Article Text

Abstract
Objective: To determine medical and nursing staffing levels in emergency departments in England and Wales.
Methods: A postal survey with an addressed return envelope was sent to all emergency departments in England and Wales enquiring about staffing levels and annual attendances.
Results: Responses were received from 91/202 departments (45%). Great variability was seen in medical and nursing staffing levels across departments in England and Wales. The predominant members of the medical workforce were SHO grade doctors. The number of senior and middle grade doctors generally increased as departments became larger. Nursing levels were not as responsive to departmental size.
Conclusions: There is great variability in staffing numbers in similar-sized departments, and most departments are understaffed in comparison with the recommendations of the British Association for Emergency Medicine to achieve the 4 h target at the 90% level.
Statistics from Altmetric.com
Appropriate staffing of the emergency department is the single most important factor in providing a prompt, timely and clinically effective service to patients. All emergency departments within the UK have an establishment for medical and nursing staff with which to perform their activities. These numbers are influenced by local historical factors, trust priorities and finances, 4 h targets, local activity profiles, staff seniority, working styles, availability of support staff, ability to recruit staff, European Working Time Directives, changes in junior doctor educational requirements, case mix, patient numbers and many other factors. In 2005 the British Association for Emergency Medicine (BAEM) indicated in the “Way Ahead” document the appropriate medical staffing levels necessary for UK emergency departments to carry out their core activity and achieve 90% of the 4 h target.1
There are no recommended numbers for nursing staff levels in the UK. The Department of Health and the Royal College of Nursing state that establishment levels are of concern for individual trusts only.2–4 Ideal nursing levels for intensive care units, coronary care units and labour wards have been published in the UK,5 6 emergency department nursing levels are set in statute in California and guideline numbers are published in Australia.7 8
The objective of this study was to compare medical and nursing staff numbers in emergency departments in England with the BAEM recommendations.
METHODS
A postal survey was sent to all emergency departments in England and Wales. Departments were identified from the 2005 BAEM directory and a questionnaire (see appendix 1 available online only) with a covering letter and addressed envelope for return was sent to the clinical director. Two hundred and two departments were identified as being suitable to be included in the survey, which was carried out in April 2007. A 6-week cut-off period was chosen in which to receive replies.
RESULTS
Responses were received from 91 departments (45%). Table 1 shows the mean number of staff categorised by size of department. The range indicates the spread of all positive responses.
Figure 1 shows the trend in medical staffing as the number of patients per department increased. A gradual increase was seen in all levels of staffing, but with a disproportionately larger increase in the number of SHOs as departments got bigger.
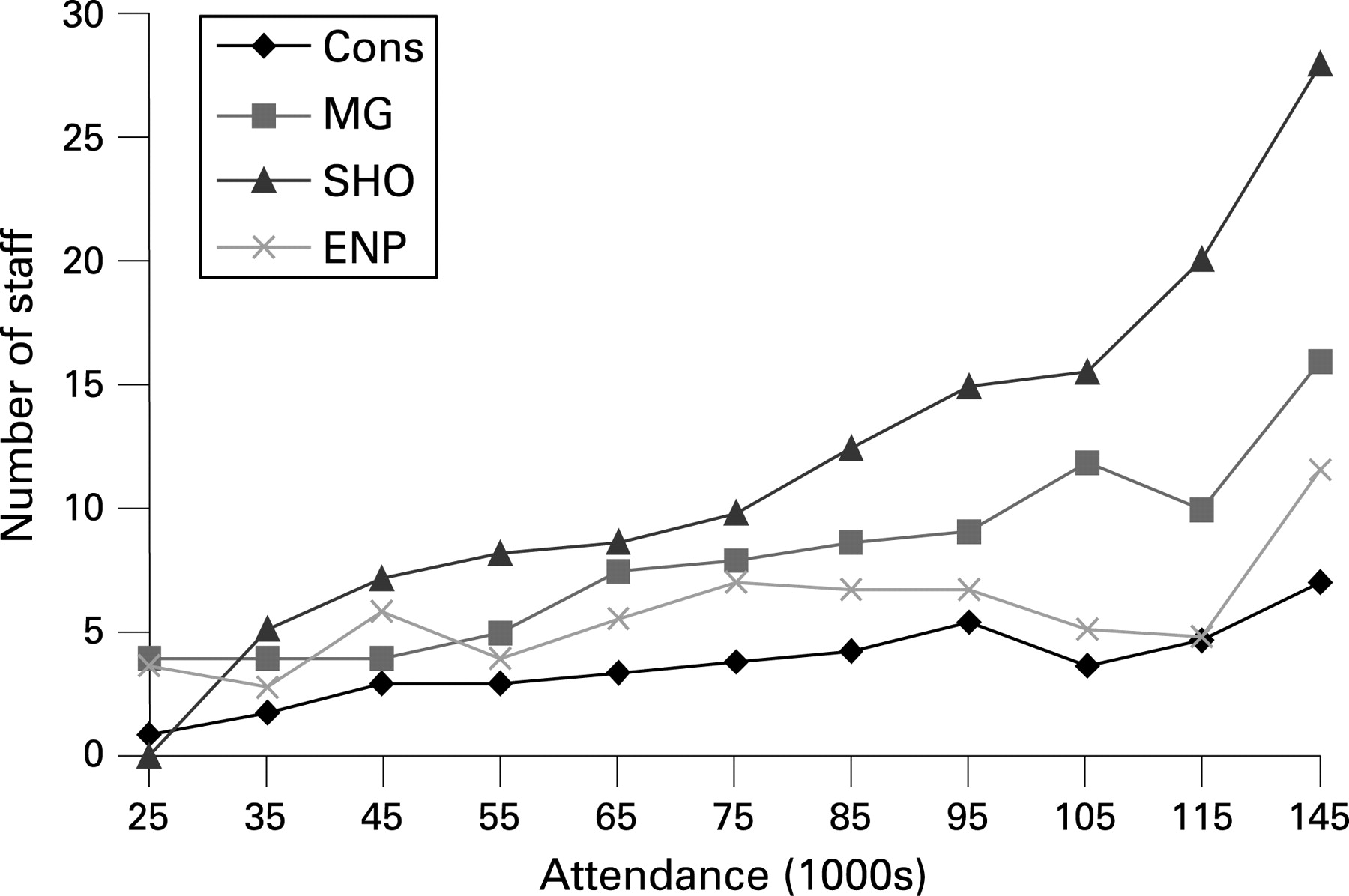
Table 2 shows nursing staff levels by size of department. The range indicates the spread of all positive responses.
Figure 2 shows this information in a visual format which, unlike medical staffing, demonstrates that there is no obvious pattern of levels of nursing staff in relation to the number of patients using a department.

DISCUSSION
The BAEM introduced the concept of the workload unit in the “Way Ahead” document,1 where a workload unit was defined as 3000 patients per year of normal case mix. The BAEM then went on to further define the amount of work expected from various grades of staff in terms of workload units (table 3), and to describe minimum numbers and levels of staff that a department of standard case mix would require to provide an adequate service and achieve the 4 h target at the 90% level (table 4).
Most departments were understaffed in comparison with BAEM recommendations for staffing departments in terms of work load units with respect to the 90% 4 h target. Emergency departments within the UK now have to conform to a 98% 4 h target, and therefore actual staffing levels would fall well below that which is recommended to achieve and maintain this higher target (fig 3).

{kind=link}
{kind=link}
{kind=link}
Many departments use SHO level doctors as the mainstay of their clinical workforce for service provision. We did not look into whether these SHOs are in stand-alone posts or are part of rotations in other specialities. Departments will have to make difficult decisions regarding service provision when the full provisions of Modernising Medical Careers (MMC) come into effect as stand-alone posts will no longer exist and, while fixed term specialty training may well make up the shortfall during the transition period, there is no guarantee that funding and approval for these posts will continue. When the full effects of MMC and centralised workforce planning come into effect, emergency medicine departments that use SHO level doctors as the major component of their medical workforce may find that they do not have enough doctors to provide a safe service.
Many large departments provide consultant supervision into the evening well beyond normal working hours. The very large multiconsultant departments envisaged as the future of emergency medicine—providing consultant supervision well into the early hours of the morning—do not currently exist. As departments get larger the increase in the number of consultants is smaller than that recommended by BAEM. We can speculate as to the reasons for this.
Primarily, consultants are employed by NHS trusts that are increasingly run to a business model. Consultants are an expensive resource and employing more than the 6–8 needed to run most large departments in terms of administration, teaching, service development and shop floor supervision entails a large expense that may not be justified with respect to increased income or the marginal cost of providing increased consultant supervision later into the evening. Smaller departments cannot provide consultant level care beyond office hours with their present staffing levels. Many of these departments do not even have enough middle grade doctors to provide 24 h middle grade cover and are staffed by SHOs alone at night. Individual departments need to decide if this level of cover is appropriate for their department, bearing in mind the number and acuity of attendances at the department out of hours.
Four factors will influence the direction of future staffing levels in emergency departments in the UK:
Models of care envisaged by the College of Emergency Medicine and the Department of Health with centralised large departments being staffed by trained doctors and increased amounts of emergency care being performed in the community by non-medical personnel.
Individual acute trust budgets: they will have to decide how best to provide their local service. A service provided by doctors in training or predominantly by consultants is not the most cost efficient.
MMC: all MMC documentation talks about post certificate of completion of training (CCT) specialists, not consultants. The opportunity to have large numbers of doctors in training in various specialties rotating through emergency medicine has been lost.
Visa regulation and employment law: emergency medicine employs many non-career grade doctors who are often from overseas. This pool of doctors in the future may well reduce as junior doctors from overseas are being actively discouraged from coming into the UK by the MMC and changes in visa regulations. Whether doctors from the new member EU countries can fulfil this need in future remains to be seen.
Nursing numbers show a very different pattern from medical staffing numbers, with levels being set almost independently of departmental attendances and a very gradual increase in the number of nurses as departments increase in size.
There are no national UK guidelines for emergency department nursing establishments, although Australia and parts of the USA have minimum nurse:bed ratios for emergency departments.7 8 Traditionally, the UK has employed a bottom-up method for determining nursing numbers which, while taking into account some measure of workload, is heavily dependent on some level of personal judgement by local managers. Victoria, Australia has set into legislation a minimum level of one nurse per three patients plus a nurse in triage plus a nurse in charge of the whole emergency department. California has legislated that the maximum number of patients that can be looked after by a nurse in an emergency department at any one time is four, with a maximum of two critical care patients or one trauma patient. There are no guidelines or recommendations as to skill mix and seniority and there is a dearth of research into the effect of skill mix on patient outcomes in the UK, although such work has been carried out in the USA where a positive relationship has been found between outcome and higher levels of trained registered nurses.
We recognise that departmental attendance is a very crude measure of departmental activity, but it does provide a useful indicator of departmental workload. The range of nursing and medical staff in different departments of similar size in England indicates that there is very little correlation between similar emergency departments in England.
CONCLUSION
Few data are available on staffing levels in individual emergency departments in the UK. This study has collected this information to enable individual departments to benchmark their own levels against national averages in order to plan future workforce developments. The survey shows that most departments rely on doctors at the SHO level to provide the majority of clinical care, although there is a trend towards increasing numbers of consultant and middle grade staff as departments get larger, but this relationship is not as strong for nursing staff. There is great variability in staffing numbers in similar sized departments, and most departments are understaffed in relationship to BAEM recommendations to achieve the 4 h target at the 90% level.
Supplementary materials
web only appendix 25/7/420
Files in this Data Supplement:
Footnotes
Funding: None.
Competing interests: None.
Linked Articles
- Primary survey