mortality and HSRM (HSMR comprises a basket of 56 diagnoses accounting for approximately 80% of deaths in most hospitals). Data for non-elective admissions were examined. No practically important difference between the two mortality measures was found, so only the all-cause mortality results are reported. The appropriate data year as the benchmark was used as our comparator. Dr Foster data were also used to examine trends.
A routinely collected measure was used to compare our standardised admission ratios (SAR). This uses data from general practitioner (GP) practices in which over 80% of referrals from these practices were to our institution. This was subsequently adjusted for deprivation by the Dr Foster unit. Trends were examined for statistical significance using the p test for trend and we compared categorical data with the χ2 test. We used STATA version 7 and CI Analysis (BMJ publishing).
The number of admissions and number of attendances to our department is presented. The quality indicators identified in 2008 were re-examined; these were the proportion of incident reports, formal complaints, the proportion of patients who left before being seen, re-attendance at the ED within 24 h and re-admission within 28 days.
We did not seek ethical approval, as this was a service evaluation using routinely collected anonymous data.
Results
When we changed our emergency care system, the numbers passing through the ED increased. The ED became the main route for non-elective admissions into the hospital. The demographic characteristics of our patients are shown in table 1. There were slight increases in the proportions of women arriving at the ED, in older age categories and higher triage categories (see table 1). The case mix probably represents sicker patients.
Demographic characteristics of patients arriving at the ED before and after the establishment of the EAU
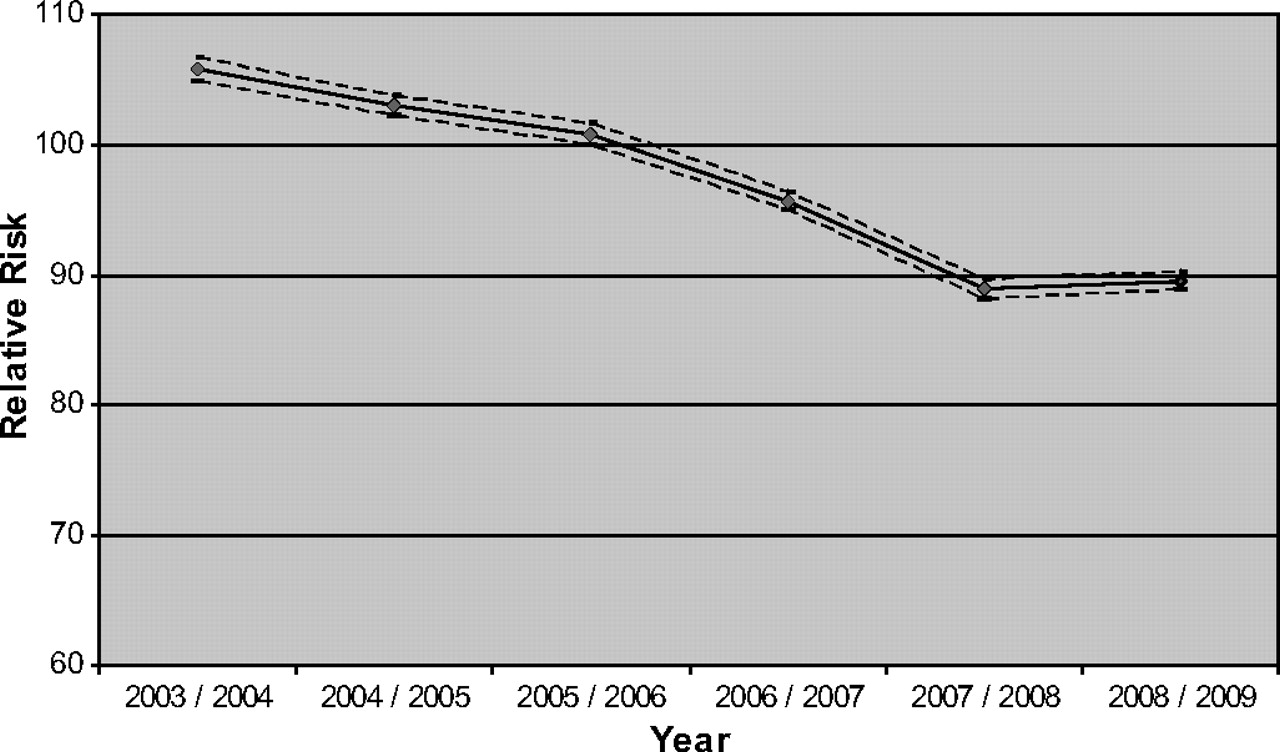
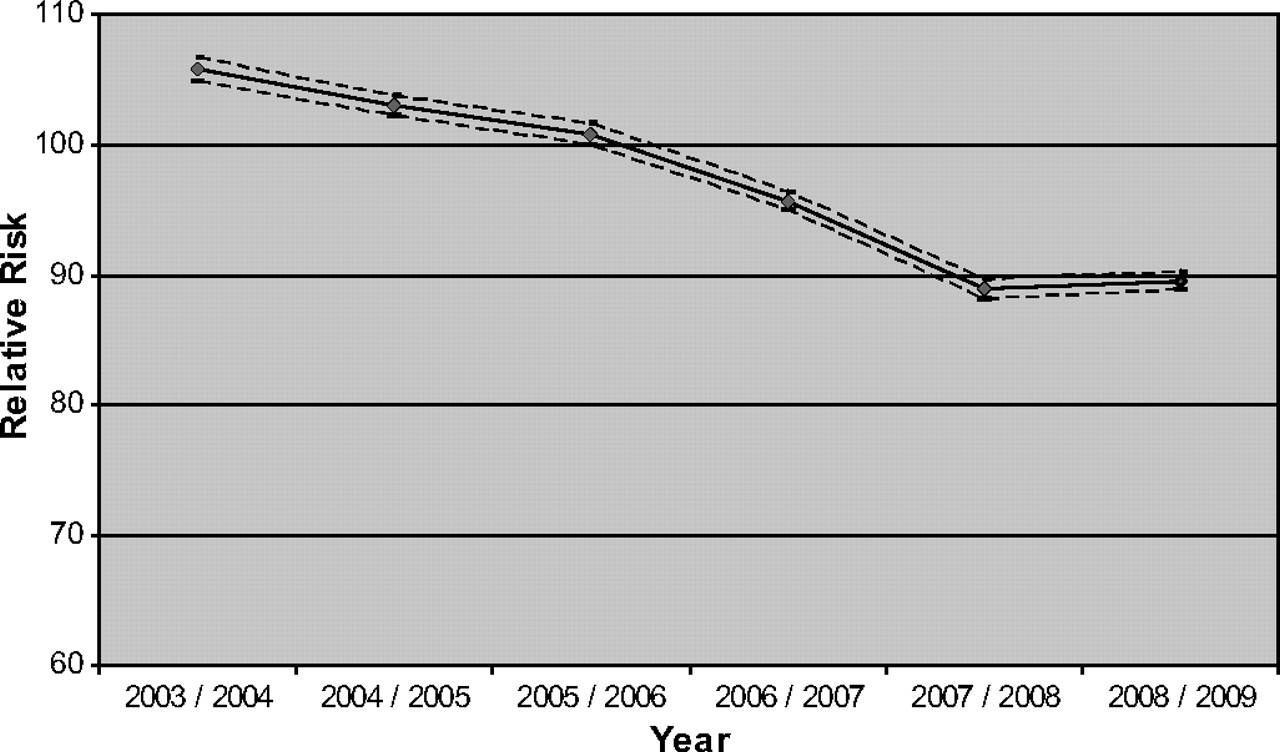
There was a significant trend to improved mortality for the percentage of deaths occurring in the ED (z=−3.92; p>0.001) and adjusted RR over the study period (z=−3.59; p>0.001) (see tables 2 and 3 and figure 3).
Numbers of patients
All-cause mortality for non-elective admissions to Addenbrookes
Mortality (in hospital)/diagnoses all/non-elective.
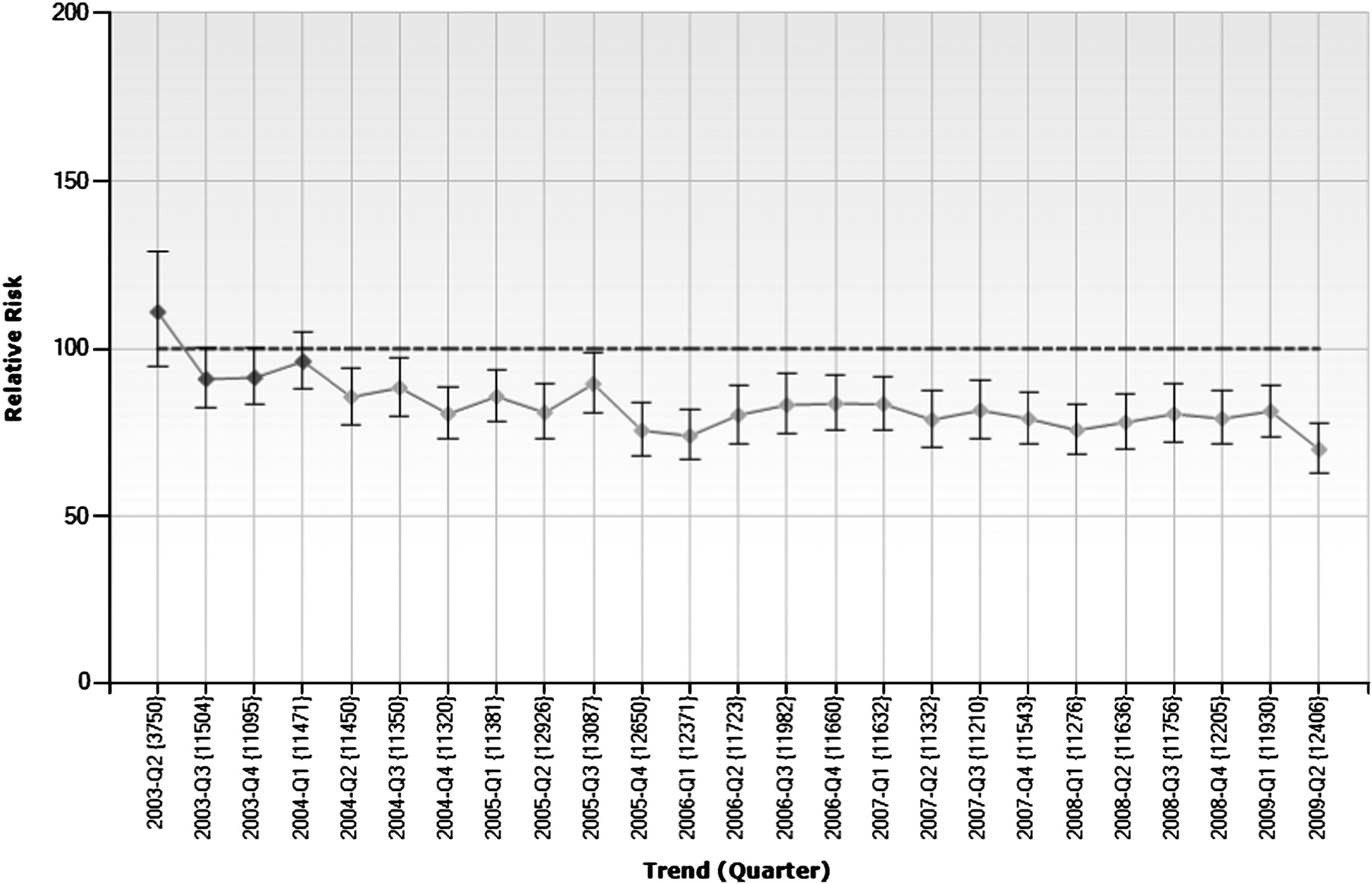
There was a drop in SAR. This drop was maintained when we adjusted for deprivation. The trend for the decline in unadjusted SAR was not significant (z=−1.65; p=0.10). This relationship was also not significant when we adjusted for deprivation (z=−1.66; p=0.10; table 4).
Standardised admissions ratio
There was a practically important and statistically significant decline in incident forms. The decline in patients who left without being seen was statistically, but not practically, significant. The number of non-elective re-admissions within 28 days remained constant. The number of formal complaints did decline, but this effect was not practically or statistically significant (table 5).
Measures of quality of care
Figure 4 shows the trend in all-cause mortality for non-elective admissions.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Standardised admissions ratio adjusted for deprivation (95% CI).
Discussion
We have evaluated the effect of combining the MAU and ED and found that mortality rates have fallen while we have managed to reduce the number of patients who are admitted to hospital. This has allowed the emergency care system to deliver its core function of saving lives while admitting only those patients who need to be admitted. We have found the quality of care has improved, by less complaints and incident forms. This paper also illustrates the usefulness of using routinely collected data to evaluate system changes and clinical performance at a system-wide level. Our measure of SAR, although novel, has great potential to evaluate the urgent care system; it provides useful benchmarking information, responds to changes and appears to be a valid measure.
Limitations
There are some important limitations to this study. The use of hospital mortality ratios to assess performance is controversial.5 6 Hospital mortality ratios are only collected on admitted patients, so they might fall or fail to rise if lots of patients were dying in the ED, other hospitals or at home. Our data show this was not the case and there was in fact a decline in the number of patients dying in the ED. We transfer very few patients out of our hospital (mainly burns and cardiothoracic emergencies) and it is likely we would have been aware of any increase in the number of patients dying after discharge from the ED. Any apparent improvements in mortality ratios may be attributable to improved coding, in particular the improved identification of palliative care codes. We are unaware of any significant improvements in our data collection, although this remains a possibility. While comparing HMSR across hospitals is controversial, we compared trends within a single centre over time. The biases may still be present, but are likely to be smaller and more constant.
Our choice of admission ratio can be criticised as arbitrary; however, we had to define a denominator population, and using GP practices that refer more than 80% of their patients to our department seems valid and without bias.
Our findings are from a single centre and the external validity is not clear. We have before and after data only, without a control group, we cannot be completely sure that any changes in the admission ratios we have seen are the result of the integration of our services. There have been other changes that reduce non-elective admissions, although we think any such changes would be unlikely to have made such a large change. Within our hospital, we have had a consultant expansion in both emergency medicine and acute medicine, and there has been an expansion in out-of-hours radiology provision. These may all have helped to reduce mortality. The biggest two changes in non-elective care systems over the study period have been the introduction of the 4-h target and the re-negotiated GP contract, which reduced GP involvement in out-of-hours care.7 We cannot see a plausible mechanism for the 4-h target and the GP contract reducing admission ratios. There have been many other smaller changes in the way care is delivered over the study period. However, the difficulties of randomising such a complex and large intervention means that controlled trials are unlikely to be conducted.
This paper has not explored the use of improved community services—such as home-based palliative care nursing, or a responsive district nurse visiting service that can deliver rapid clinical intervention in the community. However, the authors are not aware of any significant changes in community provision over the period of the study.
We used a pragmatic study design, and cannot be sure what parts of our intervention led to the changes. We are unable to quantify the costs of the benefits that we have identified, as the costs and tariffs of attendance, admissions and hospital stays are continually changing and are extremely complex to model. However, dramatically reducing admissions to hospital without any apparent increase in mortality or non-elective re-admissions must be beneficial for the health economy.
It is desirable to reduce emergency admissions appropriately—both for patients and the NHS. The current NHS operating framework also provides a specific incentive for acute trusts in 2010/11 as emergency activity above their 2008/9 baseline only attracts 30% of tariff.8 The use of a proxy SAR as proposed in this paper allows for a comparison between acute providers, and as such is a more clinically relevant indicator than crude improvements on a hospital's historic position, which can mask shifts from other hospitals and fails to distinguish consistently good performance from consistently poor performance. We think, on the evidence that we have presented, that our model of emergency care is more efficient and effective and represents an improvement. This model of emergency care allows our ED to admit fewer patients without any increase in adverse events. This benefits the whole healthcare system. Our system is better for our patients, as they are not subjected to multiple, confusing assessments. Future work might consider a qualitative evaluation of staff or patient experience in this environment, or whether this model can be applied to other ED.
Our system of emergency care has reduced our performance against the 4-h target, like many ED we have struggled to meet the threshold of 98%. However, we feel that the benefits to the wider health economy and to our patients are outweighed by the difficulties we have in achieving this process standard, which has in any event now been reduced to a threshold of 95% and looks likely to abandoned.9
Conclusion
Integrated emergency care reduces non-elective admissions without any measurable increase in mortality. This is an improvement in the organisation of emergency care, offering advantages to patients and a reduction in costs for commissioners.
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey